Article Text

Abstract
Background An understanding of the epidemiology of shoulder dislocation/subluxation in rugby union players could help develop targeted prevention programmes and treatment. We performed a multiyear epidemiological survey of shoulder dislocation/subluxation in a large cohort of rugby players.
Methods A descriptive epidemiological study was performed prospectively for five playing seasons (2008–2013) in all players licensed in the French Rugby Union. Rugby players were categorised into five groups by age. The player and the team physician reported the injury to the club insurance company if it occurred during training or a match. The goals of the study were to define the rate, type and causes of shoulder dislocation/subluxation.
Results 88 044 injuries were reported, including 1345 (1.5%) episodes of dislocation/subluxation in 1317 men and 28 women, mean age 22.5±5.9 years. About 10/10 000 men and 5/10 000 women reported an episode of shoulder dislocation/subluxation per season, including 83/10 000 senior professionals, 17/10 000 senior amateurs, 21/10 000 juniors, 12/10 000 cadets and <1/10 000 rugby school players. Shoulder dislocation/subluxation was significantly more frequent in senior and junior players (p<0.001). Injuries mainly occurred during a match (66%) in the middle of the season (44%). The most frequent playing position was forwards (56%) and the main mechanism was tackling (69%). When reported, the history of recurrence was found in 66% of injured players, fractures in 22% and acromioclavicular injury in 6.7%. Nerve injury was associated with shoulder dislocation in 6% of cases.
Conclusions Senior professionals and junior male forward rugby players with a history of shoulder dislocation/subluxation should receive special attention from sports medicine professionals and orthopaedic surgeons.
- Shoulder
- Sporting injuries
- Rugby
Statistics from Altmetric.com
Introduction
Rugby is practised more and more frequently in France, where the British introduced it around 1870. Since France organised the World Cup in 2007, the number of licensed members in rugby union has increased by 79% (http://www.ffr.fr/). Members of the ‘Rugby Union’ in our study must be distinguished from members of the ‘Rugby League’, which has different rules. The French Rugby Union (Fédération Française de Rugby or FFR) organises and manages the ‘Rugby Union’. The Ligue Nationale de Rugby (LNR) manages and organises the professional sector. Various types of games exist in Rugby Union: with XV, XII or VII players.
Rugby Union is a contact sport with more serious injuries than other sports.1 Junge et al2 showed that compared with a soccer player, a rugby player had a 1.5 times greater risk of injury during training and a 2.7 times greater risk during a match. Shoulder injuries represent 9–11% of injuries and 66% of the injuries to the upper limbs.3 In case of shoulder injury, acromioclavicular dislocation is the most frequent injury. However, dislocation and instability of the shoulder results in the longest time off the field in professional rugby players,4 which can also jeopardise a professional player's career. Brophy et al5 showed that prior surgery for glenohumeral joint stabilisation significantly reduces the length of a professional football player's career.
To the best of our knowledge, there are no studies that have specifically evaluated the epidemiology of post-traumatic shoulder dislocation/subluxation in a large cohort of rugby players at several levels of play. We aimed to describe the epidemiology of shoulder dislocation/subluxation in French rugby players: the rate, type and mechanisms of injury. The secondary goal was to describe the demographic characteristics of the injured players.
Methods
Study design and participants
We performed a prospective descriptive epidemiological study of a cohort of all the licensed players at the FFR for five consecutive seasons, from 2008/2009 to 2012/2013. All age categories and levels were included: senior professionals and amateurs (age >18 years for women and >19 years for men), juniors (only men, between >17 years and ≤19 years), cadets (between >15 and ≤17 years in boys, ≤18 years in girls) and rugby school players (≤15 years). All types of rugby were included: (1) XV, (2) XII, (3) XV or XII, (4) VII, (5) VII or XII. Patients were fully informed.
Data collection
Data were obtained from three sources:
Files from clubs affiliated with the FFR and licensed players: a license is necessary to play in a club, whatever the category, and all clubs must be affiliated with the FFR. Data included: the number of clubs affiliated per season, the number of licensed players per season by gender and category. The same player could be included several times if she/he was licensed for several seasons.
The files of the National Rugby League (NRL) for the number of professional players per season.
