Article Text

Abstract
Objective To assess whether three-dimensional imaging of the Achilles tendon by ultrasonographic tissue characterisation (UTC) can differentiate between symptomatic and asymptomatic tendons.
Design Case-control study.
Setting Sports Medical Department of the Hague Medical Centre.
Patients Twenty-six tendons from patients with chronic midportion Achilles tendinopathy were included. The “matched” control group consisted of 26 asymptomatic tendons.
Interventions Symptomatic and asymptomatic tendons were scanned using the UTC procedure. One researcher performed the ultrasonographic data collection. These blinded data were randomised, and outcome measures were determined by two independent observers.
Main outcome measurements The raw ultrasonographic images were analysed with a customdesigned algorithm that quantifies the three-dimensional stability of echo patterns, qua intensity and distribution over contiguous transverse images. This threedimensional stability was related to tendon structure in previous studies. UTC categorises four different echotypes that represent (I) highly stable; (II) medium stable; (III) highly variable and (IV) constantly low intensity and variable distribution. The percentages of echo-types were calculated, and the maximum tendon thickness was measured. Finally, the inter-observer reliability of UTC was determined.
Results Symptomatic tendons showed less pixels in echo-types I and II than asymptomatic tendons (51.5% vs 76.6%, p<0.001), thus less three-dimensional stability of the echo pattern. The mean maximum tendon thickness was 9.2 mm in the symptomatic group and 6.8 mm in the asymptomatic group (p<0.001). The Intraclass Correlation Coefficient (ICC) for the interobserver reliability of determining the echo-types I+II was 0.95. The ICC for tendon thickness was 0.84.
Conclusion UTC can quantitatively evaluate tendon structure and thereby discriminate symptomatic and asymptomatic tendons. As such, UTC might be useful to monitor treatment protocols.
Statistics from Altmetric.com
Introduction
The Achilles tendon is a hierarchically arranged structure with a collagenous matrix in the direction of tensile forces transferred through the tendon.1
Midportion Achilles tendinopathy is the clinical designation used for a painful swollen Achilles tendon at 2–7 cm proximal to the tendon insertion with an impaired function.2 3 In these tendons, a remarkable matrix disintegration can be found as a consequence of degeneration. Biochemically, a young matrix with high collagen turnover and a tendency to fibrotic repair is observed.4 These phenomena are elements of the histopathological label “tendinosis”.5
On ultrasonography, the echogenicity of tendons is based on the density and arrangement of the collagenous matrix. Normal tendons are characterised by a regular echo pattern, qua intensity and arrangement in grey scale images.6 7 On the contrary, disintegration of tendon bundles leads to a remarkable loss of the echogenicity. Consequently, hypoechoic lesions are frequently described in cases of tendinosis.8
There are some sonographic studies that evaluated the possible difference between symptomatic and asymptomatic tendons. One study reported only hypoechoic areas in 68% of the symptomatic Achilles tendons,9 but another group found hypoechoic areas also in 11% of asymptomatic tendons.10 Some studies focused on the prognostic value of hypoechoic lesions. No difference was found in overall outcome after conservative treatment between tendons with normal ultrasonographic appearance and tendons with a hypoechoic area.11 Khan et al12 reported that a reduced area of hypoechogenicity on ultrasonography did not correlate with an improved clinical outcome.
The main problem with ultrasonography is that it is a real-time and operator-dependent technique; transducer handling and machine settings can influence size and appearance of a hypoechoic lesion. To our knowledge, the inter-observer reliability of ultrasonographic assessment of tendon structure is not known, and changes in time are difficult to compare. Furthermore, the structure of the (disintegrated) tendon is a three-dimensional phenomenon that cannot be captured in flat two-dimensional transverse (nor longitudinal) images.
