Article Text

Abstract
Objectives There is no published data on the incidence or risk of SARS-CoV-2 transmission when playing golf, a sport played outdoors where social distancing is possible. The purpose of this prospective study was to report incidence and transmission regarding SARS-CoV-2, of professional golfers competing on the PGA European Tour across 23 events in 11 countries.
Methods Daily symptom and temperature checks and weekly reverse transcriptase PCR (RT-PCR) screening were performed to determine potential carriage of SARS-CoV-2. Onset and type of symptomology were analysed. Gene expression and cycle thresholds (Cts) were reviewed for all positive cases. Repeat PCR testing was performed on all positive players. RT-PCR analysis included human housekeeping genes and various RNA genes specific for SARS-CoV-2.
Results During the study period, there were 2900 RT-PCR tests performed on 195 professional golfers competing on the European Tour. Four players tested positive on-site during the study period (0.14% of tests; positive results were declared with Ct <40). Two positive tests were returned as part of routine protocols, while two reported a history of close contact with an individual who had tested positive for SARS-CoV-2 and were isolated and target tested. All were asymptomatic at time of testing, with three developing symptoms subsequently. None required hospital admission. There was no transmission from player to player.
Conclusion Golf is an outdoor sport where social distancing is possible, meaning risks can be low if guidance is followed by participants. Risk of transmission of SARS-CoV-2 can be mitigated by highly accurate RT-PCR testing of participants and by setting up a safe bubble that includes testing players and support staff, as well as all persons coming into contact with them during the course of the tournament, for example, drivers and hotel staff. This report can also provide reassurance for participants and policy makers regarding community golf, which can be encouraged for the health benefits it provides, in a relatively low-risk environment, with minimal risk of transmission by observing sensible viral hygiene protocols.
- golf
- COVID-19
- viral
- immune system
- infection
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
In 2020, European Tour golf events were subject to public health protocols aimed at decreasing transmission of SARS-CoV-2.
What are the new findings
No player-to-player transmission was demonstrated across 23 professional golf events
Robust risk assessment and control measures can enable events to be safely conducted even in locations where community transmission exists.
Policy makers and public health experts can be reassured that golf, as an outdoor sport, where social distancing is possible, carries a low transmission risk and can be safely encouraged if participants follow COVID-19 guidance drawn up by experts.
Introduction
Golf is a sport played by nearly 60 million people worldwide,1 in 206 countries,2 and its global reach was evidenced by its reinclusion into the 2016 and subsequent Olympic Games.
The COVID-19 pandemic has led to restrictions on both recreational and professional sport.
Major sporting events have considerable economic, social and wider benefits3 which, in the context of the COVID-19 pandemic, need to be balanced by any infection risks associated with the sport, as well as any concerns with associated mass gathering, travel and accommodation.4 5 Golf at the professional level is played on a number of different circuits globally. The European Tour is one of the two major men’s circuits globally, with competitors from six continents and events conducted on five continents.
For every event, the European Tour’s medical, safety and operations teams conducted a risk assessment and put in place measures to decrease risk in line with WHO best practice.6 7 Risk mitigation strategies were implemented in collaboration with the host’s national governments and public health leaders and are summarised in figure 1 (adapted with consent from Carmody et al).3 There were 23 tournaments conducted in the 2020 season from 9 July to 13 December following a period of cessation due to the COVID-19 pandemic. All constituents (players, caddies and essential support staff) were required to remain in a ‘tour bubble’ during the event week, which comprises the designated golf facilities, accommodation and transfer between these (self-drive preferred).
