Article Text

Abstract
Objective The purpose of this study was to examine the association of knee injuries with subsequent changes in body mass index and body composition during maturation in young females.
Methods A prospective longitudinal study design was employed to evaluate young females active in soccer or basketball (N=862). Participants who completed at least 1-year follow-up to provide consecutive annual measures of BMIZ and %fat were included in the study analysis to determine the effect of knee injuries on the trajectory of these obesity markers in youth.
Results Of the 71 reported knee injuries, 12 (17%) occurred in athletes at the prepubertal stage, 24 (34%) in athletes at the pubertal stage, and 35 (49%) in postpubertal athletes. Controlling for the effects of maturation, female athletes who reported knee injury demonstrated a greater yearly increase in BMIZ (LS means and 95% CI for the injured group=0.039 (−0.012 to 0.089), for the non-injured group=−0.019 (−0.066 to 0.029), and group difference=0.057 (0.005 to 0.11), p=0.03) and in %body fat (LS means and 95% CI for the injured group=1.05 (0.45 to 1.65), for the non-injured group=0.22 (−0.21 to 0.064), and group difference=0.83 (0.21 to 1.45), p=0.009), compared to those without knee injuries. This indicates that the athletes with knee injuries will increase their body mass index percentile by up to 5 units more than someone of the same age without an injury, and in body fat by up to 1.5%, compared to their non-injured peers.
Conclusions The present findings indicate that knee injury during the growing years may be associated with unfavourable changes in body composition.
- Sporting injuries
- Women in sport
- Injury Prevention
- Food intake/body weight regulation
Statistics from Altmetric.com
Introduction
Compared to inactive youth, children and adolescents who are physically active demonstrate increased levels of musculoskeletal strength, enhanced cardiorespiratory function and improved metabolic health.1–5 In young girls, sports team participation was associated with increased physical activity and reduced television viewing and body mass index (BMI) in a dose–response fashion.6 In this same pattern, fifth grade children who participated in recreational sport programmes throughout the year demonstrated increased fitness performance over their peers who did not participate in any sport or only participated in one sport.7 In fourth and fifth grade children, the addition of an after-school soccer programme effectively decreased BMI z-scores at 3 and 6 months and influenced increases in daily, moderate and vigorous physical activity at 3 months.8 Increased participation in activities designed to improve physical fitness during childhood and adolescence may provide an optimal mechanism for promoting physical activity as an ongoing lifestyle choice and ultimately support lifelong cardiometabolic health.9 ,10
While sport participation provides a mechanism to increase physical activity levels in youth, recent reports indicate that sports participation or physical activity without adequate preparatory conditioning may increase risk of injury in maturing children.11 A drastic and sudden deficit in physical activity from chronic pain or acute injury can initiate a ‘negative spiral of disengagement,’ whereby reduced physical activity leads to diminished cardiorespiratory fitness, increased adiposity and poor health outcomes.12 In addition, youth who cease sport participation during adolescence may be at a higher risk of metabolic syndrome and inactive lifestyles as an adult.13 ,14 Ultimately, sports and recreation injury during youth may initiate detrimental health effects making them less active during adolescence which may manifest into sedentary lifestyle habits and high risk of cardiometabolic disorders during adulthood.15–19
These findings raise a fundamental question: Are young athletes who suffer a physical activity-related injury early in life at increased risk for long-term reductions in physical activity and consequent unhealthy weight gain? Perhaps the physical and psychosocial consequences of a musculoskeletal injury in a previously active youth may limit or bar future participation in sports or physical activities at the desired frequency and intensity. At present, data regarding the longitudinal effects of sport-related injuries on overweight and obesity markers in active maturing females are limited. Therefore, the purpose of this investigation was to examine the association between knee injuries and changes in body composition during maturation in young athletic females. The hypothesis was that active maturing females who sustain a knee injury would be at increased risk for greater subsequent increase in overweight and obesity markers as evidenced through BMIZ and fat percentage measurements.
Patients and methods
Subjects
Female basketball and soccer players were recruited from a single geographic region, Boone County school district. Five middle schools and three high schools, teamed with two nearby universities, participated in a prospective longitudinal study. The recruited schools provided 6 high school and 15 middle school basketball teams along with 2 collegiate, 7 high school and 3 middle school soccer teams. From the initial sample (n=862), 352 female athletes who did not report knee injuries at the first visit and completed at least 1 more year of follow-up were included in the current analyses (figure 1). Female athletes who chose not to participate or did not make their respective sport's teams or who graduated during the follow-up years from study onset were not included in the study.
