Article Text

Abstract
Objectives The user experience, content and conditions for use of an online dance-health surveillance system (Performing artist and Athlete Health Monitor, PAHM) was examined through a focus group interview with professional ballet dancers.
Methods Nine professional dancers (56% female (n=5), average age=27.56± 5.17) completed biweekly questionnaires using the PAHM, including questions on health problems, injuries, mental complaints and illnesses. After 6 weeks, nine dancers participated in a focus group interview to investigate the user experience, content and conditions for use of the PAHM. Data were analysed using thematic analysis.
Results 25 of the 27 questionnaires were completed (response rate of 93%). Dancers were positive about using the PAHM. They recommend to clarifying the questions about pain and injury, expanding items on mental health, including items on workload, sleep, rest and nutrition, and receiving feedback regarding their own results. Dancers were reluctant regarding sharing their personal data with others. Data on an aggregated level can be shared because this might gain insight into the association between scheduling, workload and injury risk.
Conclusion The user experience of the monitor contributes to the willingness of dancers to keep using the PAHM. Dancers recommended adjusting the content in the PAHM to match their dance activities and health problems. The conditions for using the PAHM effectively within a company are a safe and trusting culture. Even though the PAHM alone cannot change the culture in a ballet company, it can play a role in the communication between staff and dancers.
- Surveillance
- Injury
- Qualitative
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary
This is the first study to investigate dancers’ perceptions regarding an online surveillance system.
In this study we use a qualitative approach for data collection and data analysis which has been underutilised in dance injury research.
We focus on the Oslo Sports Trauma Research Centre Questionnaire on Health Problems. This questionnaire has been frequently used in sport science. To our knowledge, this is the first study using this questionnaire in a surveillance system for professional dancers.
Introduction
Being a professional ballet dancer is very strenuous, as it requires intense dedication, focus and perseverance. Ballet dancers participate in long hours of training,1 consisting of repetitive movements,2 3 exceeding anatomical limitations (eg, turnout, pointe work)4 and competing for roles.5 These demands make ballet dancers prone to physical health problems,1 resulting in a high injury prevalence.6–8 Furthermore, dancers are at risk of mental health problems as a result of the high physical and psychological demands of dancing.9 10 Potential psychosocial stressors within dance are environmental conditions (eg, poor facilities), daily hassles (eg, financial concerns), role/work-specific stressors (eg, poor social support) and major life events (eg, serious injury).9 11 Physical and mental health problems can lead to discomfort, require treatment and inhibit artistic development due to absence from dance activities (ie, classes, rehearsals and performances).1 In extreme cases, they can lead to the end of a professional career.12 13
The first step towards prevention is measuring the extent of health problems.14 15 Therefore, health surveillance systems are essential, protecting dancers’ health and developing preventive measures.2 Although numerous research articles focusing on athlete injury and illness surveillance have been published in the past 10 years,16–18 studies using an online dance-health surveillance system are scarce. To our knowledge, two studies have used an online health surveillance system to monitor health problems in preprofessional and professional dancers.7 19 The majority of studies used a time loss or medical attention definition.20 One of the disadvantages of these definitions is that it underestimates the burden of injury because many athletes with overuse injuries continue to participate or do not seek medical help despite pain and reduced performance.21 22 When time loss definitions were used, about 90% of overuse injuries appeared to be missed.22 A study by Kenny et al found similar results in a dance population and concluded that the definitions of medical attention and time loss may underestimate the prevalence and incidence rates of overuse injuries compared with an all complaints definition.7 Surveillance methods recording all types of health problems, including overuse injuries, are needed to gain insight into the true burden of the problem and enables us to detect health problems in an early stage.
It is not clear how dancers, artistic staff and medical team perceive such surveillance methods in practice. Barboza et al 18 evaluated the athlete’s perceptions and expectations of such a system, but did not include dancers. Therefore, the aim of this study was to pilot the use of the Performing artist and Athletes Health Monitor (PAHM) at the Dutch National Ballet and gain insight into the user experience, content and conditions for use of an online surveillance system to monitor the health of dancers using this health monitoring system.
