
Abstract
Background
People today are living longer and want to remain active. While obesity is becoming an epidemic, the number of patients suffering from osteoarthritis (OA) is expected to grow exponentially in the coming decades. Patients with OA of the knee are progressively being restricted in their activities. Since a knee arthroplasty (KA) is a well accepted, cost-effective intervention to relieve pain, restore function and improve health-related quality of life, indications are expanding to younger and more active patients. However, evidence concerning return to sports (RTS) and physical activity (PA) after KA is sparse.
Objectives
Our aim was to systematically summarise the available literature concerning the extent to which patients can RTS and be physically active after total (TKA) and unicondylar knee arthroplasty (UKA), as well as the time it takes.
Methods
PRISMA guidelines were followed and our study protocol was published online at PROSPERO under registration number CRD42014009370. Based on the keywords (and synonyms of) ‘arthroplasty’, ‘sports’ and ‘recovery of function’, the databases MEDLINE, Embase and SPORTDiscus up to January 5, 2015 were searched. Articles concerning TKA or UKA patients who recovered their sporting capacity, or intended to, were included and were rated by outcomes of our interest. Methodological quality was assessed using Quality in Prognosis Studies (QUIPS) and data extraction was performed using a standardised extraction form, both conducted by two independent investigators.
Results
Out of 1115 hits, 18 original studies were included. According to QUIPS, three studies had a low risk of bias. Overall RTS varied from 36 to 89 % after TKA and from 75 to >100 % after UKA. The meta-analysis revealed that participation in sports seems more likely after UKA than after TKA, with mean numbers of sports per patient postoperatively of 1.1–4.6 after UKA and 0.2–1.0 after TKA. PA level was higher after UKA than after TKA, but a trend towards lower-impact sports was shown after both TKA and UKA. Mean time to RTS after TKA and UKA was 13 and 12 weeks, respectively, concerning low-impact types of sports in more than 90 % of cases.
Conclusions
Low- and higher-impact sports after both TKA and UKA are possible, but it is clear that more patients RTS (including higher-impact types of sports) after UKA than after TKA. However, the overall quality of included studies was limited, mainly because confounding factors were inadequately taken into account in most studies.
Similar content being viewed by others

Return to sports is possible after knee arthroplasty, but seems more likely after unicondylar arthroplasty than after total knee arthroplasty, particularly concerning higher-impact types of sports. |
In the included studies, little attention was given to possible confounding factors, such as preoperative sports level, restricting comorbidities, and negative advice from surgeons. |
We recommend generalising the definition of the assessment of the preoperative sports level to the ‘presymptomatic phase’, as this plays an important role in defining return to sports percentages. |
1 Introduction
Patients with knee osteoarthritis (OA) are progressively restricted in their daily functioning, working and sports activities, making them less active than they would like to be. A knee arthroplasty (KA) is a well accepted, reliable and suitable surgical procedure for end-stage OA patients to relieve pain, to return to function, and to improve health-related quality of life [1]. However, literature concerning the extent to which patients can return to sports (RTS) and physical activity (PA) after both total (TKA) and unicondylar knee arthroplasty (UKA) is sparse.
People are not only living longer than before, they also want to stay active and engaged in their working activities up to and after retiring [1, 2]. According to demographic projections in the Netherlands, it is expected that the number of OA patients will increase exponentially between 2007 and 2040. Subsequently, an increase in KAs of 297 % from 2005 to 2030 is envisaged, resulting in 57,900 KAs annually in 2030 [3]. This increase is not only due to more, relatively younger patients with knee OA that want to preserve an active lifestyle without knee pain, but also to the growing burden of the obesity epidemic. For example, in the US, the demand for primary KAs is estimated to grow even more, by 673 % from 2005 to 2030, leading to 3.5 million annual procedures [4].
There is overwhelming evidence that a sedentary lifestyle is undeniably one of the most serious health problems of the 21st century [5, 6]. As a consequence, people’s wish to stay active has been stimulated by several leading international organisations that have recognised the positive effects of PA in general. International guidelines of health-enhancing PA levels have been developed and ‘exercise is medicine’ is proclaimed, by stating that PA can ameliorate affluence-related chronic diseases such as cardiovascular disease, diabetes mellitus and cancer [7]. Moreover, PA has proven to have beneficial effects on bone quality and implant fixation [8].