Prospective data collection organised by the insurance company of the Fédération Française de Rugby (FRF): all clubs affiliated with the FFR are insured by the same insurance company (Centre de Gestion Administratif Rugby). For coverage of medical costs, claims must be made for injuries that occur during rugby practice and matches whatever the topography and type of injury. Specific data were obtained by the investigating physician on a standardised form for each episode of shoulder dislocation/subluxation from the player and the club doctor, which was then entered into an Excel file. These data concerned the injured players (gender, age, socioprofessional status, category of game, level of play, type of game), the accident (position of the player and line of play, date of the accident, period of the season, during a match or training, phase of the game and existence or not of an infringement) and shoulder dislocation/subluxation (anterior or posterior, left or right, previous episode of shoulder dislocation/subluxation, complications and associated injuries).
Calculations and data analysis
We calculated the rate of reported episodes of dislocation/subluxation in relation to the number (1) of reported injuries in all locations combined (2) of licensed players by gender, age category and level. The positions occupied by the injured players were presented in two categories: the ‘Forward’ lines (first line including the right and left props, and the hooker and the second and third line) and ‘Back’ lines (scrum half, the fly half, the wing, the centre and the back). A rugby season was divided into three phases, the beginning of the season from August to October, mid-season from November to February and the end of the season from March to June. The first two seasons correspond to the regular phase and the last to the eliminatory phase in most categories. In the population of players who reported an episode of shoulder dislocation/subluxation, the χ2 test was used to compare (1) the distribution of the socioprofessional categories to that of the French population in 2011 published by INSEE (Institut National de la Statistique et des Etudes Economiques http://www.insee.fr/), (2) the distribution of the age and level categories to that of licensed FFR players. The Fischer exact test was used to compare the distribution and phases of the game involved in the episodes of shoulder dislocation/subluxation between ‘forwards’ and ‘backs’, then depending on whether the accident occurred during a match or training. When ‘tackling’ was involved, we used the χ2 test to compare the frequency of being tackled and tackling between the ‘forwards’ and ‘backs’. p<0.05 was considered to be statistically significant. Analyses were performed with STATA.V.10.
Results
During this period, more than 1730 clubs were affiliated with the FFR each season, from 1734 in 2008–2009 to 1843 in 2012–2013. During the five seasons studied, 88 044 injuries were reported, including 1345 episodes of shoulder dislocation/subluxation for a mean rate of 1.5%±0.5%. The mean rate of episodes of dislocation/subluxation in relation to all licensed players was 9.5±2.8/10 000, including 4.9±2.8/10 000 in women and 9.7±2.9/10 000 in men (table 1). During the rugby season, a mean 83 senior professionals, 17 senior amateurs, 21 juniors, 12 cadets and less than 1 rugby school player out of 10 000 players, respectively, reported an episode of shoulder dislocation/subluxation (table 2).
Rate of shoulder dislocation/subluxation in all players by gender
Rate of shoulder dislocation/subluxation by category (number of reported episodes of shoulder instability/number of licensed players)
The players who reported an episode of shoulder dislocation/subluxation were men in 97.9% of the cases (1317/1345), mean age 22.5±5.9 (from 5.9 to 58.1) years. The distribution of reported episodes of shoulder dislocation/subluxation by age was 3.1% (42/1345) of senior professionals, 65.3% (876/1345) of senior amateurs, 15.5% (209/1345) of juniors, 12.3% (166/1345) of cadets and 3.9% (52/1345) of rugby school players. The distribution into categories of players who reported an episode of shoulder dislocation/subluxation was significantly different from the distribution of licensed players p<0.001. In relation to the expected distribution by category, shoulder dislocation/subluxation occurred 7.8 times more frequently in senior professionals, 1.8 times more frequently in senior amateurs, 2.2 times more frequently in juniors, 1.3 times more in cadets and 12.3 times less in rugby school players (figure 1). All socioprofessional categories were found in the group of licensed rugby players; however, they included significantly more students than in the general population and there were no retirees, p<0.001 (figure 2). Rugby XV was the most frequent form of play (91.1%) followed by Rugby XII (5.6%), XV or XII (2.4%), VII (0.8%), then VII or XII (0.1%).

Graph of the age categories and levels of licensed FRF and players who reported an episode of shoulder dislocation/subluxation.

Socioprofessional categories of rugby players and the general population.