Method
Participants
We invited 10 dancers (4 male and 6 female) of the internationally renowned Dutch National Ballet to participate in this study. The dancers were recruited through the Work Counsel of the company. Nine of the 10 dancers (4 male and 5 female) participated in the prospective study and the focus group interview. One participant was not able to participate (reason unknown).
All dancers were informed about the procedure and provided written informed consent.
Procedures
Prospective study
Every 2 weeks, during May and June 2018 (three times in total), the dancers were asked to complete a questionnaire via the online dance-health surveillance system, the PAHM.
The PAHM was developed by Codarts Rotterdam and is used to monitor physical and mental health in preprofessional and professional performing artists and athletes.16 19 On a biweekly basis, all dancers had to fill in a minimum of 5 and a maximum of 18 items, depending on their answers. Figure 1 gives an overview of the items included in the PAHM. The PAHM included the Oslo Sports Trauma Research Centre Questionnaire on Health Problems (OSTRCQ)17 and questions on injury characteristics,23–25 general health, mental health, medication use, sleep quality and additional activities.

Flowchart of subsequent questions in the PAHM questionnaire.
It took the dancers, on average, 5 min to fill in the questionnaire on either their smartphone, laptop or personal computer. After 5 days, a reminder by email was sent to the dancers who had not yet responded to the questionnaire.
Focus group interview
A focus group interview was conducted in June 2018. Eight of the 9 dancers (3 male and 5 female) participated in this interview. In addition, one male dancer participated via a Skype interview with the researchers, as he was unable to attend the focus group interview.
Before the start of the interview, the two researchers (moderator=SCK-H, note taker=DEK) introduced themselves. The moderator explained the aim of the focus group. The dancers were asked to sign written consent forms in which they clarified that they understood the aim of the study and gave consent to audio and video taping of the session. Participants were put at ease by emphasising that there were no wrong answers and different opinions were encouraged.
The interview consisted of two parts. In the first part, participants’ personal experiences with the content of the PAHM were discussed (positive/negative experiences, frequency and (long-term) user-friendliness, length of the questionnaire, importance of the items and missing information). In the second part of the interview, participants were shown outcomes of the biweekly data collection at the Dutch National Ballet and results of a study that used the PAHM in contemporary dance students.19 Participants were asked to provide feedback regarding the use of the PAHM on these two different settings (which information should be included, how should this information be visualised, what is valuable information and how to share information and with whom). Finally, dancers were asked if they wanted to share any additional information.
After 1 hour, the interview was completed and dancers were thanked for their participation.
Analysis
The audio recordings of the focus group interview, as well as the Skype interview, were transcribed verbatim. Video recordings were used to add information about linking the identity of the participants to the different quotes, and to check for non-verbal cues (ie, nodding by other participants). The transcriptions were analysed using thematic analysis.26 Using this qualitative analysis method, two researchers (DEK and SCK-H) both read all the transcripts and individually selected relevant quotes from these transcripts, which they coded with a short description (eg, ‘objective feedback,’ ‘ignore injury’). After that, the two researchers compared the individually coded quotes and grouped them into similar codes. Themes were identified based on the similar codes, and these subthemes and main themes were reviewed and named.
Results
Nine of the 88 dancers of the Dutch National Ballet completed the biweekly questionnaires and participated in the focus group interview. Participant demographics and company information are presented in table 1.
Company information and participant demographics
The top three performances during the 2017–2018 season were Narnia (25 performances), Ode to the Master (23 performances) and The Sleeping Beauty (17 performances).