Since the prevalence of OA affecting the knee is rising rapidly, this disease is currently one of the leading causes of disability in adults. Due to osteoarthritic pain, physical deconditioning arises, resulting in reduced endurance for exercise, less aerobic capacity, less muscle strength, and a high risk for being overweight. Consequently, individuals with OA greatly fall short of the public health PA guidelines [9]. The possible benefits of total knee replacement in terms of pain relief and restoration of function are well documented, but impacts on health, fitness and the lower risk for coronary heart disease have also been addressed in patients who had been able to resume activities after KA [10]. Even a possible cardioprotective benefit of primary total joint arthroplasty has been described with an absolute risk reduction of 12.4 % of serious cardiovascular events after KA [11].
Furthermore, total TKA is a cost-effective medical intervention, especially concerning the younger working population suffering from OA of the knee [12, 13]. In addition to TKA, new techniques and improved implant quality of UKA have given rise to the treatment of end-stage OA of the knee. The theoretical advantages of UKA compared with TKA are that the procedure is less invasive, patients tend to achieve a better range of motion, and report a joint as feeling ‘more normal’ [14].
As a consequence of higher patient expectations regarding activities after knee replacement, clinicians are increasingly forced to question how much sports activity a patient can participate in after knee replacement, and what kind of sports activities are acceptable [15, 16]. All doctors, but especially sports medicine physicians and orthopaedic surgeons, should counsel patients regarding an active lifestyle, including when they have to undergo KA. However, synthesised data to provide reliable answers to the questions of end-stage OA patients regarding sports activities after knee replacement are lacking. Most available recommendations, such as The Knee Society consensus recommendations of 1999, are based on expert opinions from surveys rather than on evidence-based summaries of good quality research [17–21].
However, as patients are increasingly participating in a shared decision-making process, clinicians are expected to inform and advise them according to scientific knowledge rather than ‘gut feelings’. Consequently, the aim of this review is to systematically summarise the available scientific literature on our research questions. Our primary research question is ‘to what extent do patients RTS after total and unicondylar KA, and how long does this take?’. Our second research question is ‘to what extent can patients return to PA after total and unicondylar KA?’
2 Methods
2.1 Search Strategy
The PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) statement was used for this systematic review [22]. A research protocol for this review was agreed by all co-authors before starting the literature searches. The study protocol was published online at the PROSPERO International prospective register of systematic reviews (http://www.crd.york.ac.uk/PROSPERO/) under registration number: CRD42014009370.
The electronic databases MEDLINE (biomedical literature) via PubMed, Embase via OvidSP, and SPORTDiscus (sports and sports medicine literature) via EBSCO were searched for relevant literature. Searches were performed up until January 5, 2015. In all three databases the following three categories of keywords (and related synonyms) were used to build a sensitive search strategy and to provide a systematic search: ‘knee arthroplasty’, ‘sports’ and ‘recovery of function’. In MEDLINE we strived to use medical subject headings (MeSH), otherwise we searched the title and/or abstract (tiab). Furthermore, search terms were truncated through the use of a * symbol in order to find all terms beginning with a specific word. Within each keywords category, the different synonyms were combined using the Boolean command OR, and categories were linked with the Boolean command AND. The exact details of the search strategy can be found in the electronic supplementary material, Appendix S1.
2.2 Inclusion Criteria and Study Selection
The first author (SW) selected suitable studies with the assistance of a medical student and input from a medical librarian of the Academic Medical Centre (AMC). Inclusion criteria were (1) knee OA patients who underwent total and/or unicondylar KA; who (2) were active in a sport before the surgery and intended to resume or intensify their sporting activity; and (3) that included an outcome measure of interest to the authors. The primary outcome was the percentage (and number) of patients to RTS (preferably described in terms of sports level, duration and frequency) and time to RTS. Secondary outcomes were specific PA outcomes measures, namely University of California, Los Angeles (UCLA) rating score, Tegner-Lysholm rating scale and Grimby score [23–25].
The reference lists of selected articles were screened to identify additional articles to be included. We also performed a forward search using ‘Web of Science’ to see which of these papers were referred to by other papers after they had been published.
