Article Text

Abstract
Background Rock climbing is an increasingly popular sport worldwide, as a recreational activity and a competitive sport. Several disciplines including sport climbing and bouldering have developed, each employing specific movements and techniques, leading to specific injuries.
Objective To examine risk factors and prevention measures for injury in sport climbing and bouldering, and to assess the methodological quality of existing studies.
Methods 12 electronic databases and several other sources were searched systematically using predetermined inclusion and exclusion criteria. Eligible articles were peer-reviewed, based on primary research using original data; outcome measures included injury, morbidity or mortality in rock climbing, and included one or more potential risk factor or injury prevention strategy. Two independent reviewers assessed the methodology of research in each study using the Downs and Black Quality Index. The data extracted is summarised, and appraisals of the articles are presented with respect to the quality of evidence presented.
Results 19 studies met the inclusion criteria, and introduced 35 possible risk factors or injury prevention measures in climbing. Age, increasing years of climbing experience, highest climbing grade achieved (skill level), high climbing intensity score (CIS) and participating in lead climbing are potential risk factors. Results regarding injury prevention measures remain inconclusive.
Discussion This field is relatively new and, as such, the data are not as robust as for more established sports with a larger research foundation. The key need is establishing modifiable risk factors using prospective studies and high quality methodology, such that injury prevention strategies can be developed. The CIS may be a useful measure in this field of research.
- Sport climbing
- Rock climbing
- Risk factor
- Review
- Prevention
Statistics from Altmetric.com
Introduction
Rock climbing is a popular sport worldwide, as a recreational activity and as a competitive sport. Several disciplines of the sport exist, including traditional climbing, sport climbing and bouldering.1 , 2 Sport climbing and bouldering, the newest disciplines, can be performed on artificial surfaces as well as on natural rock. Sport climbing routes are typically up to 30 m high. The climber is attached to a rope clipped onto permanent bolts using ‘quickdraws’, spaced intermittently from the bottom up (lead climbing), or the rope is anchored at the top of the climb (top roping), to allow climbers to incur frequent falls safely. Bouldering uses crash mats instead of ropes to protect climbers from falls. ‘Boulder problems’ are usually short and low to the ground.
As sport climbing and bouldering employ specific movements and techniques, these two climbing disciplines lead to specific injuries. Previous research, involving primarily adult populations, suggests that upper extremity overuse injuries and acute flexor tendon pulley strains of the fingers are the most common injuries sustained by rock climbers in varying disciplines, though ankle injuries are also common due to falls.3–9 There have been no reviews examining specific risk factors for injury in sport climbing and bouldering. By identifying potentially modifiable risk factors for these injuries, it may be possible to develop and evaluate injury prevention strategies. We systematically reviewed intrinsic and extrinsic risk factors, and prevention strategies, for injury in sport climbing and bouldering.
Methods
Information sources
Twelve electronic databases were searched systematically for relevant documents during November 2012, and the search was updated in December 2014; the databases included: PubMed (1960–present), MEDLINE (OVID) (1946–present), SPORTDiscus (1960–present), BIOSIS Previews (1980–present), CINAHL Plus (1960–present), Academic Search Complete (EBSCO) (1960–present), PsychInfo (1967–present), ScienceDirect (Elsevier) (1960–present), Health STAR (1980–present), EMBASE (1974–present), SafetyLit (http://www.safetylit.org) and Statistics Canada (http://statcan.summon.serialssolutions.com). Four websites were searched for additional relevant publications: the UIAA (http://www.theuiaa.org), the International Federation of Sport Climbing (IFSC) (http://www.ifsc-climbing.org), the Alpine Club of Canada (ACC) (http://www.alpineclubofcanada.ca) and The Alpine Journal (a flagship publication of the ACC). Articles were also obtained from a comprehensive collection provided at the annual 2012 Banff Climbing Conference. Bibliographies of selected articles were searched for additional relevant publications. The terms used for article extraction are found in table 1.
Medical subject headings and text words used for article extraction
Search strategy
Climbing search terms: 1 OR 5 OR 6
Injury search terms: 2 OR 3 OR 7 OR 8
Risk factors: 4
Injury prevention search terms: 9 OR 10 OR 11
-
climbing and injury
-
climbing and risk factors for injury
-
climbing and injury prevention
-
climbing, risk factors for injury and prevention
Search terms for climbing, injury, risk factors and injury prevention were not searched individually as they each yielded a high number of articles that were not specific to the topic of interest. Strategies A to D were used to search each electronic database. If fewer than 300 articles were obtained, titles were screened, abstracts reviewed to retrieve relevant articles and duplicates removed. Finally, the full texts of the remaining articles were reviewed to assess eligibility based on the inclusion and exclusion criteria.