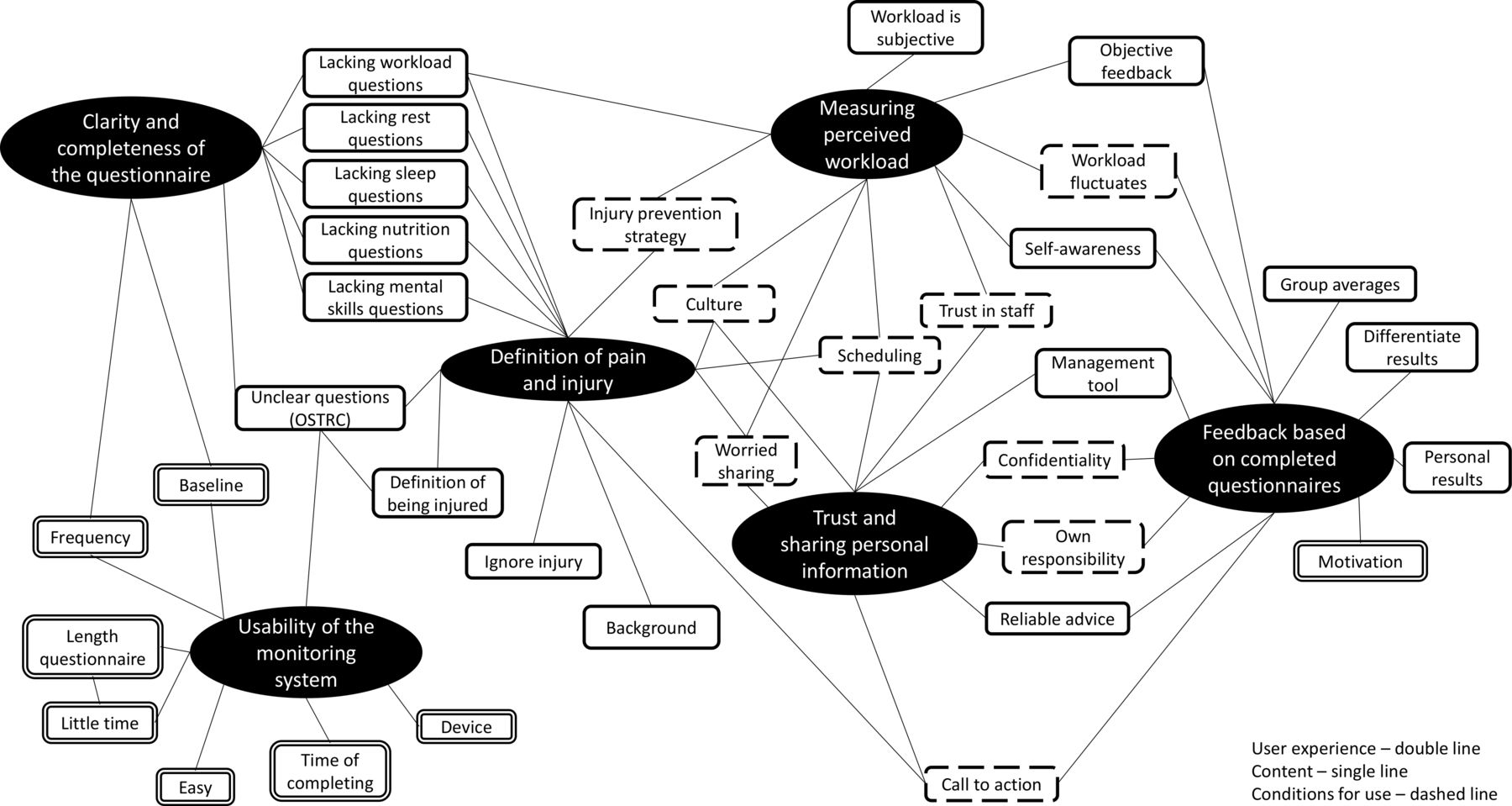
A total of three main themes and six subthemes were identified. The main themes were user experience, content and conditions for use; their respective subthemes are usability of the monitoring system and feedback based on completed questionnaires; clarity and completeness of the questionnaire, feedback based on completed questionnaires and definitions of pain and injury; trust and sharing personal information, definitions of pain and injury, and measuring perceived workload.
Figure 2 gives a graphical representation of the themes and related codes.