2.3 Methodological Quality
We assessed the risk of bias of the studies using the Quality in Prognosis Studies (QUIPS) tool [26]. This quality assessment method considers six domains of potential biases: (1) study population; (2) study attribution; (3) prognostic factor information; (4) measurement of and controlling of confounding variables; (5) measurement of outcomes; and (6) analysis approaches. The first author (SW) assessed the quality of all selected articles, and this was repeated by two other authors (VG and PK), who each assessed risk of bias of 50 % of the selected articles. We customised the tool to our review by defining the issues of the domains to be scored. The details of these issues can be found in the electronic supplementary material, Appendix S2. In domain 2, we adjusted for a minimum follow-up period of 1 year, according to the literature, which states that the greater part of the knee function will have been regained at 1 year after surgery [27–29].
By assessing response rate and information about non-responders, we chose a cut-off point of 20 %, based on previous studies in this field [30, 31]. In domain 5, concerning study confounding, we identified confounding variables for activity from previous research we found on this subject before performing this systematic review [1, 28, 32–35]. We rated the issues per domain separately as ‘yes’, ‘no’, ‘partial’ or ‘unsure’, which then led to a risk of bias for each domain to being ‘low’, ‘moderate’ or ‘high’. We considered a study to have an overall low risk of bias when the methodological risk of bias was rated as low or moderate in all six domains, with at least four domains being rated ‘low’. A study was rated as having an overall high risk of bias if two or more of the domains scored ‘high’. In-between quality was scored as ‘moderate’.
2.4 Data Extraction
The first author (SW) extracted data from all selected original articles, and this was repeated by two other authors (VG and PK), each extracting data from 50 % of the included articles.
All authors used a standardised data extraction form including the following topics: (1) study information: author, year, country and reference number; (2) study design and follow-up; (3) information about study population: cohort, population size, sex, age, body mass index (BMI), comorbidities, and type of OA (primary or secondary causes, such as systematic inflammatory disease or post-traumatic arthritis); (4) description of rehabilitation protocols used; (5) definition of the outcome measures; (6) preoperative activity and definition (e.g. presymptomatic or at time of surgery); (7) postoperative activity; (8) RTS percentages and time to RTS; and (9) confounding factors taken into account for RTS, such as sex, BMI, restricting comorbidities, complications, preoperative sports level, surgeon recommendations or other psychosocial influencing factors.
2.5 Pooling Data
From the studies that described pre- and/or postoperative participation in specific types of sports and/or times to RTS, data were pooled and categorised into low-, intermediate- or high-impact sports, according to the levels of impact on the knee joint (see electronic supplementary material, Appendix S3). This classification is in compliance with Vail and Mallon [36] and supported by a biomechanical study from Kuster et al. [37], in which both peak loads and flexion angles of the knee were considered. We calculated pooled RTS percentages by comparing pooled pre- and postoperative sports participation data.
3 Results
3.1 Literature Search
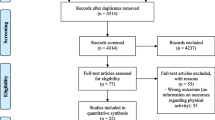
We retrieved a total of 1115 potentially relevant citations from our search. After deleting 286 duplicates and applying the inclusion criteria to titles and abstracts, we reviewed 37 full-text articles, 12 of which were review articles. We excluded these from data extraction, as with 14 other articles, which were excluded for various reasons such as current concept reviews, case reports or studies not presenting outcomes of our interest. On both reviews and the included 11 articles, we performed reference screening and forward citation tracking, which resulted in seven additional articles being included. The article by Jahromi et al. [38] was excluded because the same UKA cohort was described in the article by Walton et al. [39]. Finally, 18 original studies were included. The PRISMA flowchart of our search procedure can be found in Fig. 1.

PRISMA flowchart of search strategy. THA total hip arthroplasty, TKA total knee arthroplasty
3.2 Included Studies
All of the included studies were observational, 13 being cross-sectional studies, three prospective studies and two retrospective cohort studies. Two studies were performed in Australia [39, 40], one in Austria [41], two in France [42, 43], four in Germany [44–47], one in Italy [48], one in Korea [49], one in Switzerland [14], four in the UK [50–53] and two in the US [54, 55]. From three of the 18 included articles, data about sports activities after both TKA and UKA was able to be extracted, from ten after TKA and from five after UKA, of which one article specifically described outcomes after lateral UKA. Of the 13 articles with respect to data about RTS after TKA, the study population of eight studies was a non-selected group of KA patients. Five studies examined a selected population of patients. Two of these studies examined patients younger than 75 years old, one study assessed patients younger than 65 years old, another study concerned non-revised patients younger than 55 years old and the last study evaluated licensed judokas (i.e. people who participate in judo, which is a method of defending oneself or fighting without the use of weapons, based on jujitsu) with black belts of 60 years and older.