There is growing interest in finding ways to quantify tendon integrity.13 14 In veterinary medicine, a method for computerised ultrasonographic tissue characterisation (UTC) has been developed for tendons in the horse.15 This work revealed that each ultrasonographic image actually is a mixture of “structure-related echoes” and “interference”.7 16 Structure-related echoes are directly generated at tendon bundles and are stable over a large number of contiguous transverse cross sections. Echoes resulted from interference are the result of multiple echoes generated by smaller entities, like fibrils, cells or fluid and are variable over contiguous cross sections. Based on these equine studies, four different echo-types were discriminated with use of this three-dimensional stability criterion. With histology as reference test, the echo-types reflected the underlying structure and pathology in the horse tendon tissue (fig. 1).15,–,19
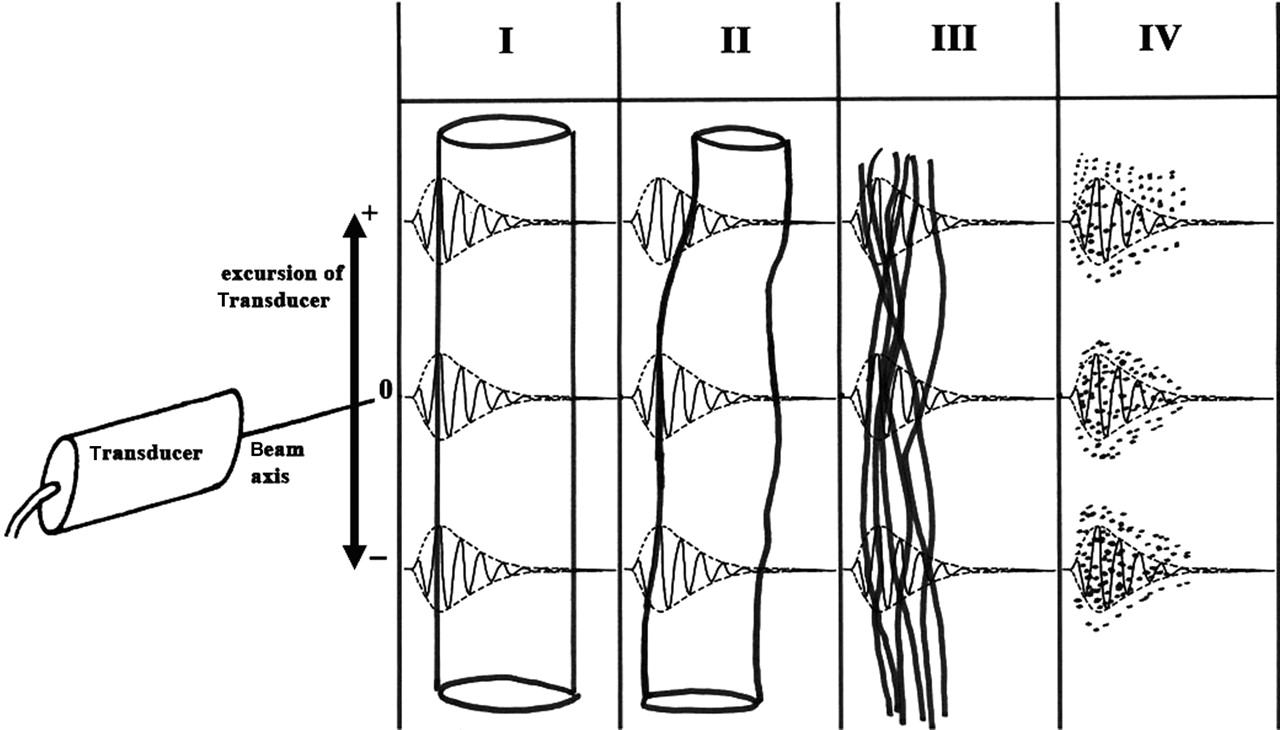
Ultrasonographic tissue characterisation (UTC) is based on a transducer in transverse position that is displaced stepwise in the longitudinal direction. In this way, contiguous transverse images provide longitudinal information. The transducer emits ultrasound waves into the tissue in the direction of the beam central axis. According to Harris et al,18 these waves form a three-dimensional sample volume that moves through tissue. Every echo in the ultrasonographic image is the resultant of interactions/reflections that occur in this sample volume. Depending of size of anatomical structure relative to the three-dimensional sample volume, echoes can be divided into “structure-related” and “interfering”. Structure-related echoes (types I and II) are generated by only one large structure present in the sample volume, thus one interface and one hit of ultrasound wave resulting in one really structure-related echo that is stable over a large number of contiguous transverse images while the transducer moves along the tendon. In contrast, interfering echoes (types III and IV) represent more than just one smaller structure in the same sample volume, thus multiple interfaces and multiple hits, and thus one echo is the resultant of multiple interfering ones. These echoes are characterised by a remarkable lack of stability over contiguous transverse images. UTC algorithms were tested on isolated flexor tendons collected from horses. By precise matching of UTC processed images with exactly corresponding tendon sections, echo-types were verified with use of histology as reference test: (I) intact and aligned tendon bundles; (II) less integer and waving tendon bundles; (III) mainly fibrillar tissue and (IV) a mainly amorphous matrix with loose fibrils, cells or fluid.7 15,–,17 19
The aim of this study is to evaluate UTC in the human setting. Therefore, we determined its inter-observer reliability and verified whether the technique could discriminate symptomatic and asymptomatic tendons. The tendon thickness was also determined.
Materials and methods
Patients