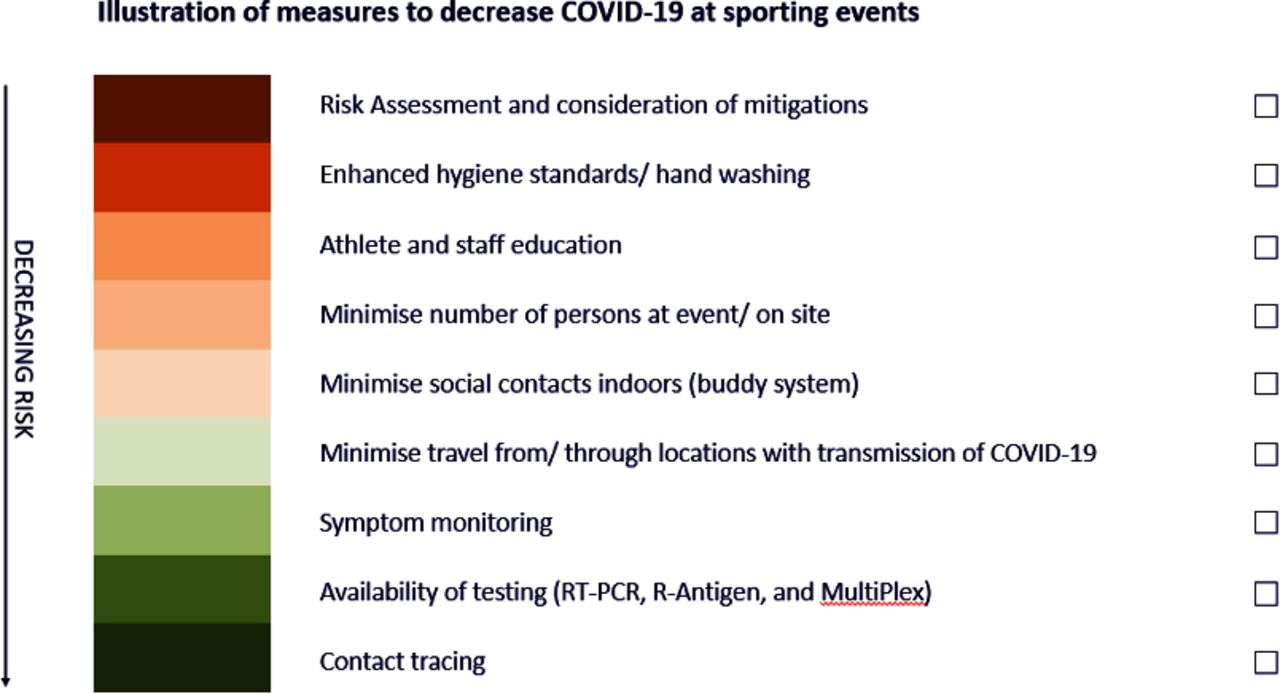
Risk mitigating measures to decrease COVID-19 rates at sporting events.
Key non-pharmaceutical interventions that were implemented at European Tour events included mandatory online education for all players, social distancing both on and off the golf course, enhanced hygiene measures, mask use when inside, and daily symptom and temperature checking. An external testing and diagnostics company (Cignpost Diagnostics) was invited to deliver reverse transcriptase PCR (RT-PCR) onsite testing using a mobile laboratory (figure 2).

The PGA European Tour mobile laboratory.
To the best of our knowledge, there are no previous data on the degree of SARS-CoV-2 transmission when playing golf or indeed any outdoor individual sport. Therefore, the purpose of this prospective study was to report the viral infective status of professional golfers competing on the PGA European Tour. These data may further inform the 60 million global golf players and policy makers regarding the risk of transmission while playing golf and highlight immediate strategies to mitigate this risk.
Methods
This prospective, observational cohort study included all players competing during 23 European Tour events during the 2020 season across 11 countries. The study period was 6 July 2020–13 December 2020. Each included player used a caddie and was allowed to forgo social distancing with this one person only. All players, including three reserves, required a minimum of one negative RT-PCR test prior to travelling to each tournament, except those attending within 90 days of a confirmed positive PCR test.