Eligibility criteria
Study inclusion criteria were: articles based on primary research using original data; outcome measures included injury, morbidity or mortality in rock climbing (indoor or outdoor); and one or more potential risk factor or injury prevention strategy; designs included randomised controlled trials, quasi-experimental, cohort, cross-sectional, case–control, longitudinal and case series studies—peer reviewed and published in English. Review articles and case studies were excluded; however, reference lists of review articles were reviewed for additional relevant articles.
Two independent reviewers completed the review of selected articles during December 2012, and again in December 2014 for the additional articles. Each reviewer screened the full-text articles to determine whether all inclusion criteria were met. Disagreements were resolved by discussion and subsequent consensus.
Data collection process
Descriptive data were extracted from studies that met all inclusion criteria. Study design, population, definition of injury, injury incidence, risk factor(s) examined and results were extracted (see online supplementary table S2). Risk factors and prevention measures for sport climbing were considered separately from those examined for bouldering, though not all articles were specified, and thus discipline could not always be isolated. Injury incidence was examined to give context to the risk factor analysis (table 2). Two independent reviewers assessed each study using the Downs and Black criteria for methodological quality. Downs and Black includes a 27-item checklist for randomised and non-randomised study designs. It aids in evaluating the quality of reporting, external validity, internal validity and power.22 The reviewers reached consensus for each article. The Oxford Centre for Evidence-Based Medicine Levels of Evidence were also determined for each study.23
Reported injury incidence proportions or incidence rates for all reviewed studies
Data synthesis
Due to the diversity of objectives, methodology and statistical analyses in these studies, meta-analyses to calculate injury rates or to quantitatively establish risk factors and prevention measures were not appropriate to carry out for this review. Therefore, extracted data are descriptive. Relevant data are summarised, and appraisals of the articles are presented with respect to the quality of evidence presented.
Results
Study selection
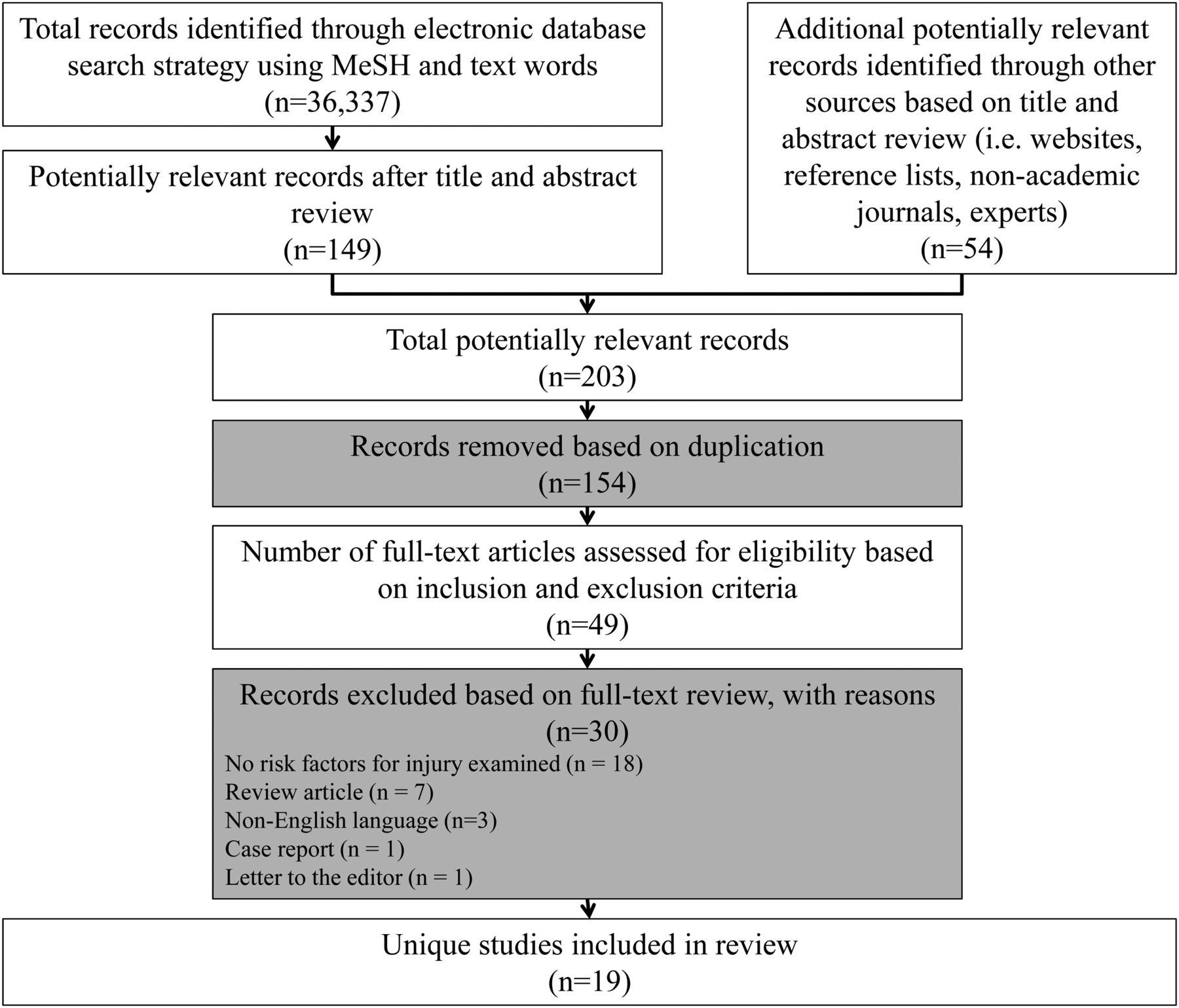
Titles and abstracts from database searches (n=149) and other sources (ie, websites, conference, bibliographies) (n=54) were screened for inclusion, and duplicates removed. The full texts of 49 articles were reviewed to assess each for eligibility; 19 studies met the inclusion criteria. Figure 1 summarises the study selection process.
{kind=link}
