Article Text

Abstract
Background The IOC encourages international federations to establish systematic athlete injury and illness surveillance programmes.
Objective To describe pattern of injuries and illnesses during the 24th Men's Handball World Championship 2015 by implementing the IOC injury and illness surveillance protocol.
Methods The medical staff of participating teams (n=24) were requested to report all new injuries and illnesses during matches and/or training on a daily basis throughout the event (15 January to 1 February, 2015). Exposure (number of player-hours) during all matches was calculated for all players (n=384) and for each of the 4 player positions (wing, back, line and goalkeeper).
Results Medical staff of all teams submitted 96.7% (n=325) of the daily report forms. In total, 27.1% of the players were injured, and of the 132 injuries reported, 40% were time-loss injuries. The total incidence of injuries was 104.5 per 1000 player-hours. The highest risk of injury was found among line players, and more injuries occurred during the first half of the matches. The most frequent injury location was the ankle, followed by the thigh, knee and head/face. The majority of injuries were contusion, sprain or strain. In total, 10.9% of the players were affected by an illness during the event. Of the 42 cases recorded, 31 (73.8%) were reported as respiratory tract infection.
Conclusions The risk of injury in handball is high among Olympic sports. Preventive measures should focus on contusions, ankle sprains, and thigh muscle strains, as well as measures aimed to reduce upper respiratory tract infections.
- Handball
- Athlete
- Injuries
- Illness
- Prevention
Statistics from Altmetric.com
Introduction
Handball is one of the Olympic sports with the highest risk of injury, according to results from the IOC injury and illness surveillance system.1–3 The game is characterised by a high playing tempo, rapid changes of movement, jumps with hard landings, frequent contact and collisions between players, as well as repetitive knee and shoulder joint stress.4 Although rules exist to make the sport safe and fair,5 players are vulnerable for both acute and overuse injuries.
The risk of injury in handball is significantly higher during match play than in training, probably explained by higher intensity, more aggressive behaviour and more frequent contact between players.6–9 However, it is still unsure whether the risk of injury changes throughout the time course of the match, or if the risk of injury or pattern differs between player positions. Epidemiological studies have reported that, in general, the knee and ankle are the most common locations for acute injuries, while overuse problems primarily affect the knee, lower leg and shoulder.6 , 10 , 11 Epidemiological data in handball are mainly based on injuries among players on the national division level, as there are limited data on elite international players.
The IOC encourages international federations to establish systematic athlete injury and illness surveillance programmes,1–3 , 12 , 13 not only to provide important epidemiological data, but also to inform prevention strategies.14–17 The International Handball Federation (IHF) reported injuries that required medical attention from six major international handball tournaments 10 years ago (2001–2004) and found a total incidence of 108 injuries/1000 player-hours, corresponding to 1.5 injuries per match.18 Since then, the intensity of the game has increased substantially at the highest international level4; yet, no systematic monitoring of player health has been established.
To protect athletes’ health, not only to prevent injuries but also illnesses, the most recent epidemiological studies from the Olympic Games1 , 12 , 19 and the world championship in football,20 aquatics21 and athletics,22 have reported illnesses in their surveillance. There are no data on burden of illness among elite handball players in a tournament setting.
Therefore, we aimed to describe the pattern of injuries and illnesses during the 24th Men's Handball World Championship 2015 by implementing the IOC injury and illness surveillance protocol.
Methods
The methodology and procedures of this study were established according to the IOC injury and illness surveillance protocol.1 , 12 , 23
Injury and illness registration
Team doctors/physiotherapists of all participating teams (n=24) were requested to report all new injuries and illnesses during matches and/or training throughout the event (15 January to 1 February 2015). They were asked to complete and submit a standardised one-page report form daily with predetermined categories, definitions and codes (see online supplementary appendix), regardless of whether or not any injury or illness had occurred. This daily report form was submitted the following day to either the researchers present at the team hotels every morning (8–10 am), or to the local organising committee physicians working at any of the three competition venues athlete medical clinics. The team medical staff were invited to participate in the study and provided a booklet by e-mail 1 month prior to the event. They were also personally informed about the study in person at the first official team medical meeting in Doha on 15 January. Each team received a folder with all the necessary documents needed for the entire event.