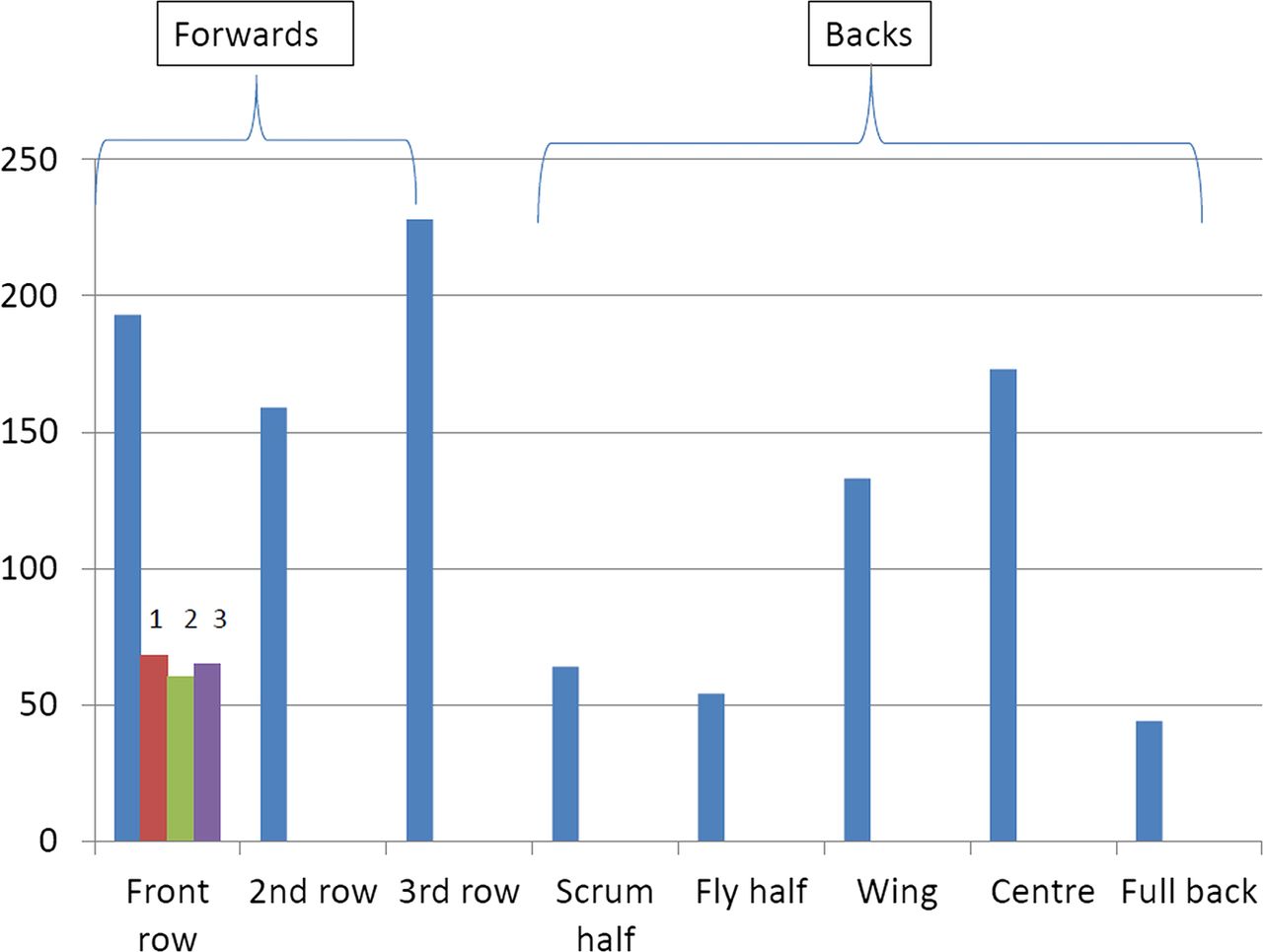
The playing position was recorded in 1048/1345 (77.9%) participants. Forwards were more frequent (580/1048 or 55.3%) than backs (468/1048 or 44.7%; figure 3). There were more third lines in the forwards and centres than in the backs. The reported episodes of shoulder dislocation/subluxation usually occurred in the middle of the playing season (43.7% vs 28.7% at the beginning of the season and 27.6% at the end of the season) (figure 4) and during matches (65.9% vs 27.9%). In 883 cases, the phase of the game and the position were recorded. The distribution of the phase of the game was significantly different depending on the position (back or forward), p<0.0001. The ‘tackle’ was the phase of the game involved in 68.8% of the cases, slightly more for backs than forwards (table 3). The ‘maul’ and the ‘ruck’ were significantly more frequent in forwards with an OR of 2.69 (1.67 to 4.35) and 15 (1.98 to 113.55), respectively (table 3). In the 608 tackle injuries, the detail of whether the player was tackled or tackling was reported in 182 players. There were more tackled (136/182=74.7%) than tackling (46/182=25.3%) injuries, except for professional players who were all tackling, and no statistically significant difference was found between forwards and backs for this criteria (p=0.20). In 97.8% of the cases, the injured players did not report infringement.