Patients were included in an outpatient sports medicine department in a large district general hospital. Patients who had participated in a previous study on the effect of an eccentric exercise program at the sports medicine department were included.20 21 In this previous study, inclusion criteria were an age between 18 and 70 years and presence of symptoms for more than 2 months. All patients had a tendon, which was tender on palpation and painful during or after activity. The tendon thickening was located approximately 2–7 cm proximal to the distal insertion. The diagnosis was made based upon clinical examination. Exclusion criteria were the presence of an insertional disorder and complete tendon rupture. Most of the patients had already received several types of conservative treatment, but none had undergone surgery for their Achilles tendon injury.
All patients with persistent pain on palpation or during sports and <100 points on the Victorian Institute of Sport Assessment-Achilles ( VISA-A) questionnaire,22 which is a validated instrument to quantify the clinical severity of Achilles tendinopathy, were selected in the symptomatic group. The activity of the lower extremity was evaluated with use of the Ankle Activity Score (AAS),23 which quantifies the anklerelated activity level.
Ultrasonographic images of “matched” asymptomatic tendons were collected from patients who visited the sports medicine department for other injuries. When individuals had not experienced pain in one of their Achilles tendons in the past, they were asked to participate in the study for evaluation of both their Achilles tendons. Inclusion was based on matching the symptomatic group in age, gender and activity level.
Ultrasonographic tissue characterisation
The UTC procedure and measurements were performed using a standardised protocol (fig. 2). A 10-MHz linear-array transducer (Smartprobe 10L5; Terason 2000, Teratech, USA) was moved manually along and perpendicular to the tendon's long axis over a distance of 9.6 cm. A custom-built tracking and data-collection device facilitated the collection of “raw” digital transverse images at regular distances of 0.2 mm. These images were stored on the hard disk of a computer and subsequently composed to a three-dimensional data block. This data block was used for the tomographical visualisation of the Achilles tendon in three planes of view: transverse, sagittal and coronal (fig. 3).

Standardised ultrasonographic tissue characterisation procedure. The patients lay prone on the examination table with their feet hanging over the edge of the examination table. The Achilles tendons were manually positioned in a maximum angle of dorsiflexion to ensure that the ultrasound probe was constantly perpendicular to the tendon. A stand-off with scan gel was applied to the Achilles tendon. The transducer was moved manually from proximal to distal in a straight line along a frame over a distance of maximum 9.6 cm with collection of images every 0.2 mm. These images were stored on the hard disc of a computer and subsequently composed to a threedimensional data block.