A newly incurred injury was defined as any musculoskeletal complaint and/or concussion incurred in competition and/or training during the tournament that received medical attention, regardless of the consequences with respect to absence from competition or training. Recurrent injuries (injuries of the same location and type) were only reported if the athlete had returned to full participation after the previous injury. Pre-existing injuries and not fully rehabilitated injuries were not reported.
A newly incurred illness was defined as any physical complaint (not related to injury) incurred due to competition and/or training during the tournament that received medical attention regardless of the consequences, with respect to absence from competition or training. Chronic pre-existing illnesses were not included, unless there was an exacerbation requiring medical attention during the event.
For each injury, the reporting form included information about whether the injury occurred during training or match play (if so, match time), injury location, type of injury, cause of injury, and whether the player returned to the game, as well as the estimated severity reported as the time expected for complete return to play (days/weeks). For illness, the form included data on organ system/region affected, main symptom(s), cause and diagnosis, as well as the estimated severity. All definitions, categories and codes were given according to the IOC injury and illness surveillance protocol.1 , 12 , 22 , 23 The report form was available in six languages; English, Arabic, French, Spanish, German and Russian.
Exposure data
As each participating team (n=24) had 16 accredited players, 384 players were included in the study. To present the risk of injury as incidences, an exposure file was created in Excel (V.2010). The result of each match was extracted from the official IHF online database (http://www.ihf.info/IHFCompetitions/WorldChampionships/MensWorldChampionships/MensHandballWorldChampionshipQatar2015/FixturesandResults/tabid/6969/Default.aspx) and transferred to the Excel file. In total, there were 88 matches during the event, including the preliminary round (60), President cup (8), placement round (4), and finals (16). We calculated the number of player-hours throughout the event (7 players×1 h×number of returned report forms) and excluded missed time due to 2 min suspensions and red cards. Exposure was calculated for each of the four player positions, based on the most common team player formation; two wing players, three back players, one line player and one goalkeeper. We did not collect data on training exposure during the event.
Statistical analyses
The data were analysed using SPSS (SPSS for Windows, V.21.0, SPSS, Chicago, Illinois, USA). Descriptive data, that is, frequencies and proportions, were presented for subgroups, such as injury type, location, cause, circumstance and severity, as well as affected illness systems with following symptoms, causes and estimated severity. The injury incidence was presented as the number of match injuries per 1000 player-hours. A Z-test based on the Poisson model, was used to compare injury incidences between subgroups. Injury incidences and relative risks (RR) were presented with 95% CI, and a two-tailed p value ≤0.05 was considered significant.
Results
Injury incidence
Throughout the 18 days of the event, 325 of 336 daily report forms were submitted by team medical staff (96.7%).
In total, 132 injuries were reported. Of the 384 accredited players, 80 sustained one injury, and 24 players sustained two or more injuries, thus, 27.1% of the players suffered at least one injury during the event. The majority of injuries occurred during match play (n=122), while 10 injuries were reported during training sessions. The number of match injuries per 1000 player-hours was 104.5 (85.9 to 123.0) in total and 50.5 (37.6 to 63.4) for time-loss injuries, corresponding to 1.4 (95% CI 1.2 to 1.7) and 0.7 (95% CI 0.5 to 0.9) injuries per match, respectively. The highest risk of injury was observed for line players (table 1).
The total number of injuries reported (n=132), as well as match injuries only (n=122), match exposure (number of player-hours), and match injury incidence (injuries per 1000 player-hours) for each of the player positions
Injury pattern
More than half (61.3%) of all time-loss injuries (n=62) were reported as less severe injuries, leading to an estimated absence from full participation in training and match play for 1–2 days, while 33.9% (n=21) were moderate injuries, with an estimated absence between 3 days and 4 weeks. A total of three severe injuries (4.8%) were reported, leading to an expected absence of >4 weeks (table 2). Of all injuries reported (n=132), 58.3% were located in the lower extremities, mainly the ankle, thigh or knee, while 16.7% affected the upper extremities, mainly the shoulder or fingers/thumb (table 2). The remaining injuries were located on the head/face (12.9%) and back/ribs/pelvis/abdomen (12.1%). The most common injury type was contusion (38.6%, n=51), followed by sprain (23.5%, n=31) and strain (12.9%, n=17). Muscle strains affected mainly the lower extremities (88.2%), mainly the thigh (n=9) and groin (n=4), while most contusions were located in the face (n=9), thigh (n=9), knee (n=8) and lower back (n=7). Ankle sprain (n=21) was the most frequent specific diagnosis.