{kind=link}
{kind=link}
Quotes from the transcripts with a similar meaning were grouped in a code, which are the rectangle white boxes. The codes were reviewed for patterns or themes. Six subthemes were found, which are the black ovals. The lines between codes and subthemes show which codes belong to which subthemes. Several codes belong to two or three subthemes. The differentiation in lines of the boxes of the codes indicates to which of the main themes the codes belong.
Usability of the monitoring system
All dancers agreed that it was convenient to use the PAHM, as the questionnaire could be filled in quickly and the number of questions was suitable. Nevertheless, several questions were unclear (see the Clarity and completeness of the questionnaire section). The favourite device to fill in the questionnaire was a mobile phone; all dancers used their mobile phone several times to complete the questionnaire. Only a few used their personal computer at home to complete the questionnaire.
During the study, the dancers received the questionnaires every 2 weeks. Dancers indicated that they preferred to complete the PAHM on a weekly basis because they assumed that a higher frequency will provide more insight into the association between injuries and workload. One dancer stated:
So much happens in 1 month in terms of… it can be so different. In the beginning, you know, 2 weeks, maybe you have a lot of shows and then again, you have a week off or something. (P2)
The dancers also suggested to receive the questionnaires at fixed moments during the week, so that completing the questionnaire becomes a routine. Dancers preferred to receive the questionnaire on Fridays, which enables them to reflect on that particular week and indicated they are willing to continue using the PAHM.
Clarity and completeness of the questionnaire
The OSTRCQ questions (the first four questions in figure 1)17 were unclear to most of the dancers. Dancers stated that these questions were not applicable to their dance activities. The dancers recommended to differentiate between dance classes, rehearsals and performances because missing a class is less of a problem than missing rehearsals or performances. Nevertheless, information regarding missing classes was important according to dancers because health problems leading to absence from classes may worsen and lead to subsequent absence from rehearsals or performances. One of the dancers illustrated:
It is really usually like this that if you start to have pain, the first thing you do (…) is to do a little bit less in class. (…) And if people stop doing classes to the end, then it means that they are already overloaded. (P4)
Dancers also indicated that the following questions were redundant and unnecessary to repeat in each questionnaire: medication use, additional activities (eg, yoga, physiotherapy) and medical background. Furthermore, dancers indicated that the PAHM questions mainly focus on physical health problems. They suggested additional items on workload, mental health, rest and sleep quality, and nutrition to get a more complete picture of a dancers’ overall health.
Definition of pain and injury
All dancers faced difficulties in deciding whether a physical health problem was an injury or not. Dancers experiencing pain during the data collection period of 6 weeks stated that they were still able to perform and therefore did not classify the health problem as an injury. Some dancers indicated that it was difficult to answer the questions honestly and chose to give a more positive answer than reality in order to feel better or pretend that there were no issues. Furthermore, some dancers continued participating in class and rehearsal despite the pain, because of the fear that they might not be selected for the next dance performance. One of the dancers stated:
Maybe not necessarily meaning they are not dealing with an injury, but just that they are choosing to ignore it at the moment, because they want to perform next month. (P9)
Measuring perceived workload
Although dancers agreed that monitoring their workload would be valuable, they acknowledged it was difficult to present results on workload appropriately. Workload averages led to a distorted picture as the different ranks have very different workloads. Therefore, dancers recommended to differentiate results between ranks and gender. Moreover, dancers stated that experienced workload was subjective because all dancers might have been answering the question differently, and even if the rehearsals were not physically demanding, it might still be tiring and mentally demanding. Dancers felt that the scheduling of the programme was the biggest problem influencing workload. Due to the schedules, dancers felt they did not have enough time to recover from heavy programme, which led to an increased risk of injuries. A dancer illustrated:
Maybe how much the dancers feel the injury that they might be dealing with… eh… is connected to… a… something work related, like whether it’s like, oh, I think I am injured like this because of the kind of work we are doing right now, like we’re rehearsing too much or, we’re not getting enough break time… (P9)
Feedback based on completed questionnaires
During this pilot, the biweekly response rate of the PAHM was 93% (range 90%–100%). During the study, dancers did not receive any feedback from the monitoring system. However, dancers suggested that receiving personal feedback was a good incentive to fill in the questionnaire each week for a longer time span. Feedback would have made dancers more self-aware about their health. Moreover, based on their personal results, dancers would have liked to receive reliable advice and a call to action, for example, on how to maintain their good results or work on their points of improvements. Dancers preferred that this advice or call to action comes from external parties, for example, a research institution.