Study selection process based on inclusion and exclusion criteria. MeSH, medical subject headings.
Methodological quality assessment
Study appraisal based on the Downs and Black criteria produced scores ranging from 6 to 15 of 32 possible points (see online supplementary table S1). Overall quality was low, as the majority of the studies were cross-sectional (n=16). Furthermore, though the disciplines of sport climbing and bouldering were the focus of this review, results were included from studies that did not specify the type of climbing examined, as it was likely that they included sport climbing and bouldering, among others. Often, all ‘rock climbers’ willing to participate were included in a study, and some samples may therefore have been less representative of the target population being examined for this review. The authors thought it better to include rather than exclude these studies and risk overlooking potential risk factors. Age ranges varied, and there was sex disparity in most studies, with samples composed of approximately 60–100% males.2 , 15 Several studies failed to adjust for confounding variables, introducing potential bias in the results. Study quality scores and the Oxford Centre for Evidence-Based Medicine Levels of Evidence are summarised in online supplementary table S1.
Injury incidence
Reported proportions and rates of injury in rock climbing are not easily compared due to varied injury definitions, methodologies, reporting characteristics and contexts of each study (table 2). Backe et al 16 estimated the injury incidence rate (IR) to be 4.2 injuries/1000 participation hours in climbing. The career incidence of injury ranges from 1.52 injuries/subject to 4.24 injuries/subject for a general population of rock climbers.10 , 24
Risk factors
The 19 studies introduced 35 possible risk factors or injury prevention measures, though 19 of these were examined uniquely in single studies.
Intrinsic risk factors
Sex
Twelve studies examined sex as a potential risk factor for injury in sport climbing, bouldering, or both. Results were conflicting; six studies found no difference in injury risk between sexes,2–5 , 18 , 21 while four found that males were at greater risk than females.8 , 12 , 16 , 19 Schöffl et al 20 conversely found that the IR of injury was 0.54/1000 competition hours for males, and 0.97/1000 competition hours for females. Nelson et al 17 found that females were at higher risk of sprain and strain injuries, while males were at higher risk of lacerations and fractures. Study quality scores were similar for all studies, however, Backe et al 16 scored highest, at 15/32, for their cross-sectional study, and had the second largest sample size, with 355 participants. Neuhof et al,4 who, conversely, found no difference between sexes, had the largest sample size at 1962, and scored 12/32.