Number of injuries (n=132) related to body part injured and injury severity, expressed as the estimated time of absence from full participation in training and match play
Injury cause
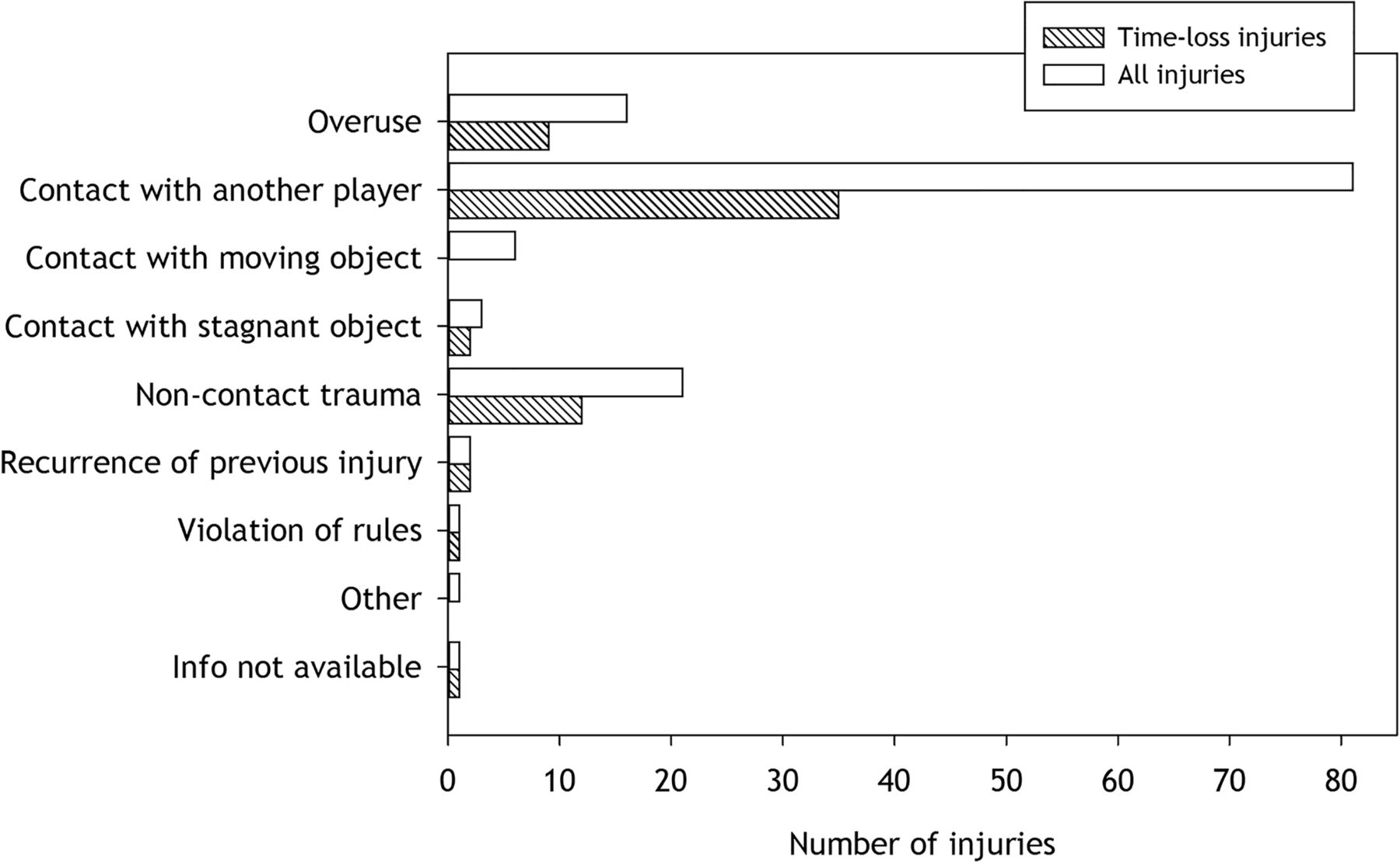
In total, more than half of all injuries (61.4%, n=81) were reported as the result of contact between players, while 15.9% were reported as non-contact trauma, and 12.1% were overuse injuries. Regardless of the main cause of injury, approximately half of the injuries were time-loss injuries (figure 1). Most injuries to the head/face (82.4%), knee (80%) and ankle (65.2%) were caused by contact with another player. No differences in injury pattern and injury causes were found between player positions.