Tomographic visualisation of a right Achilles tendon in three planes of view, in raw greyscale. (A) Transversal view. (B) Sagittal view. (C) Coronal view. (D) Transversal view with the maximum antero-posterior thickness measured (white arrow), being the largest diameter perpendicular to the latero-medial width of the tendon. At this position the outline of the Achilles tendon was drawn in the transverse image. This cross-section was used for calculation of the percentages of echo-types within the tendon. S, skin; P, peritendinous space; AT, Achilles tendon; CA, calcaneal bone.
The three-dimensional stability of the echo pattern, qua intensity and distribution over contiguous transverse images was analysed and quantified by means of custom-designed algorithms for image analysis as developed on isolated tendons collected from horses.7 15,–,17 In these equine studies, four echo-types were assigned, based on the stability of intensity and distribution in contiguous transverse images, namely (I) highly stable; (II) medium stable; (III) highly variable and (IV) constantly low intensity and variable distribution. Figure 1 summarises how underlying tissue structure was related to the stability of the echo pattern. In the current human study, we used the same UTC algorithms.
All datasets were blinded and randomised. Two researchers (HVS, RJV) performed the complete UTC processing and analysis.
The thickest part of the tendon in the anterior–posterior (AP) direction was identified, and the maximum thickness was measured. After that, the border of the tendon was identified in the grey-scale image, and the percentages of the four echo-types at the transverse cross-section at this site were calculated (figs 3 and 4). Also, at 2 mm proximal and 2 mm distal from this position, the echo-types were calculated. The average of the echo-types in these three cross sections was used in the overall assessment of the tendon.
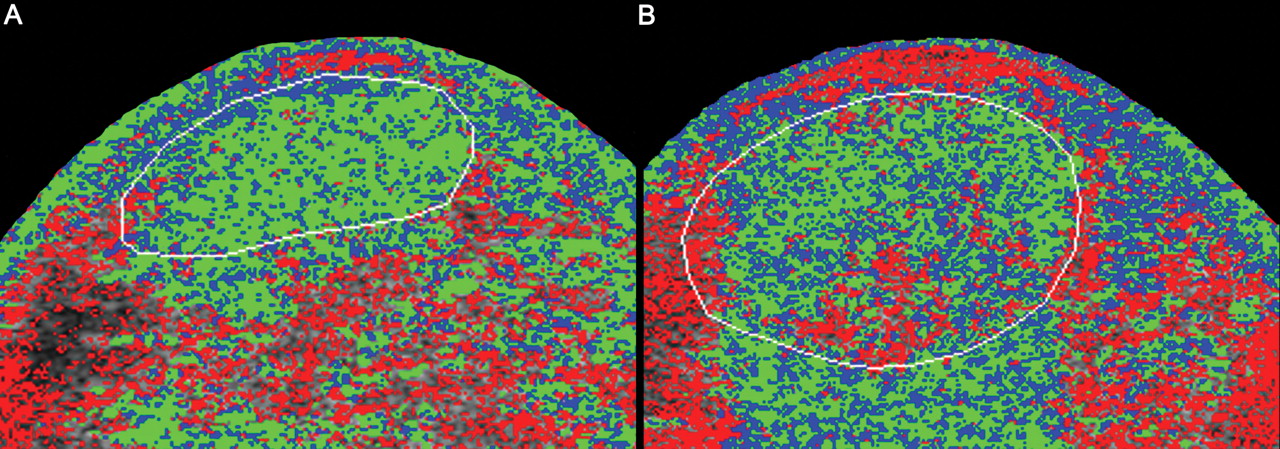
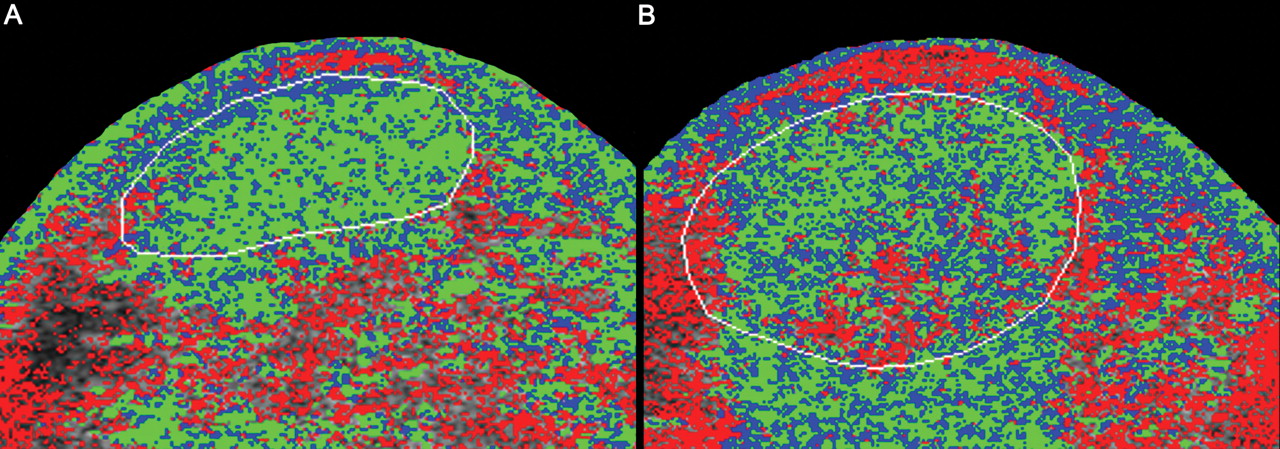