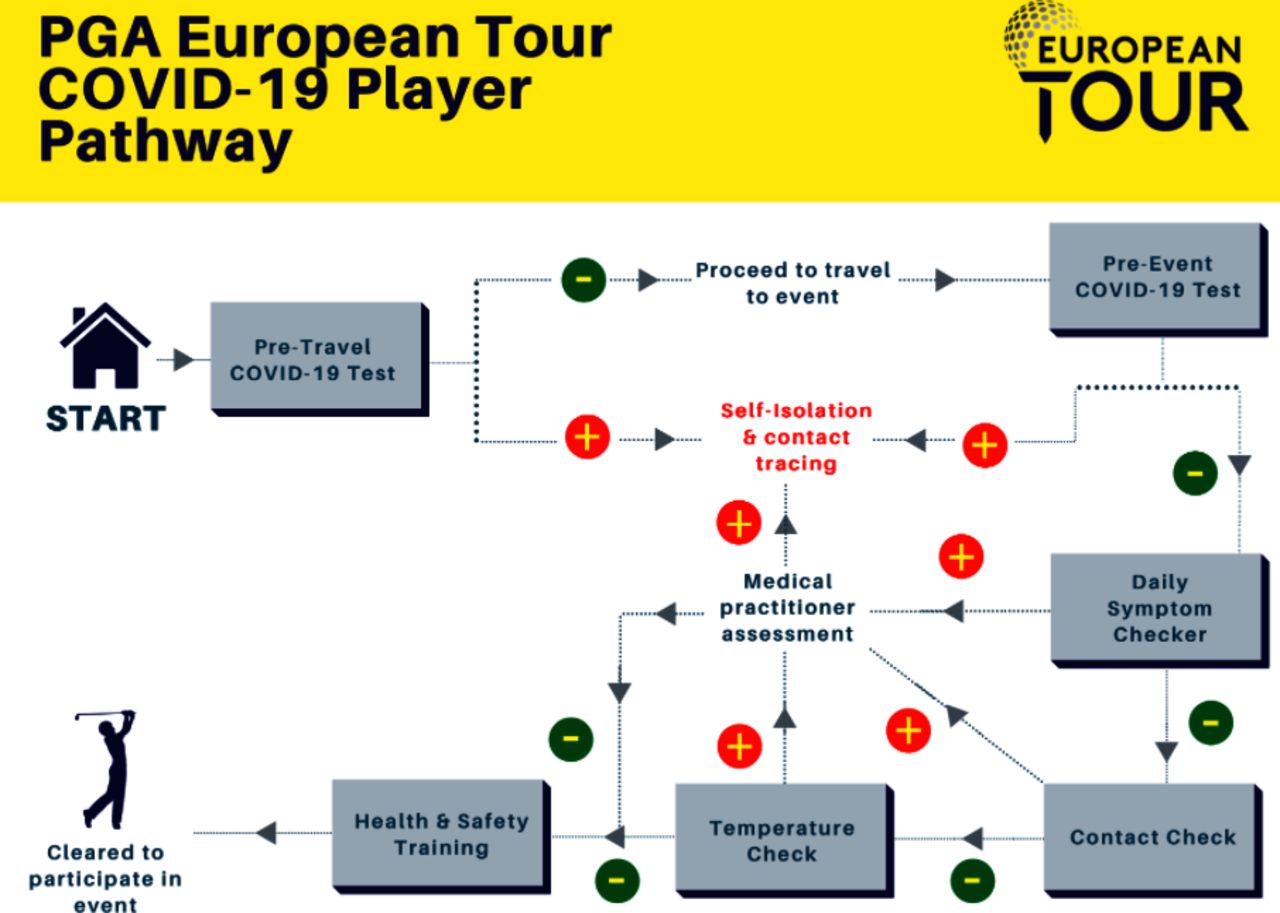
All event attendees were required to retest, on site, prior to admission. This was performed using a nasopharyngeal and oropharyngeal swab taken by a trained professional. Each day, a symptom and contact history checklist (table 1) and temperature check were performed prior to admission, and abnormalities (one answer of yes or a temperature >37.8°C) were followed up by the medical team (figure 3). Pretravel and pretournament testing, daily symptom and contact checks, and daily temperature checks were tracked through an event accreditation and tracking application (RFID, London, UK). Any abnormality was referred to the tournament infection control officer and doctor.
Player questionnaire completed before attending venue each day*
{kind=link}
{kind=link}
{kind=link}
PGA European Tour COVID-19 player pathway.
Testing and processing
Testing was conducted by Cignpost Diagnostics on the MicoBioMed (Seoul, South Korea), or Co-Diagnostics (Salt Lake City, USA) platforms, except in two countries (South Africa (Innotech) and United Arab Emirates (Mediclinic)) where testing was provided by established local laboratories. The MicoBioMed and CoDx reagent kits and thermocyclers were used and had the ability to detect virus with high sensitivity and specificity (>98%) and a limit of detection of 2.4 viral particles per microlitre. Typical run times and reporting were within 2–4 hours of swabbing. Each test assessed multiple target genes (a combination of ORF, N, S and RdRp) up to a cycle threshold (Ct) of 40 cycles. Viral levels below Ct 40 were considered positive. Indeterminate samples were repeated, where necessary. Antibody testing was not conducted systematically on European Tour.
Positive tests notification and contact tracing
All negative results were communicated by email or text to each individual. The lead technician/event doctor informed the person and host public health authority of each positive result and ensured immediate isolation and confirmatory testing. Contact tracing was conducted in line with WHO and local public health guidelines/requirements, with each contact informed and quarantined.8
Local population COVID-19 rates
All local rates of COVID-19 were reported as new cases per day per 100 000. UK data were extracted from the Office for National Statistics (ONS).9 When new cases were reported using the percentage of the population at risk, the conversion to individual daily cases per 100 000 was calculated using census data from the ONS for 2020. This applied to the tournament in Northern Ireland and the first tournament in Scotland. The national percentage was then converted into cases per 100 000 of the population. Non-UK data were extracted from the Our World in Data website in association with the University of Oxford.10
Results
One hundred and ninety-five different players representing 32 different countries entered European Tour event ‘bubbles’. Players played a mean of 15 events following recommencement of the playing season. The median number of players per event was 132 (range 65–156).