This latter study described outcomes of two different age groups, namely patients younger than 55 years and patients aged 65–75 years. Of the eight articles with respect to data about RTS after UKA, seven studies examined a non-selected cohort and one study examined a cohort of patients younger than 75 years old.
The total number of patients in the 13 TKA cohorts was 3261 and the mean age of these patients varied between 49 and 73 years at time of surgery, with ranges from 21 to 96 years. Mean BMI varied from 27 to 34 kg/m2 with ranges from 16 to 44 kg/m2, but was clearly described in three of the 13 included studies. Only three of the 13 studies provided information concerning possible restricting comorbidities on levels of PA. Five of the 13 studies provided information about the rehabilitation protocols followed.
The total number of patients in the eight UKA cohorts was 662. The mean age at time of surgery of these patients varied between 59 and 72 years, with ranges from 21 to 95 years.
The BMI of the patients was specified in three of eight UKA cohorts and was described as means of the total cohort of 26 and 28 kg/m2 (range 20–42) and Pietschmann et al. [46] described a mean BMI in active patients of 28 kg/m2 (range 20–56) and in inactive patients of 29 kg/m2 (range 19–43). Fisher et al. [51] took into account medical problems restricting PA after UKA and four of eight studies provided information about the rehabilitation protocols. The results of the data extraction are presented in Table 1 for articles concerning data of RTS after TKA and in Table 2 for articles concerning data of RTS after UKA.
3.3 Methodological Quality
Three of the 18 studies, namely Bradbury et al. [50], Huch et al. [44] and Naal et al. [14], were rated as having a low risk of bias, nine were scored as moderate [40, 41, 45–47, 49, 51, 52, 54] and six as high [42, 43, 48, 55]. It was notable that most studies provided no information about possible confounding factors, as six studies scored ‘high’ and eight studies ‘moderate’. The lowest risk of bias was found for the prognostic factor in which the type of prosthesis was described. No study scored a ‘high’ risk of bias in that domain. A summary of all scored risks of bias per domain is listed in Table 3.
3.4 Return to Sports (RTS)
Eight of the 13 studies reported data about the percentages of patients who RTS after TKA. Mean percentages of RTS varied from 36 to 89 %. Huch et al. [44] described two possible percentages of RTS depending on which moment the preoperative sports participation percentage was chosen. They found that 94 % of the patients were active in sports preoperatively ‘during life’, but only 36 % of the patients were still active in sports ‘at time of surgery’. Hence, the rates of RTS after TKA compared with these two different preoperative percentages were 36 and 81 %, respectively. Nine of the 13 TKA studies clearly defined the time period of scoring the preoperative sports participation. Argenson et al. [42] defined the preoperative sports moment as ‘at the time of surgery’ (RTS 86 %), Wylde et al. [53] used ‘3 years before surgery’ (RTS 73 %) and Lefevre et al. [43] and Huch et al. [44] used ‘participation during life’ (RTS 63 and 36 %, respectively) as the preoperative sports moment.
Seven of the nine studies reported the overall percentages of patients who RTS after UKA. Mean percentages of RTS varied from 74 % to more than 100 %, meaning that more patients participated in sports postoperatively than preoperatively. Four of these seven studies clearly described that the time period for the preoperative sports participation level was at the ‘presymptomatic phase’ with described RTS percentages of 93, 95, 98 and 75 % [14, 47, 51, 53].
3.5 Pooling of Data of Sports Participation, RTS and Time to RTS
3.5.1 Pre- and Post-Operative Sports Participation and RTS
Data of ten TKA studies could be pooled (Table 4). Preoperatively, 1436 patients performed some type of low-impact sports a total of 1265 times. These sports included walking, swimming, golf and cycling (mean of 0.9 sports per patient), while 202 patients participated in an intermediate-impact type of sports, such as hiking, mountain climbing and downhill skiing (mean of 0.1 sports per patient), and 107 took part in a high-impact type of sport (mean of 0.1 sports per patient), such as running, tennis and ball sports.