Age
Age was investigated as a possible risk factor in nine studies. Five reported that injury risk was not associated with age.3 , 4 , 8 , 13 , 18 However, most of these studies covered a broad age range, with Downs and Black methodological quality scores between 11 and 13/32. Sample sizes ranged from 29 to 1962 participants. Carmeli et al 12 reported finding significantly more hand and finger injuries (p<0.05) and a higher incidence of tendonitis in the long flexor tendons of the second and third fingers for those 19–34 years of age versus those aged 9–18 years, though their study only included 19 participants. However, Pieber et al,19 whose sample size numbered 193, found that, similarly, their two older age groups (29.5±1.7 years and 39.7±5.6 years) sustained significantly more injuries (p=0.021) than the younger climbers (23±2.4 years), and Rohrbough et al 5 found that, of 42 climbers, those suffering from A2 pulley pain were significantly older (30.7±8.2 vs 22.6±5.9 years, p=0.004). Conversely, Backe et al,16 who again scored highest on methodological quality at 15/32 and used a sample of 355 participants, found that the risk of reinjury increased for the adolescent age group, as opposed to older climbers (p=0.003 for 20–45 year-olds, and p<0.001 for +46-year-olds compared with <20-year-olds). However, their sample in this study was predominantly between 22 and 45 years.
Years of experience
Total years of climbing experience were examined as a risk factor in seven studies. Three found the number of years of climbing participation to have no significant impact on the risk of injury,2 , 3 , 16 while four found this factor to be a significant predictor of injury.4 , 5 , 8 , 18 Wright et al 8 found higher injury rates in climbers with over 10 years of experience (p=0.006), as did Hasler et al 18 (p=0.006), though both of these studies analysed prevalence only. Similarly, Neuhof et al 4 found higher injury rates for climbers with over 5 years of experience (p<0.01). Finally, Rohrbough et al 5 found that history of medial epicondylitis increased with increasing experience (p<0.0005), though these authors found no impact by experience on any other injuries.
Difficulty (skill) level
Eight studies investigated the highest difficulty level at which the subject could climb, a measure of skill level, as a risk factor for injury. Three studies found no significant impact on injury,2 , 5 , 13 with study quality scores between 11 and 12/32 and sample sizes ranging from 29 to 152 participants. Five studies found a difference, though Gerdes et al 14 did not analyse this statistically.3 , 4 , 8 , 15 Though the latter studies differed in their populations, all found that, in general, participants who climbed at higher grades reported more injuries. Sample sizes varied between 201 to 1962 participants, though study quality scores ranged from 7 to 12/32.
Body mass index (BMI)
Body mass index (BMI) was examined in three studies. Josephsen et al 2 and Neuhof et al 4 reported no significant difference in injury risk associated with this factor. However, Backe et al,16 who scored higher on methodological quality than either of the other studies (15/32 vs 12/32 for both of the former studies), found that higher BMI was significantly associated with a higher risk of injury (p<0.015), and of reinjury (p=0.121).
Body weight
Only two studies examined weight as a risk factor, and neither found any significant association with injury.2 , 13 However, because these studies examined different populations (Schlegel et al's study included only young, elite rock climbers, and Josephsen et al's, active boulderers), it is difficult to hypothesise the effect of body weight on injury.
Grip strength
Grip strength in relation to injury risk has only been examined in two climbing-specific studies to date; Schlegel et al 13 (Downs and Black score: 13/32) measured grip strength at 90° of elbow flexion in 29 climbers, and found that it did not significantly affect the risk of injury (p>0.05), though Carmeli et al 12 (Downs and Black score: 11/32), who measured at 90° of shoulder flexion with a straight elbow in 19 climbers, found a “mild to moderate correlation” (p<0.05).
Extrinsic risk factors
Lead climbing and top roping
Lead (sport) climbing was investigated in five studies.1 , 4 , 8 , 15 , 14 Most of these articles compared it to top roping, though two also compared it to bouldering, and a third included bouldering, traditional climbing and free soloing (free soloing is a type of climbing where no ropes, harnesses or any other protective gear are used, and therefore falls would likely be fatal). Four of these studies suggested that lead climbing was a risk factor for injury.1 , 4 , 8 , 14 Schöffl et al, who did not conduct a statistical comparison, noted the injury IR for lead climbing to be 0.29 injuries/1000 h, versus 1.47/1000 h for bouldering (and 0 for speed climbing, a third competitive discipline). Methodological scores ranged from 7 to 12/32 for these studies, though sample sizes were large; Gerdes et al,14 for example, with 1887, and Neuhof et al 4 with 1962 participants. Shahram et al 15 were the only authors who found that lead climbing was not associated with injury, though this conclusion was based on prevalence proportions, as incidence and risk were not captured in their study. Methodological quality was also low for this study (7/32), and the sample size comprised 50 climbers.