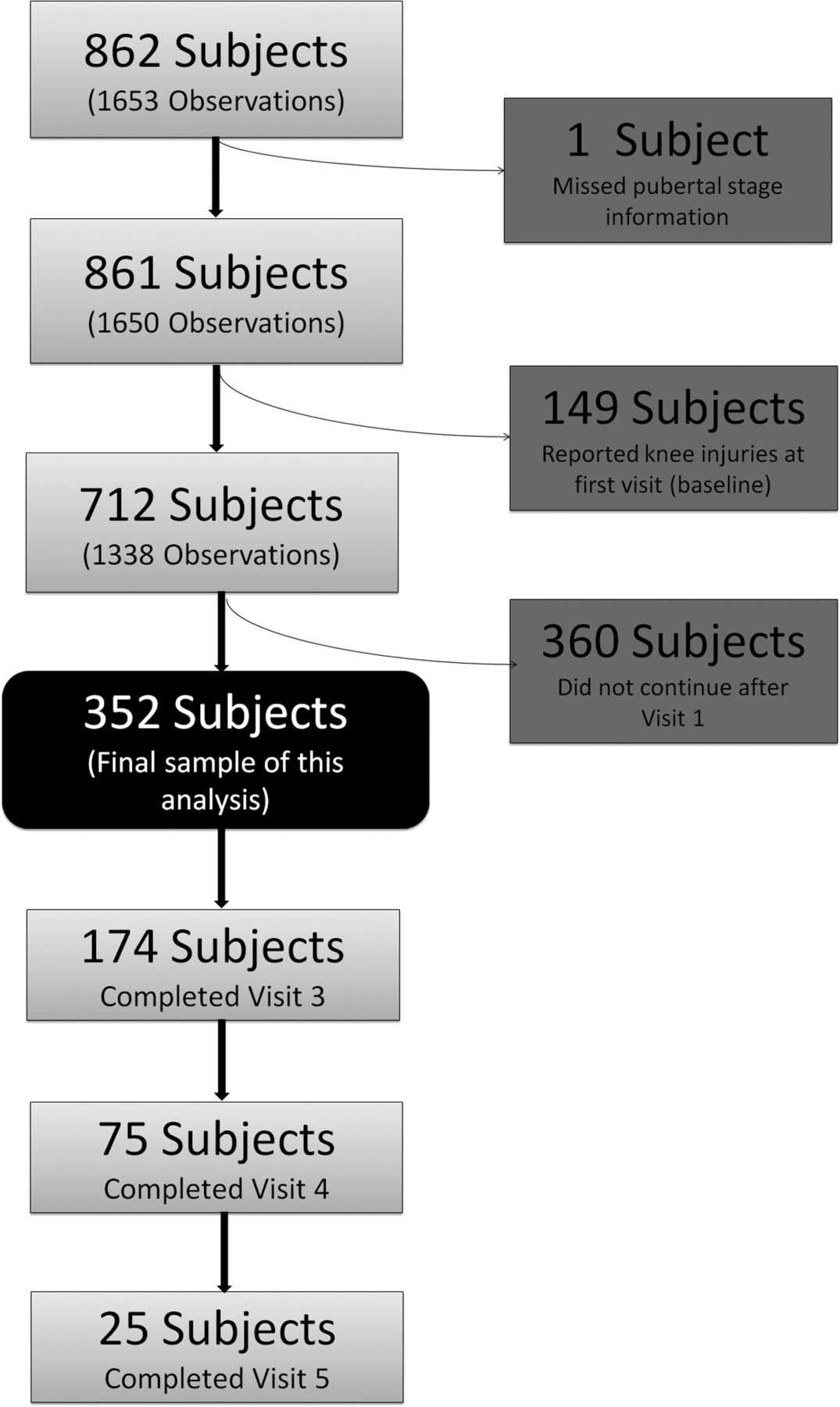
Flow chart which provides a graphical depiction of the study population as a whole, and how the final sample of 352 participants was identified for the study analysis. Note that the number of participants and the number of observations did not decrease the same amount as each participant could have had 1, 2 or 3 visits in the sample.
Procedures
The Cincinnati Children's Hospital Medical Center Institutional Review Board approved the data collection procedures and consent forms. Parental consent and child assent were received in participants under the age of 18 years and consent was obtained from those 18 years or older prior to data collection. Participants were tested prior to the start of their competitive soccer or basketball season. The testing session included a knee examination, medical history form and interview, maturational estimates and anthropometrics.