Difference of an ultrasonographic tissue characterisation-processed image between an (A) asymptomatic tendon and (B) asymptomatic tendon in transversal view. The border of the Achilles tendon, which was defined on the grey-scale image, is drawn with the white line. Green pixels represent echo-types I, blue pixels echo-types II, red pixels echo-types III and black pixels echo-types IV. Note the frequently observed increased echo-types III and IV on the posteromedial side within the asymptomatic tendon and the diffuse distribution within the symptomatic tendon.
Study design
The design was case-control study. The severity of the clinical status of the symptomatic tendons was evaluated by a single researcher, using the VISA-A questionnaire.22
The inter-observer reliability was calculated with a oneway random model. The intraclass correlation coefficient (ICC) was used to evaluate the correlation between the observations of two researchers. To evaluate the ICC, one score per observer per tendon was computed. The reliability is excellent if the ICC is >0.75, fair to good if 0.4<ICC>0.75 and poor if ICC is <0.4.15 To detect a difference in UTC parameters between symptomatic and asymptomatic tendons, a Student t test was used. Statistics were performed using SPSS version 15.0.0, and significance was assumed for p values <0.05. The study protocol was approved by the Medical Ethics Committee of the Hospital. Informed consent was obtained from all patients.
Results
Patients
In both the symptomatic and asymptomatic groups, 26 Achilles tendons were included.
In the symptomatic group, there were 12 male and 14 female tendons. In seven patients, symptoms were located in the left Achilles tendon, three patients in the right tendon and eight patients had bilateral complaints. The mean age was 44.9 years (SD 6.2), mean duration of symptoms was 193.9 weeks (SD 277.5) and the mean body mass index was 24.8 kg/m2 (SD 2.2). The mean AAS was 4.8 (SD 2.0), and the mean VISA-A score was 67.3 (SD 18.2).
In the asymptomatic group, there were 16 male and 10 female tendons. The mean age was 43.6 years (SD 12.6), and the mean body mass index was 26.1 kg/m2 (SD 4.3). The mean AAS was 5.5 (SD 1.6).
There was no significant difference between the symptomatic group and asymptomatic group in age (p=0.63), gender (p=0.17), BMI (p=0.20) and AAS (p=0.15).