Climbing volume
The amount of time spent climbing (per week or per year) was examined in three studies.4 , 13 , 16 Backe et al,16 who scored highest on methodological quality at 15/32, found that the total climbing time each year did not have a significant effect on injury for their 355 participants, though the authors did control for exposure hours in their injury IR. Schlegel et al,13 whose study scored 13/32, found the same results when examining injury and hours per week spent climbing, though they included only 29 participants. Conversely, the study by Neuhof et al 4 found that climbing volume per week did significantly increase the risk of injury for their 1962 participants during summer (p<0.01) as well as winter months (p<0.01), though they did not indicate whether indoor climbing, outdoor climbing or both were examined (Downs and Black score: 12/32). Similarly, Jones et al 3 investigated the frequency of climbing (times per year) for each subject, and also found that as the frequency per year of outdoor (lead) sport climbing, indoor (lead) sport climbing and bouldering increased, so did the incidence of overuse injury.
Climbing intensity score (CIS)
A climbing intensity score (CIS) was used in two studies to examine degree of exposure to ‘climbing stress’ as a risk factor.9 , 19 CISs, introduced by Logan et al,9 and used again by Pieber et al,19 indicate the climbing intensity and volume by multiplying the average grade of climbing by the mean number of climbing days per year. Both studies found participants who scored higher in climbing intensity to be at a higher injury risk. Logan et al 9 (Downs and Black score: 10/32) compared an injury group to a non-injury group and found the mean CISs in the injury group to be significantly higher (p=0.01). Pieber et al 19 (Downs and Black score: 12/32) split the CIS into tertiles (CIS 1: 398±232 points; CIS 2: 1526±461 points; CIS 3: 5088±2701 points) with 56 participants per group, and found groups two and three to be significantly different from group one, which scored lower on the CIS (p<0.001).
Indoor versus outdoor climbing
Two studies investigated outdoor climbing compared to indoor climbing as a predictor for injury. Josephsen et al 2 (Downs and Black score: 12/32), who examined bouldering specifically in 152 participants, suggest a significantly higher risk of finger injuries outdoors, but a higher risk of fall-related injury indoors. Gerdes et al 14 (Downs and Black score: 9/32), who examined sport climbing, traditional climbing, bouldering and free soloing, observed an approximately even distribution of injuries indoors and outdoors in their 1887 participants. However, traditional climbing is rarely performed indoors and free soloing is performed exclusively outdoors, thus introducing a potential bias. It is likely that outdoor injuries would be over-represented for the purposes of this systematic review, since the focus here is on sport climbing and bouldering.
Influence of drugs/alcohol
Only two articles studied the influence of drugs or alcohol on climbing injury, and these yielded different results. Gerdes et al 14 (Downs and Black score: 9/32) found that substance use significantly increased the potential for injury in their 1887 participants, while Hasler et al 18 (Downs and Black score: 13/32) found no significant increase in risk in their 113 participants.
Other risk factors
A number of different risk factors were examined uniquely in single studies (see online supplementary table S1), including: wall height,11 average boulder height,2 maximum boulder height,2 history of injury,2 on-sighting (climbing a route for the first time),18 self-reported readiness for risk,18 lean body mass,13 increase in climbing difficulty per year,13 start age (of climbing),13 performing regular one-finger climbing,13 capsular thickening of finger joints,13 radioulnar instability of finger joints,13 Beighton score,13 number of years climbing at the elite level,5 handedness15 and climbing in a familiar versus new location.14
Prevention measures
The self-reported use of a warm-up and different lengths of warm-up were investigated in three studies, and no significant difference in injury was found between groups.2 , 10 , 11 Stretching prior to climbing was reported to be significantly associated with overuse injury by Tomczak et al 10 (Downs and Black score: 7/32). However, their claim that their “‘P’ value of 0.9763 [meant] that 97% of all people who reported stretching prior to climbing reported an overuse injury of some type” is incorrect. It is possible that a value of 0.9763 is instead a correlation coefficient, in which case this would suggest a strong association between stretching and overuse injuries. Conversely, Josephsen et al, who scored higher on methodological quality (12/32), found no significant difference in injury risk between those climbers who stretched versus those who did not. These authors also examined regular participation in yoga as a preventative measure and found the same results.2 Imposing strict regulations regarding equipment use and instructor presence was not found to significantly decrease the risk of injury in sport climbing or bouldering, nor was the presence or number of safety mats used, nor the number of spotters.2 , 11 Josephsen et al also investigated the taping of fingers and wrists, taking glucosamine and other supplements, heating hands prior to climbing, taking time off to prevent injuries, the use of corticosteroid injections, and weight training as potential preventive measures. Of these strategies, only taping wrists and weight training were found to be significantly associated with a decreased rate of injury.2
Discussion
In previous studies, older age, a higher number of years of climbing experience, higher climbing skill level, higher CIS, and lead climbing, were found to be risk factors. However, the reviewed studies differ in injury definitions, study populations and methodological quality, resulting in variability in injury rates and making conclusions regarding risk factors difficult. Nevertheless, modifiable potential risk factors may be relevant for future interventions.