Demographics and medical history
Prior to the initial testing session, all participants completed a two-page questionnaire that addressed issues of prior and concurrent sport participation, self-reported maturational characteristics and a personal and family history of sport-related injuries. Knee injury was defined as any pain or injury to the structures surrounding the knee, resulting in time loss from sport participation. On a subsequent annual follow-up (approximately 12 months later), the questionnaire and medical history interview were repeated.
Anthropometrics and maturational assessment
Height was measured with a stadiometer with the participant in bare feet. Body mass and body composition (relative fat percentage via bioelectrical impedance) were assessed according to the manufacturer's standards (age-specific and sex-specific equations) on a TBF-300A Body Composition Analyzer (Tanita Corporation of America, Inc, Arlington Heights, Illinois, USA). BMIZ was calculated using a SAS macro (gc-calculate-BIV.sas, available on the CDC website), which allowed combination over age. Electrical impedance measures have demonstrated excellent reliability and validity relative to dual-energy x-ray absorptiometry for adults and hydrostatic weighing for children.20 The modified Pubertal Maturational Observational Scale (PMOS) was used to classify the participants into one of three pubertal categories (prepubertal, pubertal and postpubertal). PMOS is a reliable instrument that21 uses both parental questionnaires and observations, all performed by a single investigator, to classify participants into one of three pubertal categories: prepubertal, pubertal and postpubertal.22–25
Statistical analyses
Participants who indicated a positive response to the development of a knee injury on the medical history form or interview at a follow-up visit were allocated to the injury group, while those who did not report a new knee injury served as the uninjured referent group. Univariate analyses were conducted to examine data distribution and describe the characteristics of the study sample. We examined descriptive statistics, including range, mean, SD, frequencies and percentages, for the whole study sample and also by pubertal stage. We calculated the knee injury incident rate by the athlete’s pubertal stage for each year and the further accumulative incident rate by the pubertal stage for the entire follow-up time. We examined the association of anthropometric outcomes (yearly change of BMI z-score, and yearly change of body fat percentage) with knee injury status using generalised mixed models to account for the repeated measures over time, assuming an underlying autoregressive correlation structure. This latter approach was used for bivariate and multiple-variate modelling when examining for potential covariates and confounders. Those considered were pubertal status and sport. SAS V.9.3 (SAS Institute, Inc, Cary, North Carolina, USA) was used for all data analysis.
Results
At the first visit, the study participants were 13 years (SD=1.7), 157.8 cm (SD=8.6 cm), and had a mean body mass of 51.5 kg (SD=11.5 kg). Table 1 presents the anthropometric and demographic and sport characteristics of the female participants by maturational stage. Pubertal girls are taller, heavier and have a higher per cent of body fat than prepubertal girls, despite their being only about half a year older. Participants completed two to five visits, with 174 (49.4%) completing at least three visits (including first visit). The mean length of follow-up was 23 (±11.9) months. A knee injury was reported in 71 participants. Of these 71 knee injuries, 12(17%) occurred in athletes at the prepubertal stage, 24 (34%) in athletes at the pubertal stage, and 35 (49%) in the postpubertal athletes, where pubertal stage was defined as the visit immediately prior to the knee injury. These injuries occurred after 12.2 (±9), 15.7 (±7) and 22.2 (±11) months of follow-up in the prepubertal, pubertal and postpubertal groups, respectively. Of the 71 young girls who reported knee injuries, 40 did not return for the second follow-up. Of the 31 who returned, 20 continued with one visit, 11 continued with two visits, and none continued with three visits or beyond.
Study population—baseline information from study participants included in the final analyses
Bivariate analyses showed a significantly greater yearly increase in BMIZ (LS means and 95% CI for the injured group=0.04 2 (0.002 to 0.080), for the non-injured group=−0.014 (−0.051 to 0.024), and group difference=0.055 (0.001 to 0.11), p=0.047). Also noted was a yearly increase in body fat percentage (LS means and 95% CI for the injured group=1.37 (0.83 to 1.91), for the non-injured group=0.56 (0.21 to 0.90) and group difference=0.82 (0.17 to 1.46), p=0.01) among female athletes who reported knee injuries, compared to those who did not. When controlling for the effects of pubertal maturation, the differences in BMIZ trajectory and body fat percentage trajectory (between the injured group and the non-injured group) stayed significant. Specifically, for yearly changes in BMIZ, LS means and 95% CI for the injured group=0.039 (−0.012 to 0.089), for the non-injured group=−0.019 (−0.066 to 0.029) and group difference=0.057 (0.005 to 0.11), p=0.03; and for yearly change in body fat percentage, LS means and 95% CI for the injured group=1.05 (0.45 to 1.65), for the non-injured group=0.22 (−0.21 to 0.064) and group difference=0.83 (0.21 to 1.45), p=0.009.