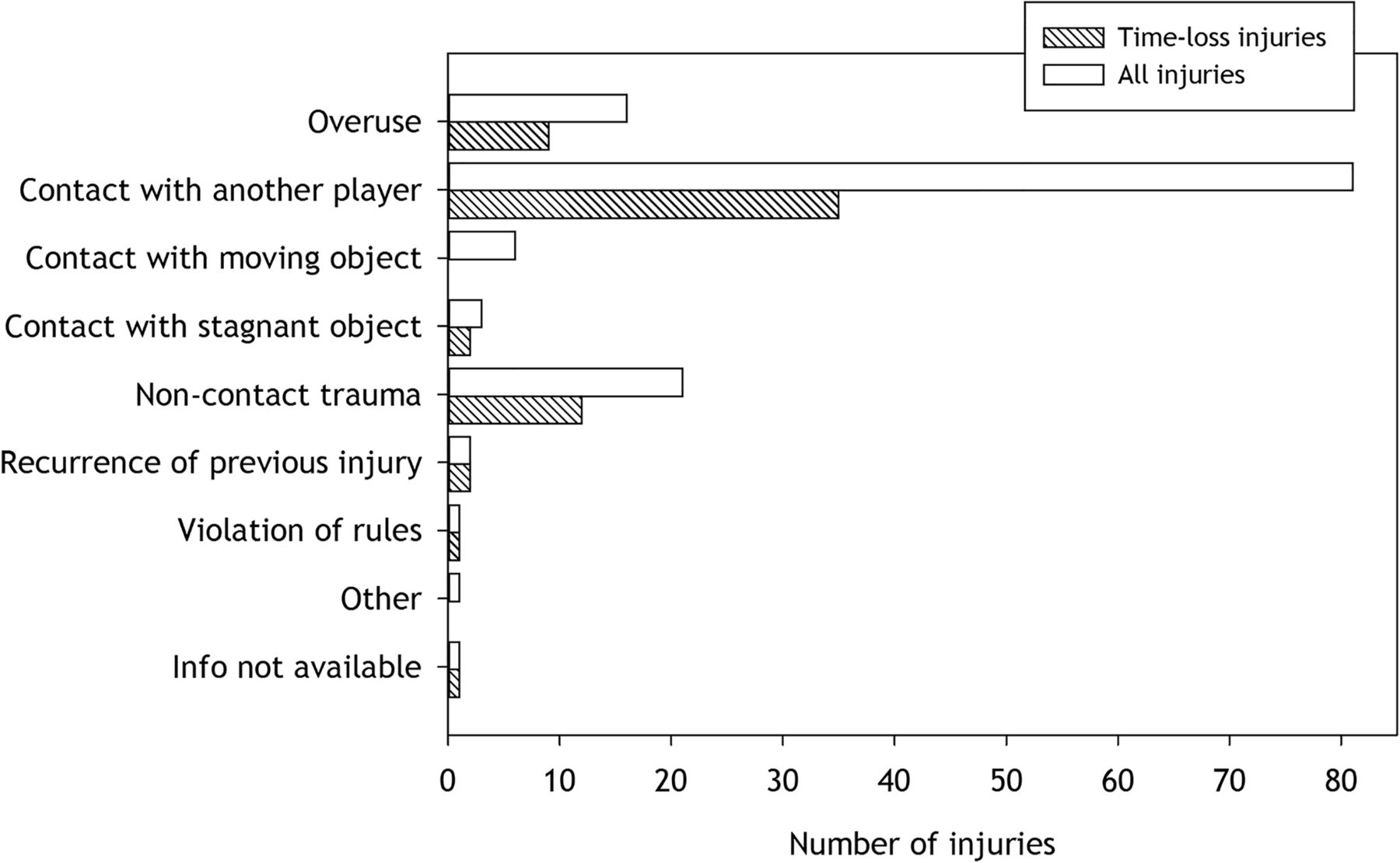
Number of injuries distributed according to injury cause for all injuries (n=132) and time-loss injuries (n=62).