Because I realize also, when I haven’t been well for two months… But I don’t know what to do, we just keep going, and then we have the same thing of where we just keep going and going. Right? I would be interested in knowing what to do then. (P8)
The dancers were positive about sharing data on an aggregated level, which would have provided dancers with the opportunity to compare their own results to the results of the group, and could be used as a management tool for the staff. Dancers expressed their wish that these data would be used to provide the staff with better insights into the association between scheduling and injury.
Trust and sharing personal information
Dancers worried about sharing personal information regarding their health status. Dancers were reluctant to fill in that they were injured or in pain. They were afraid the artistic and medical staff would use this information to decide which dancers will be selected for specific roles and performances. One of the dancers stated about using the PAHM:
I really hope that I will fill in the … that thing … very honestly, if I am 100% sure that the information cannot be used against me. (P4)
They felt it was their own responsibility to see their family doctor or psychologist.
Discussion
The focus of this paper was on the user experience, content and conditions for use of an online health surveillance system (ie, the PAHM). These three main themes are discussed below.
User experience
Dancers indicated they were willing to continue using the PAHM. They evaluated the usability of the PAHM as good and user-friendly because the layout of the monitoring system provided an easy way to answer the questionnaire. Furthermore, filling in the PAHM did not require a large time investment, and dancers could use their phones to complete the questionnaire. Dancers stated that they would prefer to complete the PAHM weekly to minimise recall bias.
During this pilot study, dancers missed feedback that would have motivated them to fill in the PAHM. These findings are in agreement with a study on the perceptions of end-users towards an online sports-health surveillance system.18 Nevertheless, the dancers were positive about monitoring their health problems. They stated that they became more aware of their own physical and mental health, as they evaluated their health regularly, and would have liked to improve their general health and prevent overuse injuries through advice based on the PAHM data.
Content
When evaluating the content, the dancers indicated that they would like to have more (extended) questions about mental health, workload, sleep, rest and nutrition. Dancers were aware of the fact that including additional items will result in a longer questionnaire. However, they indicated a few more questions would be beneficial to monitor their health problems, as long as they could still complete the questionnaire in approximately 5 min.
Moreover, the definition of being injured was unclear. We used the ‘all complaints’ injury definition that has been used in sports injury research.20 Using an ‘all complaints’ definition as opposed to the narrower ‘time-loss’ and ‘medical attention’ definitions allowed us to gain insight into all health complaints, which enabled us to detect health issues at an early stage.27 28 However, dancers felt that pain and injuries are different constructs. As a result, the dancers were uncertain on how to answer the questions.
Lastly, the dancers stated that the OSTRCQ questions were not specific enough and detailed enough. This is in disagreement with the results from a study using the OSTRCQ in preprofessional and contemporary dancers.7 We recommend to carefully tailor or fully replace the OSTRCQ with more specific questions, for example, by differentiation between class, rehearsal and performance. We are aware that any changes to these questions might influence the validity of the questionnaire.
Conditions for use
We found that the dancers would like to receive personal feedback, containing alarms or calls to action. Nevertheless, they were hesitant about sharing their results with company staff. The reason for this was that the dancers were concerned that negative results might impact their opportunities for roles and dancing. This is in line with the worries of dancers in other dance companies and students.5–7 10 A striking finding was that while we did not share the data from the PAHM with the company staff, dancers still indicated they were hesitant to fill in their ‘pains’ and ‘issues’.