Figure 2A,B present the yearly change of BMIZ (from the last visit) over time, or the BMIZ trajectory, for the reference group and investigational group, respectively. An examination of the graphs reveals a greater yearly increase of BMIZ at the visit when the new knee injury was reported among the female athletes who were injured, while the trajectory of BMIZ remained stable among those who were not injured. When further limited to the participants who provided at least three longitudinal measures prior to the new knee injury (n=26; figure 3), a more pronounced increase of BMIZ change associated with the new knee injury was observed.

(A) Plot represents change (from the previous year) in BMIZ for female athletes who did not sustain a knee injury (n=281). (B) Plot represents change (from the previous year) in BMIZ for female athletes who reported a new knee injury (n=71). Blue-shaded area indicates the year of the reported knee injury. The visit year indicates±years from the year of the reported knee injury.

{kind=link}
{kind=link}
{kind=link}
Plot represent change (from the previous year) in BMIZ of participants in subgroup analysis (n=26). Blue-shaded area indicates the year of the reported injury. The visit year indicates±years from the year of the reported knee injury.
Discussion
The salient finding from the current dataset of healthy young female participants is that those who reported a knee injury demonstrated significantly greater increases in BMIZ (increased BMI percentile by up to five units more) and an increase in body fat percentage (by up to 1.5%) relative to their uninjured peers within 1 year of the reported injury. Of interest, the entire sample (injured and uninjured) of pubertal and postpubertal participants demonstrated BMIZ of +0.6 and +0.6, respectively, at their first visit. A z-score above zero would be indicative of BMI greater than for age-matched and sex-matched peers from the general populations of youth prior to the year 2000.26 To have a sample of athletic participants showing global increases in BMI measures, compared with the age- and sex-matched youth of the past, is a public health concern. While participation in sport-related activities has dramatically increased over the past three decades, during the same time frame, paediatric obesity rates in the USA have more than doubled with over one-third of all US adolescents falling into the overweight or obese categories.27–29 Over the next two decades, researchers forecast a 33% increase in obesity and a 130% increase in severe obesity in non-pregnant adults ≥18 years.30
As the results of the current study show, there appears to be an acceleration in BMIZ trajectory during the year of the reported knee injury. However, no similar acceleration occurs in BMIZ measures in the current population until the year of the reported knee injury. Normal growth and development influence a small increase in the adiposity and overweight markers, but the current data indicate that a reported knee injury will influence a more rapid decline in health-related measures in young girls.
Knee injury and overweight/obesity in isolation are two of the primary contributors to long-term osteoarthritis,31 ,32 and the detrimental effects of increased BMI and knee injury during the growing years very likely compound the risk for osteoarthritis during adulthood. The relative ineffectiveness of treatment and the poor long-term prognosis for both knee injuries in young athletes and obesity during childhood indicate that methods fostering prevention are needed to reduce the associated morbidity.33–37
With an increasing number of youth sport participants and an association between sports-related injuries and markers of overweight and obesity in youth, there is compelling impetus to better prepare aspiring young athletes for the demands of sports practice and competition. Specifically, knee injuries which occur 2–10 times more often in females relative to males can often restrict young girls from participation in PA.38 Reduced levels of regular PA during the growing years can lead to diminished levels of physical fitness, increased adiposity and poor health outcomes.12 ,39–42 Previously, little if any attention has focused on prevention strategies for knee injury in preadolescent and early adolescent females.43 ,44
Although the total elimination of recreational and physical activity-related knee injuries in young athletes is an unrealistic goal, regular participation in appropriately designed and sensibly progressed preparatory conditioning programmes beginning during preadolescence may help to reduce the likelihood of a sports-related knee injury in young athletes and the resultant unhealthy weight gain. Although only a minority of aspiring young athletes participate in conditioning programmes prior to sports participation,45 recent data indicate that multifaceted conditioning programmes may reduce sports-related injuries in adolescents44 and have an even greater potential to reduce injury and improve health if implemented during preadolescence.18
Limitations