In total, these 1436 patients practised preoperatively an average of 1.1 sports per patient, of which 80 % were low impact, 13 % were intermediate impact and 7 % were high impact. Postoperatively, 1524 patients performed some type of low-impact sports 1262 times (mean of 0.8 sports per patient), 132 a type of intermediate-impact sport (mean of 0.09 sports per patient) and 51 a type of high-impact sport (mean of 0.03 sports per patient). In total, these 1524 patients practised postoperatively an average of 0.95 sports per patient, of which 87 % were low impact, 9 % intermediate impact and 4 % high impact. RTS after pooling resulted in 94 % of patients returning to low-impact sports, 64 % to intermediate-impact sports and 43 % to high-impact sports. Two included studies for pooling were rated as having a low risk of bias [44, 50]. Pooled data from these two studies resulted in 337 sports practised by 549 patients (mean of 0.6 sports per patient: 58 % low impact, 25 % intermediate impact and 17 % high impact) preoperatively. Postoperatively, these 549 patients practised 155 sports (mean of 0.3 sports per patient), of which 85 % were low impact, 8 % intermediate impact and 7 % high impact. Two of the pooled studies used a similar definition of the time of the assessment of the preoperative sports level, namely ‘during life’ [43, 44]. Pooling of these data resulted in 398 patients performing a total of 209 sports preoperatively (mean of 0.5 sports per patient: 50 % low impact, 39 % intermediate impact and 11 % high impact). Postoperatively, 396 patients performed 93 sports (mean of 0.2 sports per patient), of which 79 % were low impact, 13 % were intermediate impact and 8 % high impact. All pooled data, specified by impact of sports, are summarised in Table 4.
Data of seven UKA studies were pooled (Table 4). Preoperatively, 509 patients practised some type of low-impact sport 612 times (mean of 1.2 sports per patient), an intermediate-impact sport 237 times (mean of 0.5 sports per patient) and a high-impact sport 91 times (mean of 0.2 sports per patient). In total, these 509 patients practised preoperatively an average of 1.9 sports per patient, of which 70 % were low impact, 22 % intermediate impact and 8 % high impact. Postoperatively, 562 patients performed some type of low-impact sports 629 times (mean of 1.1 sports per patient), an intermediate-impact sport 155 times (mean of 0.6 sports per patient) and a high-impact sport 33 times (mean of 0.1 sports per patient).
In total, these 562 patients practised postoperatively an average of 1.5 sports per patient, of which 77 % were of low impact, 19 % of intermediate impact and 4 % of high impact. RTS after pooling resulted in 93 % of patients returning to low-impact sports, >100 % of patients returning to intermediate-impact sports and 35 % to high-impact sports. There was only one article with a low risk of bias which could be included for pooling of data [14]. In this study, 83 patients practised 381 sports preoperatively (mean of 4.6 sports per patient: 49 % low impact, 36 % intermediate impact and 15 % high impact). Postoperatively, 238 sports were still being practised by these 83 patients (mean of 2.87 sports per patient), of which 64 % were low impact, 32 % intermediate impact and 4 % high impact. Three of the pooled studies used a similar definition of the time of the assessment of the preoperative sports level, namely ‘before the onset of any restricting knee symptoms’ [14, 47, 51]. Pooling of these data resulted in 194 patients performing a total of 563 sports preoperatively (mean of 2.9 sports per patient: 56 % low impact, 31 % intermediate impact and 13 % high impact).
Postoperatively, these 194 patients performed 415 sports (mean of 2.1 sports per patient), of which 71 % were of low impact, 26 % of intermediate impact and 3 % of high impact.
3.5.2 Time to RTS
Four articles considered time to RTS after TKA. Argenson et al. [42] reported a mean time of 6 months and Hopper and Leach [52] a mean time of 4.1 months to return to mainly low-impact sports. Bock et al. [41] reported an overall mean time of 4.7 months to return to both low- and higher-impact sports, and Lefevre et al. [43] reported on time to return to one specific high-impact type of sport, namely judo, with a mean of 5.2 months in former black belt judokas. Pooling of the time to RTS data (Table 4), 388 patients needed an average time of 13 weeks after TKA to RTS, of which 95 % concerned low-impact sports. The average time for nine patients to return to intermediate-impact sports was 12 weeks and for nine patients it took an average of 26 weeks to return to high-impact sports. None of these included studies scored a low risk of bias.
Three studies contained data regarding overall time to RTS after UKA. Hopper and Leach [52] reported an overall mean time to RTS of 3.6 months to return to low-impact sports. Naal et al. [14] and Walker et al. [47] described an overall RTS after UKA within 3 months of 46 and 56 %, respectively, and within 6 months of 69 and 78 %, respectively.