According to the dancers, sharing PAHM data on an aggregated level with the staff was an opportunity to create a management tool that gains insight in the load and load management of dancers. Using personal data may help to adjust the training and workload for each individual dancer, for example, as is shown by Barboza et al 18 and Clarsen et al 17 in sports. Such an approach is impossible when only aggregated data are used. In an ideal and healthy company culture, personal data would be respectfully shared to keep the injury prevalence low. However, this is currently not the culture observed within dance companies.5 6 29
Dancers may be more likely to open up and be willing to share personal data in a safe and trusting culture. Although this cannot be changed by using an online health surveillance system alone, we do feel that the objective data collected with the PAHM may serve as a first step in discussing the needs of both the dancers and the management.
Limitations
Nine dancers participated in a study lasting 1.5 months. The short duration of the study was adequate for evaluating the dancers’ experiences and expectations of using the PAHM in order to make improvements before distributing the monitoring system to all dancers in the company. We conducted the study in only one company; therefore, our findings might not be generalisable to other companies. Nevertheless, the dancers’ experiences of pain, injuries and trust are in line with previous research.5–7 10 29
The focus group interview lasted for 1 hour, and the Skype interview lasted 30 min. In personal interviews, participants are able to give more information on the topic. However, we decided to conduct a focus group interview to start a discussion about the questions in the PAHM and to gain a deeper insight into the participants’ viewpoints and let them learn from each other. After the focus group interview, the dancers did not have further remarks or questions about the PAHM.
Findings of this study will be used to improve the PAHM before introducing the online dance-health surveillance system to all dancers of the company.
Practical implications
The current study was carried out to gain insight into the user experience, content and conditions for use of the online dance-health surveillance system PAHM. Participant suggestions for the next iteration of the PAHM were as follows:
Topics to be covered in the questionnaire are pain/injury (and definitions of those), mental complains, workload, rest and sleep and nutrition.
The questionnaire should be adjusted to reflect the professional context of the dancers, for example, by differentiating between class, rehearsal and performance.
Dancers preferred to receive personal feedback in a personal overview. These individual data should not be shared with company staff.
Dancers stated that they do not foresee any problems with sharing data on an aggregated level.
The frequency of filling in the questions should be changed from biweekly to weekly.
Conclusions
Nine dancers of the Dutch National Ballet used the online dance-health surveillance system (ie, PAHM) for 6 weeks. The user experience of the PAHM contributes to the willingness of dancers to keep using the online dance-health surveillance system. The dancers appreciated that the PAHM questionnaire was short to fill in and could be completed using a phone. However, dancers would have preferred to receive personal feedback on their answers containing alarms or calls to action. Dancers recommended adjusting the content in the PAHM to match their dance activities and health problems, such as expanding the questions on mental health, workload, rest and sleep and nutrition. A clear injury definition would help dancers on how to answer the questions. A safe and trusting culture are conditions for using the PAHM effectively. Even though the PAHM alone cannot change the culture in a ballet company, this online dance-health surveillance system can serve as a tool in discussing the needs of both the dancers and the management by providing insights into the association between scheduling and injury prevalence. The results of this focus group will be used to further develop the PAHM.
Acknowledgments
We would like to thank the dancers of the Dutch National Ballet who participated in the study and the focus group interview for their participation, open attitude and insightful remarks.
References
Footnotes
Contributors All three authors made a substantial contribution to the information and material submitted and have read and approved the final version. DEK and SCK-H collected and analysed the data. DEK wrote the manuscript. SCK-H and JS contributed to the content of the article.
Funding This study was supported by National Association of Applied Sciences SIA (SPR.VG01.007).
Competing interests None declared.
Patient and public involvement statement Participants who took part in this study received feedback on the results.
Patient consent for publication Not required.
Ethics approval The Dutch Central Committee on Research Involving Human Subjects (CCMO) stated that no medical ethical approval was necessary for this questionnaire study, as stated in the Dutch Medical Research Involving Human Subjects Act (http://www.ccmo.nl/nl/toetsingscommissie-ccmo-of-metc?55a37b93-dd8c-4bf8-8883-2d30c35ff8ba).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.