Increases in overweight and obesity markers during youth very likely have a multifactorial aetiology. Prior epidemiological data indicate that both intrinsic (eg, genetics and maturation) and extrinsic (environmental factors such as diet, hormonal and potentially psychological parameters) factors may contribute to increases in body fat per cent and BMIZ in young girls. Future investigations with larger sample sizes should aim to develop more robust risk factor prediction models, which include other potential contributing parameters (eg, genetics, hormonal measures and potentially psychological parameters) to further elucidate risk factors for the evaluated changes in body composition. Another potential limitation to consider is that the current analyses were limited to the study participants who returned to sport following their knee injury as this was the inclusion for their involvement in this longitudinal investigation. It is likely that the demonstrated effects of increasing body fat per cent and BMIZ would be even more pronounced in those study participants who injured their knee and discontinued sports participation and therefore experienced even greater reductions in PA. As noted in the results, of the 71 who reported the first knee injury, nearly 60% discontinued participation in the following year, which further suggests the detrimental effect of knee injury on physical activity in youth. Continued efforts to monitor all injured sports participants who experience knee injuries, especially those who discontinue sport participation, may further elucidate the rapid detrimental effects of reduced PA on unhealthy weight gain during adolescence. As noted earlier, previous investigations have found relationships between the obesity markers investigated in the current study and risk factors to knee injury. While the current investigation utilised robust longitudinal analyses, future work to clarify causation between the reported relationships of knee injury and increased markers of obesity is warranted. Lastly, we were unable to include the timing of the injury during each follow-up year in the model. The interval between time of the injury to a follow-up interview likely affects weight gain measured. For example, the weight gain in a girl who was injured just 1 month before the follow-up interview would be different, had she been injured 11 months before the interview. Future research is warranted to monitor both the acute and long-term effects of knee injury on reductions in PA and cardiometabolic health in youth.
Summary and conclusions
While regular sport participation has the potential for enhancing the health, well-being and fitness of school-age youth, the current results indicate that knee injury can initiate an unhealthy gain in body mass and detrimental changes in body composition in young female athletes. Youth who are not adequately prepared for the demands of sports practice and competition may be at increased risk of knee injury and consequent increased adiposity. Since physical inactivity is now recognised as the fourth leading risk factor for global mortality,46 long-term initiatives that aim to maintain participation in PA throughout the lifespan, while reducing the prevalence of obesity and related disorders, are warranted.
What are the new findings?
-
Young females, active in sport, who reported knee injury demonstrated a significantly greater increase in the relative body fat percentage trajectory compared to their non-injured peers.
-
The present findings indicate that a knee injury during the growing years may be associated with unfavourable changes in body composition for females who participate in sport.
How might it impact on clinical practice in the near future?
-
The current results indicate the importance of prevention of physical activity-related injuries with appropriately designed youth prevention programmes, which can help children maintain the benefits of sport participation while avoiding the negative effects of injury on the relative body composition.
-
Further work is needed to develop strategies that influence safe sport and vigorous physical activity participation that can support the associated increased energy expenditure and fitness levels compared with non-sports participants.
Acknowledgments
The authors would like to thank Boone County Kentucky, School District, especially School Superintendent Randy Poe, for participation in this study. We would also like to thank Mike Blevins, Ed Massey, Dr Brian Blavatt and the athletes of Boone County public school district for their participation in this study. All authors are independent of any commercial funder, had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
References
Footnotes
-
Contributors GDM contributed to the conception and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, obtaining funding and supervision. ADF contributed to the conception and design, critical revision of the manuscript for important intellectual content, analysis and interpretation of data, and administrative, technical or material support. KBF contributed to the acquisition of data, drafting of the manuscript, and administrative, technical or material support. YX contributed to the analysis and interpretation of data, critical revision of the manuscript for important intellectual content, and statistical analysis. J K contributed to the analysis and interpretation of data, critical revision of the manuscript for important intellectual content and statistical analysis. LMD contributed to the analysis and interpretation of data, critical revision of the manuscript for important intellectual content, and administrative, technical or material support. TMC contributed to the interpretation of data, critical revision of the manuscript for important intellectual content, and administrative, technical or material support. TEH contributed to the conception and design, critical revision of the manuscript for important intellectual content, obtaining funding and supervision.
-
Funding This work was supported by the National Institutes of Health/NIAMS Grants #R01-AR049735, #R01-AR05563 and #R01-AR056259.
-
Competing interests None.
-
Ethics approval Cincinnati Children’s Hospital IRB Board.
-
Provenance and peer review Not commissioned; internally peer reviewed.