Distribution of reported shoulder dislocation/subluxation in relation to phases of play and forward or back playing positions

Distribution of positions in rugby players who reported an episode of shoulder dislocation/subluxation. 1—Right prop; 2—Left prop; 3—Hooker.

Distribution of reported episodes of shoulder dislocation/subluxation during the playing season.
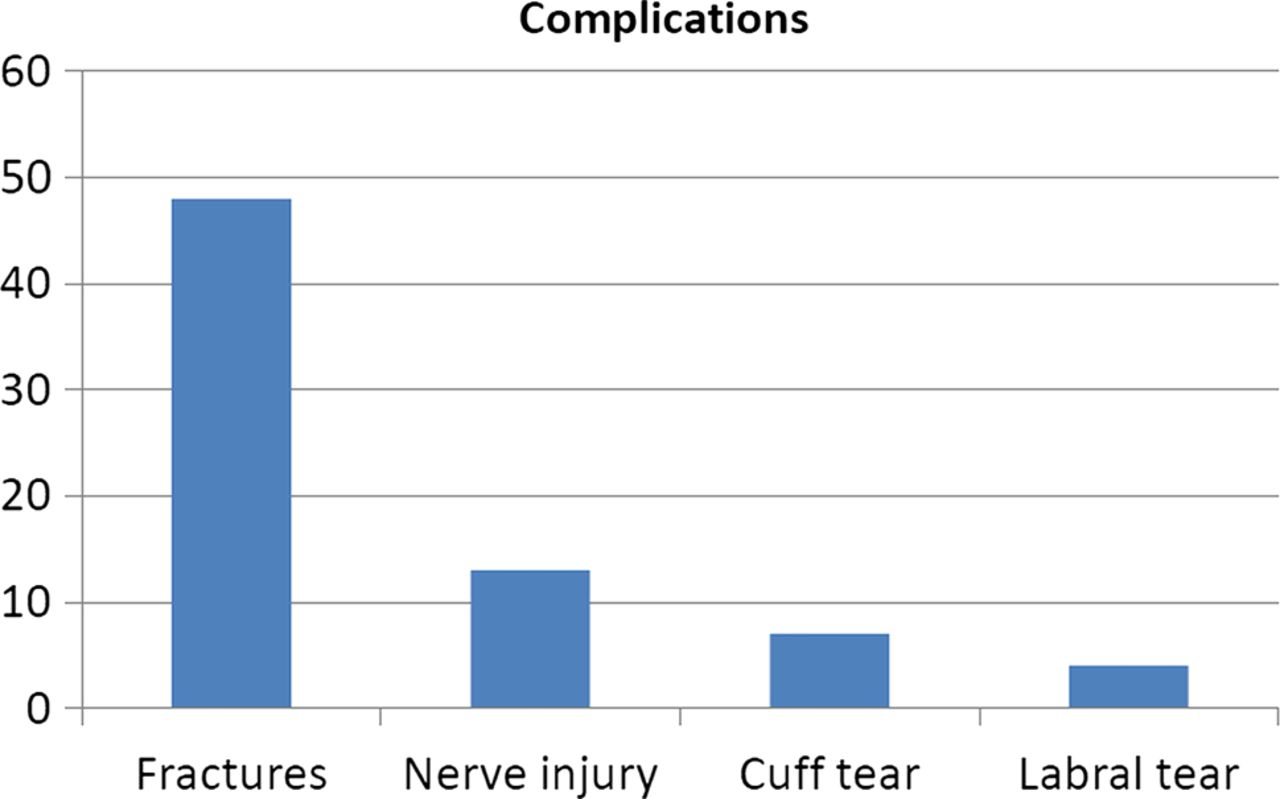
Among the 1345 episodes of reported dislocation/subluxation, 1201 (89.3%) were true dislocations, and 144 (10.7%) were subluxations, usually anterior (98.4%) both right (53.1%) and left (46.9%). The notion of recurrence was recorded in only 223 (16.6%) players and involved 147 patients or 65.9%. The presence or not of complications was reported in 215 (16%) patients and involved 70 players (32.6%; figure 5). Nerve injury was associated with shoulder dislocation in 13/215 (6%) patients. The presence or not of associated injuries was reported in 164 (12.2%) patients and involved 25 players (15.2%; figure 6).