Many studies examining sport injury in general have identified age, sex and BMI as significant risk factors for injury in youth, but there are conflicting results in the literature as to whether these specific factors affect injury risk in rock climbers in this, or any other age group.2 , 3 , 16 , 25–27 Results regarding sex as a risk factor for injury in climbing are conflicting. The majority of the studies examined samples that were predominantly male, and Wright et al,8 who found a significantly higher risk of injury in males, failed to report sex distribution. The studies that reported no difference between sexes included samples ranging from 59.9–83.3% male.2–5 , 18 It is therefore difficult to know the validity of these conclusions, as overall methodological quality was low.
Results suggest that older age may be a risk factor for injury in sport climbing and bouldering, though conclusions are difficult to draw, as reviewed studies used convenience samples with heterogeneous age groups. Authors have also suggested that there are differences in the types of injury sustained by younger and older climbers, such as epiphysial fractures of the fingers from repeated stress on the bone in children and adolescents.28 Based on this research, the International Climbing and Mountaineering Federation (UIAA) has set the minimum age for international bouldering competition participation at 16 years. This guideline was established to minimise the risk of epiphysial fractures, as bouldering training often involves dynamic movements that should be avoided in children whose bones have not yet matured sufficiently.28 It would follow that if the types of injury differ between adults and children, the risk of injury may differ as well. Similar conclusions have been made previously with regard to resistance training in young children and adolescents, though past claims that such training is unsafe and poses a risk of injury are now being refuted. Current research indicates that age-appropriate resistance training can be safe.29 Future studies are needed to explore this possibility in young climbers. An additional consideration when examining age as a risk factor is that multicollinearity may exist with factors such as years of experience and difficulty level. Analyses involving these individual factors must therefore be adjusted for age.
The literature suggests that increasing years of climbing experience may increase the risk of injury. More research is needed to confirm these findings and to explore whether this factor is associated with other variables (eg, age, height, weight, skill level). The same is true for the highest difficulty or skill level at which individuals climb. A multitude of different rating scales were used to grade the technical difficulty of climbs, as different countries and different disciplines often use different scales. However, the UIAA Medical Commission recently established a metric rating system into which all countries’ scales can be converted, standardising reporting for research purposes in particular.30 , 31 With this scale it will become easier to compare studies and make conclusions about skill level as a risk factor.31
Though there is a paucity of valid research about BMI as a risk factor for injury in climbing, the results reported by Backe et al, that higher BMI was significantly associated with a higher risk of injury and reinjury, appear to be valid, as this study was of higher methodological quality. As well, their study sample approached a normal population distribution for BMI, making their results more generalisable.16 Previous research involving other sports has also indicated that BMI is a potentially modifiable risk factor.26 As such, it may gain attention for injury prevention strategies in climbing. Similarly, body weight merits further investigation, though care must be taken when analysing BMI and body weight together, considering multicollinearity between these two measures.
When compared to top roping (and in two cases bouldering), the examination of lead climbing suggests that it is a potential risk factor for injury. As a modifiable risk factor, limiting the amount of ‘leading’ that a climber does may reduce injury.
Results are conflicting with regard to climbing volume as a predictor for injury in climbing. Backe et al 16 and Schlegel et al 13 did not find that higher climbing volumes increased the risk of injury. Two studies, however, combined climbing volume with climbing grade to calculate CIS, both showing a significant correlation between higher CIS and injury. Neither study sample, however, was representative of their population, and neither adequately adjusted for confounding.9 , 19 While more research examining climbing volume and intensity is required, CIS may be a measure to use in future studies. Climbing volume and CIS are both potentially modifiable risk factors, and knowing the healthy limit may aid in injury prevention.