The last two authors studied return to both low- and higher-impact sports. By pooling the data of 243 patients (Table 4), a mean time of 12 weeks to RTS after UKA was found, of which 91 % concerned low-impact sports. The average time for 222 patients to return to low-impact sports was 12 weeks, for 18 patients to return to intermediate-impact sports this was 16 weeks, and it took an average of 10 weeks for three patients to return to high-impact sports. None of these studies included for pooling data scored a low risk of bias.
3.6 Physical Activity
Regarding specific outcome measures of PA after TKA, UCLA scores were retrieved from three studies. Chang et al. [49] described a mean UCLA score of 4.5/10 (4.5 from a maximum possible score of 10) preoperatively and 4.8/10 postoperatively, and 9 % had a score higher than 6/10. Keeney et al. [55] described pre- and postoperative scores of patients younger than 55 years of 3.4/10 and 4.6 /10, respectively, and of patients between 65 and 75 years of 3.8/10 and 4.9/10. Bock et al. [41] described only a mean postoperative score of 5.9/10 in active patients. The Tegner-Lysholm score was described twice; it was 1.3/10 preoperatively and 3.5/10 postoperatively, with 24 % of scores higher than 5/10 in the study by Diduch et al. [54] and postoperatively a score of 3.9/10 was described in the study by Bock et al. [41]. The Grimby score was described only postoperatively in two studies; twice with scores of 2.8/6 [38, 40].
Regarding specific outcome measures concerning PA after UKA, two studies retrieved UCLA scores. Fisher et al. [51] scored a mean score of 4.2/10 before surgery and a score of 6.5/10 after surgery. Walker et al. [47] measured a mean score of 5.3/10 preoperatively and 6.7/10 postoperatively, with two-thirds of the scores >7. Walker et al. [47] also scored a Tegner of 2.9/10 preoperatively and 3.5/10 postoperatively. A Grimby score was measured in only one article, which showed a score of 3.9/6 postoperatively [38]. These PA scores show that after TKA, patients can regularly return to mild-to-moderate activities and UKA patients can return to moderate-to-high activities.
3.7 Rehabilitation and Confounding Factors
Eight of the 18 included studies described information about the rehabilitation protocol followed after KA, typically not much more than mentioning that ‘full weight bearing was allowed’ or ‘all patients underwent standardised rehabilitation’ (not otherwise specified). Naal et al. [14] and Lo Presti et al. [48] gave the best descriptions by saying that patients were advised not to RTS before a sufficient muscular recovery of both quadriceps and hamstrings was reached.
Whether confounders were taken into account concerning RTS after KA was scored separately in our data extraction form (Tables 1 and 2). Five of the 18 studies adjusted for confounding: Bradbury et al. (50) found negative influences of restricting co-morbidities and complications, and positive influences of motivation and preoperative sports level on RTS, the latter confirmed by Naal et al. [14].
Age was mentioned as a possible confounder in eight studies, but only in five of these studies was this confounder adequately adjusted for; in four studies age did not have any influence on RTS and only Naal et al. [14] reported a negative influence of older age on RTS after UKA. Chatterji et al. [40], Huch et al. [44], Keeney et al. [55] and Wylde et al. [53] found an influence of sex—men were more able to RTS than women—but Naal et al. [14] did not find any influence of sex. A negative influence of high body weight on RTS was described in four studies. Three studies [44, 47, 53] listed specific patient-reported reasons for restricted sports participation after KA. Discouragement from their surgeons, mainly to high-impact types of sports, was one reason, in addition to pain, functional problems, instability and loss of motivation or loss of confidence. Moreover, the importance of counselling advice from the surgeon was mentioned in six studies, in four of which it was explicitly stated that patients were advised not to resume high-impact sports after KA. Only in the article by Lefevre et al. [43], concerning the judokas, did the influence of this advice seem low because many patients returned to sports despite the surgeon’s recommendations to the contrary. This therefore suggests a positive influence of motivation on RTS.