Reported complications by players presenting with shoulder dislocation/subluxation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Associated injuries reported by players presenting with shoulder dislocation/subluxation.
Discussion
For five consecutive seasons, 1.5%±0.5% of injuries reported by the French Rugby Union players were episodes of shoulder dislocation/subluxation. The mean rate of shoulder dislocation/subluxation in relation to all licensed players was 4.9±2.8/10 000 in women and 9.7±2.9/10 000 in men. Senior professionals had the highest risk and rugby school players had the lowest risk of shoulder dislocation/subluxation.
The shoulder is a joint with the highest risk of dislocation during sports.6 In our study, the highest incidence was found in senior professionals, which is comparable to the results in the literature for all injuries.7 ,8 Indeed, the professionalisation of rugby union, which was decided by the International Rugby Board after the second world cup in 1995, resulted in an increase in the number of injuries of all types combined. The incidence of injuries went up from 1/3.4 matches in 1993–1994 to 1/2 matches in 1997–1998.9 In younger players, the lowest incidence was seen in rugby school players followed in increasing order by cadets, then juniors, which is comparable to the study by Palmer-Green et al.10 In a study including 210 British rugby players between <9 and <17 years of age, 39 (18.6%) were injured.11 The incidence and severity of injuries increased significantly with age. Head and neck injuries were the most frequent, followed by shoulder injuries, all pathologies combined.
Fewer women than men play rugby, but the number is increasing. In our study, women reported two times fewer episodes of dislocation/subluxation of the shoulder than male players. This is probably explained by the difference in speed and power during impact12 or by the fewer phases of tackling during the match in women's rugby. By order of frequency of injuries, the shoulder was in second position in men after the face and in third position in women after the knee and the ankle.13 In men, the most frequent diagnosis was cuts, followed by dislocations, and in women it was bruises and contusions followed by sprains.
The positions with the highest risk of injury seemed to be the third line in forwards and centres in the backs. These results extend those of Brooks and Kemp14 in a study analysing the incidence and severity of injuries, all locations and pathologies combined, according to playing position in a group of 899 English rugby union professionals. In our study, the tackle was the mechanism of injury in 68.8% of cases, which is similar to the study by Sundaram et al15 which identified the same mechanism in 66.3% of the 166 Australian players operated on for shoulder instability. The tackled player was more likely to suffer a shoulder dislocation than tacklers except for professional players as reported by Headey et al.4 We assume that the tackle is a demanding competence in rugby, and capacity to fall fair more perform by professional than non-professional players. The maul and ruck were significantly more frequent in forwards, which is not specific to shoulder injuries.16–18
Practical implications/rugby-specific insight
When a tackled player is injured, dislocation can occur during the fall. If the tackled player controls the fall this could prevent dislocation. Prevention should be based on learning a technique to protect the shoulder as it hits the ground with internal rotation, adduction and with the elbow against the body, while remaining pressed against the tackler. These techniques are taught during training in combat sports such as judo or wrestling.
If the injured person is the tackler, it is the phase when the shoulder is used to tackle that must be controlled. The shoulder is at risk of dislocation if the arm is in adduction and external rotation. To prevent dislocation, the player must be taught to tackle with the shoulder in adduction as well as internal rotation and antepulsion (or anterior elevation of the arm) to make sure that the glenohumeral joint muscles are locked.