Time of injury
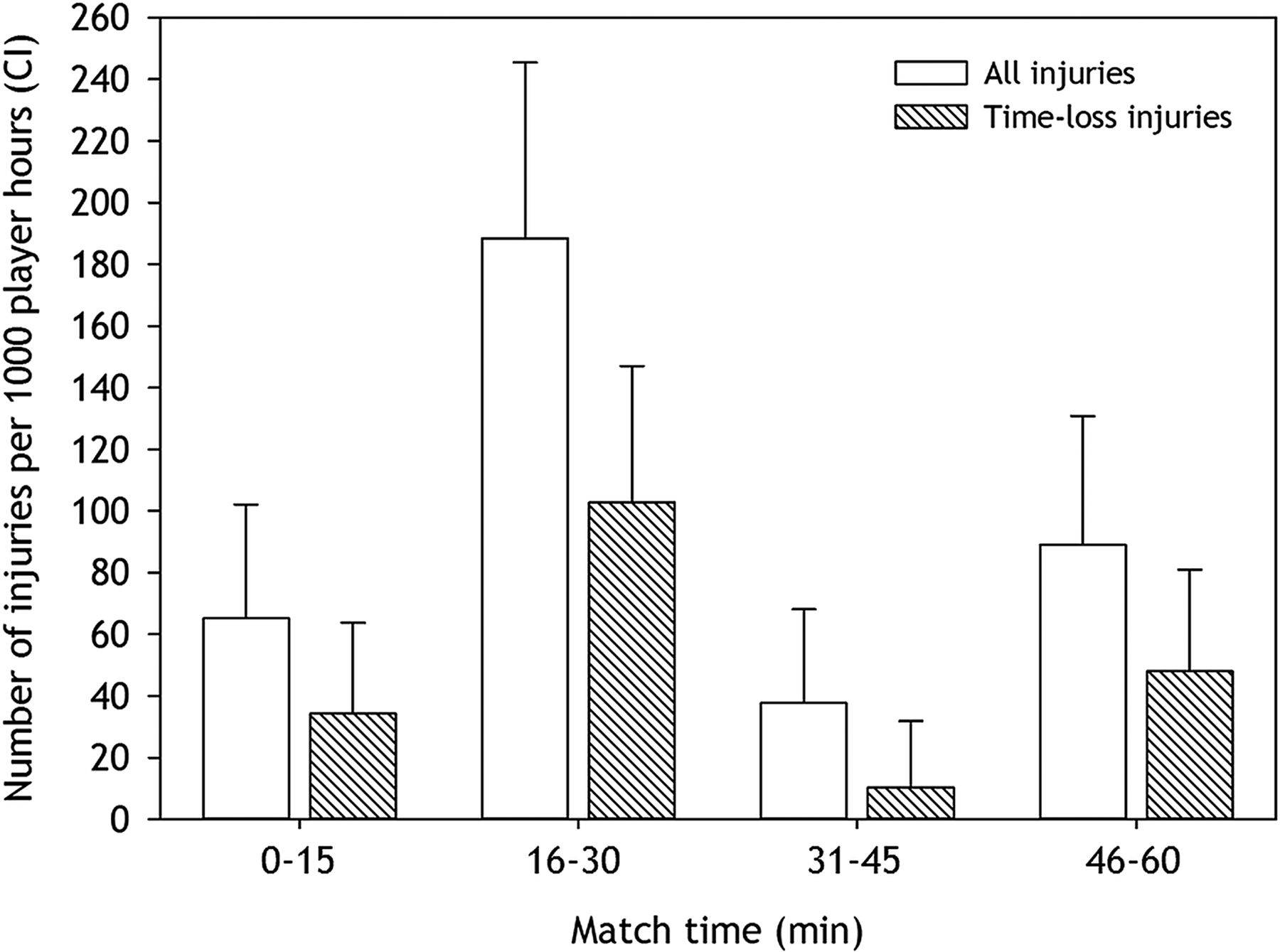
More injuries occurred during the first half of the match (0–30 min) compared with the second half (31–60 min): 126.7 (95% CI 97.8 to 155.6) versus 63.4 (95% CI 42.9 to 83.8) injuries/1000 player-hours, respectively (RR 2.0, 95% CI 1.35 to 2.97). The difference was even higher for time-loss injuries: 68.5 (95% CI 47.3 to 89.7) versus 29.1 (95% CI 15.3 to 42.9) injuries/1000 player-hours, RR 2.35, 95% CI 1.33 to 4.15). In total, the highest risk of injury was found in the second part of the first half (188.5, 95% CI 138.6 to 238.3), which was significantly higher than during the first quarter of the match (65.1, 95% CI 35.8 to 94.3), RR 2.89 (95% CI 1.72 to 4.88) (figure 2).