4 Discussion
4.1 Main Results
Patients are able to return to both low- and higher-impact sports after both TKA and UKA, with overall percentages varying from 36 to 89 and from 74 to >100 %, respectively. Participation in sports seems more likely after UKA than TKA, with mean total numbers of sports postoperatively of 1.1–4.6 sports per patient after UKA and 0.2–1.0 after TKA. RTS after TKA for low-impact sports was 94, 64 % for intermediate-impact sports, and 43 % for high-impact sports. For UKA, these numbers are 93, >100 and 35 %, respectively. These findings were confirmed by the PA scores of patients, which are higher after UKA than after TKA, namely return to mild-to-moderate activities after TKA and return to moderate-to-high activities after UKA. Time to RTS took 13 weeks after TKA and 12 weeks after UKA, with 95 and 91 %, respectively, concerning low-impact sports.
4.2 Limitations and Strengths
A common limitation to all systematic reviews, including ours, is that some papers were overlooked. To overcome this problem, we performed an extensive search with sensitive search criteria and synonyms, and by making use of the expertise of a clinical librarian. Another limitation of this systematic review was that it consists of studies with broad heterogeneity in investigated study populations, defined baseline characteristics, chosen outcome measures and, of course, in research quality. Although systematic reviews with meta-analysis are generally seen as ‘a high quality of evidence’, we believe that given these limitations, our findings are at most of moderate quality. According to the outcome measures, many self-designed sports questionnaires were used. This kind of research is prone to so-called ‘recall bias’, as many rely on the patient’s ability to describe their sporting activities of several years previously. Moreover, different PA outcome measures were described, which were mostly not validated. The UCLA scale was most commonly used. Although the intrinsic disadvantage of the UCLA is that it is a categorical measure, it is a validated scale and until 2009 it seemed to be the most appropriate scale available for assessing PA levels in patients undergoing joint arthroplasty [56].
With respect to confounding factors, it is notable that in only seven of the 18 included studies was there a clear definition of the time of assessment of the preoperative sports level given. Considering the definitions used, such as ‘at time of surgery’, ‘at presymptomatic phase’ or ‘during life’, this has a significant effect on the reported RTS percentage, as Huch et al. [44] have also clearly shown. Other confounding factors that should have been adjusted for in determining percentages of RTS are sex, BMI, restricting comorbidities, complications, and psychosocial factors such as motivation and kinesiophobia of the patients. Conflicting results of a possible negative influence of age on postoperative activity have been mentioned previously, but the influence of age on RTS was also not clear from our included studies. Only a few included studies adequately adjusted for some or all of these confounding factors, resulting in an assessment of moderate or high risk of bias in 15 of 18 studies. In five of 13 included TKA studies and in four of eight included UKA studies, possible influences are stated concerning advice given by the surgeon that should also be taken into account. It is reasonable to assume that negative recommendations from their surgeons concerning high-impact types of sports will negatively influence a patient’s return to (especially) higher-impact sports, even if the patient had had the intention of doing so. Furthermore, the percentage of RTS is dependent on the preoperative sports level and (sports) rehabilitation.
A strength of the present study is that it provides a systematic overview of the literature concerning RTS and time to RTS after KA, including PA-specific outcome measures, while differentiating between TKA and UKA and pooling all extracted data. For this purpose, we selected only articles containing data of both pre- and postoperative sports participation, time to RTS and/or specific PA measurements. Most other reviews included general knee function scores like OKS (Oxford Knee Score) and the WOMAC (The Western Ontario and McMaster Universities Osteoarthritis Index) tool, which are generally accepted Patient Reported Outcome Measures (PROMs) nowadays. However, recently it has been stated that using these instruments has substantial disadvantages for the assessment of knee function with respect to activity and participation [57].
4.3 Comparison with the Medical Literature
In 1996, Vail and Mallon [36] stated that published information on sports participation after joint arthroplasty is retrospective, limited in scope and primarily anecdotal in origin.