Recurrent shoulder dislocation is high in rugby: in professional rugbymen, the rate is 62% and clinically more severe with a longer time out of play (115 vs 66 days)4 than for a primary dislocation. In a consecutive series of 198 rugby players who underwent arthroscopic repair for shoulder instability, 158 (79.8%) were recurrent.19 However, in a series of 34 rugby union players operated on for recurrent shoulder instability by the Latarjet-Patte method, 65% of the patients returned to playing rugby with no recurrence noted after a mean follow-up of 12 years.20 A systematic review of the literature has also shown a low rate of recurrent instability after the Latarjet procedure.21 In our study, recurrence was reported in 66% of the injured players. In a prospective 10-year study by Hovelius et al,22 the estimated rate of recurrent dislocation after 2 years was 47% in 12–22-year-olds, 28% in 23–29-year-olds and 13% in 30–40-year-olds. At 10 years, the rate of recurrence went down from 67% in 12–22-year-olds to 58% in 23–29-year-olds to 21% in 30–40-year-olds. In the literature, there is limited evidence regarding the comparative effectiveness of surgical and non-surgical treatment of traumatic anterior shoulder instability (TASI).23 In our study, the rate of recurrence history was high and we suggest assessing the efficacy of surgical treatment in rugby players at the first TASI.
Shoulder injuries are frequently associated with other injuries.24 According to the literature, the ‘unhappy or terrible triad’ consists of anterior post-traumatic dislocation of the shoulder associated with a complete rotator cuff tear and brachial plexus or axillary nerve damage.25 According to Neviaser et al,26 the incidence of nerve injury secondary to dislocation of the shoulder in the general population is 10.8% in patients aged over 40 years. For Blom and Dahlbäck,27 the frequency of these nerve complications is underestimated and is approximately 35% based on electromyographic tests. In our study, nerve injury was diagnosed in only 13/215 (6%) patients, which seems low, and it was probably underestimated in our group. Practitioners and healthcare providers must understand the importance of and be trained to identify these potentially severe injuries, before and after reduction of dislocation.
The incidence of rotator cuff tears associated with an episode of shoulder dislocation increases with age.28 Our study seems to confirm these data because in our series, with a mean age of 22.5 years, this occurred in a very low number of patients 7/215 (3.2%).
This study has several limitations. We reported the incidence in terms of the number of episodes of dislocation/subluxation in relation to the number of licensed players, while most authors report the number of injuries per 1000 player-hours, which may make it more difficult to compare our results to those obtained in other studies. The number of days off the playing field was not recorded, so the severity of the injuries could not be determined. This study is important because it presents a large body of data which include all of the licensed players of the FFR. Thus, we were able to evaluate the characteristics of 1345 dislocations/shoulder instabilities in rugby union players.
Summary and conclusions
The most important results of this study were: (1) 1.5% of reported accidents involved shoulder dislocation/subluxation, (2) there were two times fewer women than men, (3) senior professionals had the highest rate of shoulder stability of all licensed players, (4) the ‘tackle’ was the phase of play that was the mechanism of injury in half the cases, while the ‘maul’ and the ‘ruck’ were significantly more frequent in forwards than in backs, (5) when a history of recurrence was recorded, it involved 2/3 injured players and (6) when complications were reported, they involved 1/3 injured players, usually fractures and associated injuries in 1/6 of injured players, usually with acromioclavicular joint involvement and nerve injury.
What are the new findings?
Description of the epidemiology of dislocation/subluxation of the shoulder in male and female rugby union players as well as all age categories and levels.
Shoulder dislocation/subluxation is twice as frequent in men as in women.
It is most frequent in senior professionals and least frequent in rugby school players.
How might it impact on clinical practice in the near future?
Preventive measures should target men and professional players.
Prevention should focus on good rugby technique, especially during tackling.
Healthcare professionals should be trained and made aware of the importance of identifying associated nerve injury before and after reduction of shoulder dislocation.
Acknowledgments
The authors would like to acknowledge the contribution of the team of physicians who recorded injuries throughout this project. The authors would also like to thank Danièle Ballini from the Fédération Française de Rugby and Christine Arrault from CGA Colonna for their help in collecting data for this study.
References
Footnotes
Contributors YB was involved in orthopaedic and sport surgery, and was responsible for initiating, developing and coordinating this study. SK undertook statistical analysis, and wrote and submitted the manuscript. NL and SH were involved in orthopaedic and sport surgery, collaborating in clinical research for sport traumatology for this study. J-CP and J-PH provided data from the Fédération Française de Rugby. BD provided data from the Ligue Nationale de Rugby. AR was in charge of collecting data from patients.
Competing interests None.
Ethics approval Ethics approval for this study was received from the Comité de Protection des Personnes Ile-de-France VI (CPP IDF VI), Hôpital La Pitié- Salpêtrière.
Provenance and peer review Not commissioned; externally peer reviewed.