{kind=link}
{kind=link}
Injury incidences, expressed as the number of injuries per 1000 player-hours (with 95% CIs) for different time intervals (in min) of the match. Note: For 11 of the 122 match injuries, injury time was not reported.
Illnesses
The team medical staff reported 42 cases of illness during the event, 29 with a sudden onset and 13 with a gradual onset; thus, 10.9% of the players were affected by an illness during the tournament. While one-third (n=14) did not influence participation in training or match play, almost two-thirds (61.9%) resulted in an absence of 1–2 days. In one case, diagnosed as appendicitis, the estimated absence was more than 4 weeks. The respiratory tract (mainly upper) was the most commonly affected system (n=31, 73.8%), followed by the gastrointestinal tract (n=5, 11.9%) and dermatological problems (n=3, 7.1%). The main symptoms were pain, ache or soreness (n=25, 59.5%), fever, excess sweating or chills (n=6, 14.3%), and nausea, vomiting or diarrhoea (n=4, 9.5%). Infection was reported as the most frequent cause of illness (n=32, 76.2%). Other causes included nutritional, endocrine or metabolic disturbances (n=3, 7.1%), environmental conditions (n=2, 4.8%), and pre-existing disease (n=2, 4.8%). The most frequent diagnosis was tonsillitis (n=14, 33.3%) and common cold (n=10, 23.8%).
Discussion
This is the first study to describe both injuries and illnesses among players during a handball world championship. More than one in four players suffered from an injury during the event. Of the 132 injuries, contusions, ankle sprains and thigh muscle strains were most common. The highest risk of injury was observed among line players, and most injuries occurred towards the end of the first half of the match. Illness causing time-loss affected 7% of the players, and respiratory problems caused by infection were most frequent.
Risk of injury
We observed a total incidence of 104.5 match injuries per 1000 player-hours, which is lower than during the 2001 and 2003 Men's World Cup,18 but higher than that reported among men in the 2004 Olympics.3 Of the match injuries, about half were reported to cause subsequent time-loss, which corresponds to an incidence of 50.5 time-loss injuries per 1000 player-hours. This is substantially higher than previously reported.3 , 18 However, the response rate during the 2001 and 2003 Men's World Cup was less than 80%, and information about time-loss was not reported in 20% of the injury cases. A low response rate and missing data in previous studies could therefore explain the apparent discrepancy in match injury rates between studies. Conversely, the intensity of handball at the highest international level has increased substantially during the past decade,4 and this may have contributed to the secular trend for more time-loss injuries. In addition, several one-season cohort studies at the national level have suggested that the risk of time-loss injuries increases with increasing competitive level, most likely due to more intensive and faster play.6–9
Although the injury incidence in handball is higher than other team sports, including volleyball, basketball, rugby and football,3 , 20 , 24 , 25 the bulk of handball studies indicate that few of the time-loss injuries are severe, most leading to an absence from training and/or match play for only a few days. The current study confirms this, showing that severe injuries are rare; there were only three reported injuries expected to cause an absence of >4 weeks.
When do injuries happen?