Twelve players declared a ‘contact’ on daily checking. Of these, five met the host national public health guidelines for contact tracing and were isolated and excluded from participation. Of these, three were stratified as ‘high risk’, due to sustained indoor contact (shared hotel room, shared prolonged contact at residential address and shared a meal at 1 m for >1 hour indoors). Two of these subsequently tested positive for SARS-CoV-2. The other ‘high risk’ contact had previously tested positive and subsequently tested negative throughout the remainder of the season. All other contacts, including all that had only had outdoor contact, remained negative and asymptomatic despite enhanced medical monitoring and PCR testing.
Regarding symptom checking, three out of four players who tested positive on site developed symptoms, although none required hospitalisation. A further five players declared symptoms requiring assessment but on medical assessment tested negative via RT-PCR, and a clear alternative diagnosis was made.
Over the course of 23 events, four players tested positive at an event, representing 0.14% of tests, excluding further testing of known positive cases to monitor Ct values for risk stratification. Of the four positive cases, two were detected as asymptomatic individuals on routine testing, while two players were informed they were a contact of a confirmed case (informed while on site but contact had been from prior to the event) and tested positive. One of these tested positive initially, while the other initially tested negative but became positive 2 days into isolation. All were initially asymptomatic, with three subsequently developing symptoms. All were interval tested, with the lowest Ct values for each of these four being 21.4, 24.2, 28.4 and 31.8, and all testing positive for multiple gene makers. Testing was negative for two cases on day 11, with two cases (Ct value 21.4, 24.2) returning negative on day 14 but returning intermittent results with a single positive gene (N) and Ct values 36–40 for 86 and 36 days, respectively.
Strict guidelines were provided to all players to maximise social distancing and minimising creation of contacts. There were consequently four on-site persons deemed ‘high risk contacts’ of these positive cases. They all tested negative for the SARS-CoV-2. This exposure was largely outdoor player-caddy encounters or shared meals at closer than 2 m. Further contacts were established in off-site personnel including through contact tracing of airlines in collaboration with the host public health authority. None of the players that tested positive had been inside an event tour ‘bubble’ in the week prior to their positive test.
The number of players per event and local rates of COVID-19 at the time of the tournament can be seen in table 2. Local COVID-19 rates were reported on the date of the first day of the event. If this was not available, a weekly average was used. The median number of daily cases per 100 000 of the population across 23 events was 13 (range 1–102).
European Tour events following resumption of the 2020 season, with host nation COVID-19 incidence
Discussion and comparison with the literature
Professional sporting events can have health, social and economic benefits for individuals and the wider society.3 The WHO recommend to conduct a risk assessment for COVID-19 transmission and proceed if benefits outweigh risks and if risks can be adequately controlled.6 7 For each event, the European Tour conducted a risk assessment consistent with WHO best practice and implemented strict measures in collaboration with national governments, public health authorities and other leading sports organisations. These data have immediate translational benefit highlighting that international, competitive golf can be conducted safely, achieving low rates of COVID-19 with minimal player-to-player transmission when appropriate mitigating factors are established and adhered to.
This is the first study to report on the incidence of SARS-CoV-2 detected in golf players. We have shown a very low incidence of positive RT-PCR COVID-19 tests among professional golfers competing in the European Tour. There was no evidence of player-to-player transmission, and although numbers appeared to be small, cases were typically related to sustained indoor contact with close proximity prior to on site arrival. The median rate of SARA-CoV-2 carriage at each event was lower than the host country national incidence at the time of the event. Three studies have reported the viral rates in professional team sports since the outbreak of the COVID-19 pandemic, reporting low player-to-player and in-competition transmission rates in outdoor sports in managed environments.11–13 In contrast to rugby and football, golf does not typically involve high-intensity levels of exercise, and therefore, heavy breathing is not present. This has been regarded as a known risk factor through increased production of aerosol droplets.14 In addition, the aforementioned sports involve player-to-player contact, which is not typically experienced in golf. One study assessing viral transmission from an individual, non-contact sport (squash) reported a cluster of five positive COVID-19 cases secondary to indirect transmission playing squash. All players shared the same court and squash ball.15 These findings may not be directly applicable to golf given the indoor, high-intensity nature of squash. Previous literature has reported the rate of viral recovery from contaminated sports equipment to be low,16 and we did not associate any positive cases with fomite transmission via golfing equipment.