UTC measurements
UTC analyses showed a distinct difference between the distribution of the four echo-types in the symptomatic group versus the asymptomatic group. Figure 4 represents a typical echo-type distribution of both groups in transversal view. Quantitatively, the symptomatic group was significantly different from the asymptomatic group for all echo-types (table 1). Although there was some overlap between the groups, symptomatic and asymptomatic tendons could be clearly discriminated, for example, based on the percentage of pixels in echo-types I+II (51.5% vs 76.6% in symptomatic vs asymptomatic, p<0.001; table 1, fig. 5). A difference in mean tendon thickness between symptomatic and asymptomatic tendons could also be observed (9.2 vs 6.8 mm in symptomatic vs asymptomatic, p<0.001; table 1).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The distribution of the percentages of echo-types I+II in symptomatic and asymptomatic tendons. A clear discrimination can be made between both groups. With a threshold of 75% echo-types I+II (dotted line), three tendons in the symptomatic group were above this threshold and six tendons in the asymptomatic group were below this threshold (dark bars). The other 43 tendons (grey bars) had a tendon structure that could be expected (abnormal structure in symptomatic tendons and normal structure in asymptomatic tendons).
Mean percentage of the separate four echo-types and tendon thickness are denoted for the symptomatic and asymptomatic tendons
When a threshold of 75% in echo-types I+II is chosen (see dotted line in fig. 5), three symptomatic tendons are above this threshold and six asymptomatic tendons are under this threshold (table 2). Thus, nine of the totally 52 tendons were categorised in another group than expected, based on the UTC findings. With 43 tendons that were categorised as expected, an accuracy of 83% was found.
The number of tendons that were symptomatic and asymptomatic are given
The ICC values for the UTC parameters are presented in table 1.
Discussion
This is the first study that quantifies tendon structure in patients with Achilles tendinopathy and controls with use of UTC. Symptomatic tendons showed significantly less stability of transverse echo patterns (less echo-types I+II) than asymptomatic tendons (p<0.001). The mean AP tendon thickness was 9.2 mm in the symptomatic group and 6.8 mm in the asymptomatic group (p<0.001). The inter-observer reliability of determining the UTC parameters was excellent (ICC 0.92−0.95) for quantification of the ultrasonographic tendon structure. This indicates that different observers examining the same tendon have excellent agreement between their findings; a prerequisite for implementation of UTC in the clinical setting. For the evaluation of the tendon AP thickness, an ICC of 0.84 was found.
Recently, other researchers focused on quantifying tendon integrity.13 14 For instance, Bashford et al13 attempted to quantify structural changes in tendon tissue by analysing the anisotropy of the speckle pattern of the ultrasonographic image. Anisotropy of tendons is based on their unique architecture with tendon bundles organised in longitudinal alignment. As such, this approach is fairly similar to UTC since both methods aim to isolate exclusively structure-related information from a “speckle pattern”. As a consequence of anisotropy, ultrasonography of tendons is sensitive for the tilt of the transducer, possibly leading to a hypoechoic representation of normal tendons.24 25 In case of UTC, this artefact is prevented by the tracking device with the transducer clamped in standardised position, in alignment and perpendicular to the tendons long-axis and with fixed transducer-tilt in the transverse plane. The foot was supported with the ankle joint in a maximum dorsiflexion which prevented a sag of the Achilles tendon as much as possible and thus resulted in an optimal angle of insonation. With this technique, only small tilting (lower than 3°) may have occurred. From previous equine studies, it is known that transducer tilting within 3° can result in small variations in grey level.26 However, with the use of UTC, the outcome in echo-types is determined with the relative grey value of the contiguous pixels and not the absolute grey value. Therefore, small tilting would have no effects on the echotypes measured with UTC.
In the study of Bashford et al,13 tendinopathic and healthy tendons could be discriminated with an accuracy of 80%. With optimal settings, an accuracy of 83% was found with use of UTC in this study, which is comparable with the study of Bashford et al13 (fig. 5 and table 2). The advantage of UTC is that a connection with underlying tissue histology was made with this approach in equine tendons.