There was a higher risk of injury during the first half of the match compared with the second half, and the difference was even higher for time-loss injuries. Within each half, the highest risk of injury was found during the last 15 min. This might be secondary to more intensive play and/or fatigue at these stages, indicating that conditioning programmes should be considered as injury preventive measures. These findings contradict previous studies reporting that most injuries occurred in the second half, and that time-loss injuries were equally distributed over the entire course of the match.3 , 18 , 26
Does player position matter?
More injuries occur while attacking than defending,6–8 meaning that most injuries occur when the team has ball possession and control in the opponent's half of the court. No previous studies from international handball tournaments have been able to address the risk of injury to the different player positions. Other epidemiological studies among national level players have reported more injuries among back players.27 , 28 However, these studies did not take exposure into full consideration. We distributed the total exposure time (player-hours) in accordance with the most common team player formation (3 back players, 2 wing players, 1 line player and 1 goalkeeper).
The highest total risk of injury was for players in the line position, followed by wings, backs and goalkeepers. For time-loss injuries, the risk was almost the same for line and wing players, also reported from a one-season cohort study among German male senior handball players.8 A high total risk of injury among line players may be explained by the diverse range of manoeuvres required in this position, for example, pivoting, frequent throwing, side-step cutting, jumping and landing, as well as constant contact with opponents and high involvement in counterattacks.4 However, as the player formation can vary between teams, and also within a team during a match, these results should be interpreted with caution.
The pattern of injuries
In total 58% of the injuries were located in the lower extremities, which is higher than previously reported from studies using similar methodology.3 , 18 The corresponding proportion from the 2001 and 2003 World Cup, and 2004 Olympics, was 44%, and most injuries were located in the knee, followed by the ankle and thigh. We report most injuries to the ankle, followed by the thigh and knee. In addition, those previous studies reported that 22% of all injuries were located in the head/neck, while our study found that head/face/neck injuries accounted for 15%.
The most recent injury epidemiological study in handball, performed during the 2010/2011 season among Danish male and female players,6 found the same injury pattern as the current study with ankle, thigh and knee as the most common acute injury locations. On the other hand, two small previous studies on injuries during international handball tournaments reported a high number of head injuries.29 , 30
These data suggest that the injury pattern has changed during the past 10 years, with fewer knee and head/face injuries, but more ankle and thigh injuries. This may also explain why we found fewer contusions, but more joint sprains and muscle strains than previously reported.3 , 18 The handball community has implemented warm-up programmes, aimed at improving running, landing and cutting technique, as well as neuromuscular control, balance and strength during the past years to prevent lower extremity injuries, especially knee injuries,28 , 31–33 but we do not know to what extent these are being used by top-level male handball players. In addition, stricter judging by the referees5 may have resulted in more fair play and fewer contusions due to inappropriate contact between players.
How do injuries happen?
Handball is a contact sport, and opponent contact is a normal part of the game. However, inappropriate contact and collisions between players contributes to acute injuries.6–9 Injuries can be caused by a direct blow to the body, for example, during collisions between players, or by being pushed or held by an opponent, which may put the player off balance, indirectly causing the injury. While 80–90% of all injuries during the 2001 and 2003 Men's World Cup, and the 2004 Olympics, were reported as contact injuries,3 , 18 we found that 60% were caused by player contact. Interestingly, while previous studies reported that half the contact injuries were caused by foul play, rule violation was very rare in this current study. It is reasonable to assume that more fair play reduced careless tackles and collisions that led to injury. However, injuries usually happen fast and abruptly and often involve several players, both opponents and team mates. It is therefore not easy for witnesses to accurately describe the injury mechanism. To obtain more accurate information on how injuries happen, systematic video analysis of real injury situations is an important tool34 and has been used to describe non-contact ACL injury mechanisms in more detail.35–38 Basing on this current study, it would be interesting to use a similar approach to analyse the mechanisms of contact injuries to the head/face, knee and ankle, as well as thigh muscle injuries.