Research involving general youth populations has shown that behaviours such as alcohol consumption and smoking tobacco are risk factors for sport injury.32 Although findings by Gerdes et al 14 and Hasler et al 18 are conflicting, it follows that these behaviours would increase the risk of injury in youth climbers. These behaviours are modifiable and therefore merit further investigation.
Finally, muscular strength has been suggested as a possible factor influencing musculoskeletal injury.33 Results from the two studies examining this factor are difficult to ascertain conclusions from, but as low grip strength may be another modifiable risk factor, research is warranted in this area.
Few studies have investigated prevention strategies for climbing. Stretching is often used for injury prevention, though Josephsen et al 2 found no association, and Tomczak et al 10 suggested a positive relationship between climbing injury and the use of stretching. However, a high proportion of the participants in Tomczak et al's study reported stretching prior to climbing (73%), and the association found by the authors does not necessarily imply causation. This is likely a spurious correlation.10 Though there is presently no evidence that warming up affects injury risk in climbing and the use of stretching remains inconclusive, this may yet be an avenue for future research, as these are both easily modifiable factors that many climbers perform nonetheless.
Limitations
Several factors limit our ability to draw valid conclusions based on the data available for this systematic review, including the multidisciplinary nature of climbing, the multitude of injury definitions, injury rate reporting and methodologies and the heterogeneous nature of the study populations. The majority of studies were retrospective surveys and were therefore subject to the biases associated with cross-sectional studies. Recall bias and an overestimation of the most traumatic injuries may have resulted, as well as uncertainty of temporal relationships and causation. Selection bias is also a limitation of convenience samples, as injured climbers may not be included in the sample if they were not present during recruitment. Finally, publication bias may have influenced the results.
Conclusions and perspectives
Intrinsic and extrinsic risk factors for injury specific to sport climbing and bouldering have not previously been the subject of reviews. Twelve electronic databases and several other sources were searched systematically, to examine risk factors and prevention strategies for injury in these disciplines, and to assess the methodological quality of existing studies. The injury incidence proportions and rates are inconsistent throughout the literature, emphasising the need for standardised injury reporting in climbing research. The overall methodological quality of reviewed studies was low according to the Downs and Black Quality Index. However, several potential risk factors for injury in sport climbing and bouldering were highlighted, including age, increasing years of climbing experience, higher skill (difficulty) level, a high CIS and lead climbing. Several potential risk factors are worth further investigation, namely those that are modifiable, such as BMI, taping, weight training and the use of stretching. Results regarding injury prevention measures remain inconclusive. Future avenues for research in climbing should include previous injury, as it has been shown to be a significant predictor for subsequent injury in other sports,6 as well as examining the use of correct climbing technique and the growing issue of ‘climber's back’.34 As climbing continues to gain popularity, understanding the healthcare burden presented by this sport is essential. Developing injury prevention measures will reduce the strain on healthcare resources, and disseminating knowledge about the main types, mechanisms and risk factors for injury will be important to reduce these injuries through awareness, for climbers as well as for healthcare providers. It will be important for future research to involve youth, such that young climbers, their parents and coaches, will be able to learn safe development and training for climbing.
Acknowledgments
The Sport Injury Prevention Research Centre is one of 9 International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table
Footnotes
-
Twitter Follow Carly McKay at @Dr_CMcKay
-
Contributors KYW contributed to the planning, conduct of analysis and reporting of the results. KYW is responsible for the overall content of this research. CDM contributed to the planning, conduct of analysis and reporting of the results. CAE contributed to the planning, conduct of analysis and reporting of the results.
-
Funding The authors acknowledge the funding provided by Alberta Innovates Health Solutions and the Alberta Children's Hospital Research Institute for Child & Maternal Health through the Talisman Energy Research Fund in Healthy Living and Optimizing Health Outcomes. Dr Emery is supported by a Population Health Investigator Award from Alberta Innovates Health Solutions and a Professorship in Pediatric Rehabilitation in the Faculty of Medicine, University of Calgary (Alberta Children's Hospital Foundation).
-
Competing interests None declared.
-
Provenance and peer review Not commissioned; externally peer reviewed.