The normal Achilles tendon has a more or less flattened ellipsoid shape with the axis through maximum AP thickness frequently somewhat oblique, from antero-lateral towards postero-medial. Therefore, we decided not to measure the maximum AP thickness in the sagittal plane but rather in the transverse image, thus independent of angle of insonation. Maximum AP thickness was defined as the maximum diameter perpendicular to the maximal latero-medial width (fig. 3D). In the great majority of diseased tendons at least some increase of cross-sectional area can be observed. Therefore, it is relevant to measure the antero-posterior thickness. Aström et al27 found that a thickness over 10 mm may be related to the presence of a partial rupture. However, it should be noted that these dimensions do not provide information about the tendon structure. With the use of UTC, the dimension was measured manually; and maybe, therefore, the inter-observer reliability was not as excellent as measured by Syha et al,28 who used an automatic identification procedure. With their approach, an inter-reader variability of 3.9% was found.
UTC has clear advantages over conventional ultrasonography, as UTC directly visualises and quantifies integrity. Moreover, the grey levels in contiguous transverse echo patterns are not an absolute value but rather a relative one, namely their stability along the tendon long axis which is independent of the ultrasonographic gain settings. This stability refers to stability of the echo pattern in consecutive transverse sections and is thereby a true three-dimensional measure. Furthermore, the tracking device prevented the transducer from tilting; thus, the angle of insonation is standardised and stable. The use of the tracking and data-collection system did not only prevent a tilting artifact24 25 but also facilitated the storage and subsequent compounding of transverse images.
There are some limitations in this study. For instance, the group of symptomatic tendons had already been unsuccessfully treated with a heavy load eccentric exercise program. Öhberg and Alfredson29 reported in an observational follow-up study that all 41 tendons of 30 patients had structural ultrasonographic changes (hypoechoic area or irregular fibre structure). After follow-up (mean 28 months) with a 12-week eccentric exercise program, 37 of 41 tendons had a normalised tendon structure. It is possible that this treatment may alter the tendon structure and, therefore, result in an improved echo pattern in some symptomatic tendons. Similarly, we cannot exclude that a certain degree of degeneration could have been present in the asymptomatic group. Subjects were included simply by asking if the subjects never had complaints in the Achilles tendon region, while stricter criteria could have been used. From post mortem studies, it is known that asymptomatic tendon degeneration is present in approximately 30%.30 This may implicate that a certain degree of degeneration could have been present in the asymptomatic group. Based on the anatomical similarities between animal and human tendons,31 the UTC echo-types in human tendons can be expected to be similar to horse tendons. Further analyses that relate UTC outcomes with histology from human Achilles tendon material (eg, from patients undergoing surgery) might corroborate tissue characterisation by UTC. Reference sets for different age, gender and activity level might be needed to precisely determine the clinical relevance.
The UTC procedure could be even more standardised with standard dorsiflexion of the ankle joint and improved tracking- and data-collection device. As such, UTC might be a very useful quantitative method for the monitoring and evaluation of existing and new treatment protocols for tendinopathy. In addition, it would be very valuable to determine its prognostic value.
Conclusion
UTC was transferred from equine-validated tests to human Achilles tendons. The method showed excellent interobserver reliability and a significant difference in quantified echo-types between symptomatic and asymptomatic tendons, indicating its value for the evaluation of treatment in tendinopathy.
What is already known on this topic
▶ An ultrasonographic observation in tendinopathic tendons is the presence of a hypoechoic lesion. However, ultrasonography is essentially based on a qualitative assessment, and transducer handling and machine settings do influence echogenicity and size of the hypoechoic lesion to a large extent. Ultrasonographic tissue characterisation (UTC) is a valuable technique to quantify the integrity of tendon tissue in the horse, with histology as reference test.
What this study adds
▶ In this study, UTC was applied for the first time in human Achilles tendons. There was an excellent interobserver reliability when evaluating the images and a significant difference in quantified echo patterns between symptomatic and asymptomatic Achilles tendons.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Medical Ethics Committee METC Zuid-West Holland.
-
Provenance and peer review Not commissioned; externally peer reviewed.