Illnesses
This is the first study to provide detailed information on the burden of illness among elite handball players in the tournament setting. Illnesses among handball players were recorded for the first time during the 2012 Olympics;1 7% of Olympic handball players were affected during the event. In the current study, 10.9% of the players were affected by an illness, which resulted in subsequent absence from training and/or match play in two-thirds of cases. Similar to the Olympics,1 and also the World Championship in football,20 aquatics21 and athletics,22 the most frequently affected system was the respiratory tract, caused by infections. We can only speculate as to why infections and respiratory problems are the most common illnesses. During major international sports tournaments, athletes are exposed to crowded venues and a compressed training and match schedule, as well as environmental conditions, which they may not be used to. A systematic approach to illness prevention may help to reduce the number of respiratory problems. After implementing preventive measures, such as general guidelines on illness prevention, screening for airway problems, a vaccination programme, and specific measures to minimise the risk of infection, Hanstad et al 39 reported a reduced rate of illness in the Norwegian Olympic team in Vancouver 2010 compared with the team in Turin 2006.
Methodological considerations
The IOC injury and illness surveillance protocol was successfully implemented during the event with a response rate of 96.7%. To test the internal validity and accuracy of the data provided by team medical staff, we were able to compare the report forms submitted with information from two other sources; report forms completed by the local organising committee (LOC) physicians working at the players’ clinic in each of the three competition venues and hospital encounters for players who were transferred there. After cross-checking the injury and illness information obtained from the three different sources, we found three injuries and one illness case that were seen in the hospital, but not by the team medical staff or the LOC physicians. This demonstrates that, like any surveillance programme, the results presented must be considered as minimum estimates of injury and illness incidence.40
Although high compliance and accurate data reporting indicate that the surveillance system was feasible and accepted by the team physicians and physiotherapists, we do not know whether they all had the same reporting threshold. The team medical staff had different experiences of reporting; some had participated in the Olympics and were familiar with the system, while others had no previous experience. Thus, how the definitions of injury and illness, as well as the given categories and codes were interpreted, may have influenced the results.41How close the medical staff are to the player and how much knowledge they have about the player's medical history, may also influence whether they decide to report the occurrence as an injury/illness or not.
Epidemiology of overuse injuries is not as mature as that of acute injuries.42 We found that overuse problems accounted for 12.1% of all injuries. This is most likely an underestimate of the true magnitude of overuse problems in this elite player population. A study on world-class beach volleyball players documented that while a ‘traditional’ cohort study approach using a time-loss definition of injury suggested that risk of injury was very low, a concurrent survey of pain problems in the shoulder, knees and lower back demonstrated that overuse injuries were highly prevalent.42 The same can be expected in our player cohort.10–11 , 43 To obtain a more valid picture of overuse problems among players, the Oslo Sports Trauma Research Centre Overuse Injury Questionnaire has been developed,44 but this approach is not easily implemented in an international event setting.
Summary
The IOC injury and illness surveillance protocol was successfully implemented during the 2015 Men's Handball World Championship, with a response rate of 96.7%. The risk of injury in male elite handball is high among Olympic sports. Preventive measures should focus on contusions, ankle sprains and thigh muscle strains, as well as measures aimed to reduce upper respiratory tract infections.
What are the new findings?
-
The risk of injury in elite handball is high.
-
Line players display the highest incidence of injury.
-
More injuries occurred during the first half of the matches.
-
Illness is common, mainly respiratory problems.
How might it impact on clinical practice in the near future?
-
Preventive measures should focus on contusions, ankle sprains and thigh muscle strains, as well as measures aimed to reduce upper respiratory tract infections.
Acknowledgments
The authors would like to sincerely thank the IHF senior management, all team medical staff members and local organising committee physicians for their outstanding cooperation and contribution to the injury and illness surveillance project throughout the entire 2015 World Championship.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
-
Twitter Follow Juan Manuel Alonso at @DrJuanMAlonso, Arnlaug Wangensteen at @arnlaugw, Arnhild Bakken at @phbakken and Hendrik Dijkstra at @DrPaulDijkstra
-
Contributors All authors contributed to the study design and data recoding preparation. TB, J-MA, AW and AB were responsible for the data collection and data analysis. TB and RB interpreted the data and wrote the first draft of the paper. All authors contributed to the final paper. TB, J-MA and NP are responsible for the overall content as guarantors.
-
Competing interests None declared.
-
Ethics approval The study has been reviewed and approved by the Anti-Doping Lab Qatar (ADLQ), Doha, Qatar.
-
Provenance and peer review Not commissioned; externally peer reviewed.