Detection rate of SARS-CoV-2 among players in our study did not appear to be related to the national rates of detection in the host country. This confirms the success of the ‘tour bubble’ concept and the effectiveness of evidence-based, non-pharmaceutical interventions. Previous studies have conducted team sporting events in countries with daily rates of 511 and 4512 per 100 000 of the population. The median daily national rate of COVID-19 in our study was 13 with only three events taking place with rates greater than 45/100 000 and four events less than 5/100 000. When a clear link was found, cases were typically due to shared indoor space including housing or car sharing. This is in keeping with the transmission routes in professional team sports where transmission was thought to be minimal during training or matches but shared indoor environments presented higher risk than outdoor environments.11–13 17 In our study, where players reported contacts in shared outdoor space, none subsequently returned positive RT-PCR tests. When positive cases were detected, strategies were effective in identifying the positive player, implementing individual isolation and tracing appropriate contacts. This achieved cessation of disease transmission within the ‘tour bubble’. It is therefore clear that when appropriate mitigating protocols are adhered to, competitive golf can be conducted internationally with low rates of SARS-CoV-2 transmission.
Despite an international player attendance at each event, rates of SARS-CoV-2 were overall lower than the local daily rate. This is likely secondary to enhanced hygiene during travel, while transferring and while in accommodations and at the golf course. Although playing golf represents an outdoor, low-population density activity, travel (especially transit through airports and shared public transport) and hotels likely carry more risk and require comprehensive risk mitigation. Events were deliberately clustered geographically for the 2020 season, but considerable cross-border travel was still required. All athletes completed mandated COVID-19 training and were required to take an assessment on their knowledge regarding COVID-19 symptoms and measures. The number of persons within the bubble was limited to players, caddies and essential support and event delivery staff. Professional–amateur pretournament days, hospitality and spectators were comprehensively risk assessed and managed when it was agreed reasonable with national public health teams to introduce these. Within the bubble, all participants were subject to daily contact, symptom and temperature monitoring to ensure any potential cases could be identified and if necessary isolated promptly. Testing was immediately available on site, as were experienced social distancing officers, COVID-19 officers and medical staff to ensure risk mitigation strategies were put in place and to support care for affected parties and contact tracing.
Limitations
Although comprehensive in testing all players and wider personnel on site at the golf tournaments, findings are presented with caution noting limitations. Case numbers were modest, limiting the applicability of findings related to transmission. Although athletes were tested prior to leaving for an event, weekly testing was not mandated when athletes were not on tour, and practising at home, due to the low-risk environment of golf and lack of availability of testing for routine surveillance in some markets. Contact tracing is unavoidably limited by the accuracy of the information delivered by the player to the healthcare practitioners although independent verification was sought. In addition, we do not report the rates of SARS-CoV-2 transmission among staff and caddies at the event, as different databases and testing regimes were used. Incidence was low in caddies staying in the professional bubble.
Conclusion
This study is the first to report SARS-CoV-2 incidence within a professional golf environment. Using WHO and national public health guidance, events were hosted with incidence similar or lower than the general population. Adherence to non-pharmaceutical interventions such as avoiding discretionary social contacts is very important. There was no evidence of player-to-player transmission during the sporting activity, and this shows golfers can participate safely in outdoor environments. There are transmissions risks associated with tournament golf; however, these are largely away from the sport itself, related to transport and accommodation, and can be mitigated substantially. Golf itself intuitively represents a low-risk environment.
Data availability statement
Data are available on reasonable request.
Ethics statements
Ethics approval
Ethical approval was granted by the local ethics committee of Liverpool John Moores University (21/SPS/025).
Acknowledgments
Colleagues at the WHO and various international governing bodies for sport (ATP, FIFA, F1, the IOC, PGA Tour and World Rugby) were instrumental in shaping risk assessment and risk mitigation policies.
Footnotes
Twitter @docandrewmurray
Contributors PGR: data collection, data analysis, writing manuscript and final approval. AM: study idea, data collection, data analysis, writing manuscript and final approval. GC and DFK: writing manuscript and final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PGR: none. AM and GC have paid roles with The R&A, the European Tour and The Ladies European Tour. DFK is founder and chief medical officer of Cignpost Diagnostics Ltd.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.