Almost 20 years later, negative advice concerning high-impact activities after joint arthroplasty is still more speculative than evidence-based. Concerning these sports recommendations, the general consensus is that return to low-to-intermediate-impact sports within 3–6 months is possible without any problems, while high-impact sports should be discouraged and high-contact athletic activities should be avoided [17, 20, 58, 59]. In contrast, the article by Lefevre et al. [43] showed that 63 % of former black belt judokas resumed their high impact sport, and Mont et al. [60] conducted a promising study with high-level tennis players, all of whom were also able to resume their sport after TKA. Although long-term effects of high-impact sports on outcomes of TKA need to be determined, both studies proved that return to high-impact sport is actually possible. The discussion includes risks of instability, periprosthetic fractures, bearing surface wear, early aseptic loosening, and subsequently premature revisions after high-impact sports. If one considers this subject from a purely mechanical point of view, it seems apparent that the bearing surface wear rate is directly related to the cycles of use. However, accumulating data suggest that prosthetic wear is not simply a function of time in situ, but rather a function of use [61]. During activities such as hiking or jogging, between 40 and 60 degrees of knee flexion high joint loads of 5–10 times body weight can occur, something that not all knee designs are capable of absorbing, so high polyethylene inlay stress may occur [62]. While some studies indeed found higher radiological wear and potential implant failure in active patients, they did not show an increase in revision rates due to high activities at mid-term [63]. This means that the feared higher risk for survival reductions after TKA in active patients cannot be confirmed. However, length of follow-up is not yet adequate to be able to make definitive conclusions on this matter [64]. On the other hand, recent advances in implant technology, surgical techniques and prosthetic designs and materials, and survival rates of new and improved types of KAs are promising for patients with high demands [65]. Several systematic reviews have concluded that patients and orthopaedic surgeons do not necessarily worry about the same things after joint replacement surgery, that patients should be encouraged to become active after joint replacement, and that further research in this area should be stimulated [16, 66–70].
4.4 Clinical Implications
While younger and more active patients who undergo joint replacement may have higher expectations regarding activity, the literature suggests that nowadays they actually do not participate in functional levels of sports so often after knee replacement [20]. For example, Kersten et al. described that almost half of TKA patients did not meet health-enhancing PA guidelines and they were less active as a normative group [71]. After performing our review, the question arises: Is it due to a lack of will on the part of the patients that they are not always active after TKA? Or are they also highly influenced by negative advice from their orthopaedic surgeons regarding return to sports, as well as other possible restricting factors? Due to the fact that fulfilment of patient expectations after KA is considered to be a predictive criterion of satisfaction, the value of exploring a patient’s expectations regarding activities after knee replacement has been proven [72].
Historically, participating in sports after joint replacement has been discouraged. Although evidence on this subject is still sparse and of low quality, we can learn from this review that these negative recommendations are still not evidence-based and that actually it is possible to play many different sports after knee replacement surgery. Since postoperative outcomes and return to preoperative sports activity levels are influenced by many factors, individual characteristics, preoperative lifestyle, sport levels, motivation and patient preferences should be taken into account when one considers recommendations for athletic activity after joint replacement [73]. To optimise results, patients who demand higher levels of activity should be carefully selected. Since it seems that more patients can RTS and also to higher-impact types of sports after UKA in comparison with TKA, the choice of type of implant should also be considered. For individuals with limited anteromedial or only lateral compartment concerning types of OA, ‘as limited prosthetic constraint as possible’ and ‘as much retention of a “normal knee feeling” as possible’ are desirable.
Papalia et al. [70] recently found comparable RTS activity rates in patients undergoing TKA and UKA, but they based their conclusion on only one article. Regarding the results of our extensive systematic review, we, like Boyd et al. [74], tend to recommend a UKA over a TKA when indicated for a patient who wishes to remain highly active in a sport.
4.5 Recommendations
Based on this review concerning RTS after KA, we strongly recommend using the same language concerning generalising a clear definition of preoperative sports level in future studies. It seems most rational to define the (real and only) preoperative sports level as the ‘presymptomatic phase’ and not the moment ‘at time of surgery’. In other words, preoperative sports level should be based on the phase when the patient was not yet restricted in participating in his or her preferred sports because of osteoarthritic knee complaints.
There is still no real reliable and valid method to analyse PA levels, although the level of activity seems an important prognostic factor, as well as a valuable outcome measure in the assessment of orthopaedic disorders [75]. PROMs have gained importance in both clinical practice and medical research and not only to patients and clinicians, but also to regulators, policy makers and health insurance authorities. But skewing and ceiling effects of currently used PROMs have been described, so using these would not be sufficient for reporting PA outcomes after KA [76]. So-called performance-based outcome measures (PBMs) are defined as assessor-observed measures of tasks classified as ‘activities’ using the International Classification of Functioning, Disability and Health (ICF) model of the World Health Organisation (WHO). PBMs are strongly related to patient self-efficacy in actual performance of function, and have been suggested as possible complementary objective measurement tools next to existing PROMs [77]. In predicting return to work in musculoskeletal diseases, PBMs were shown to strengthen the prognostic value of self-reporting modestly, from 9 to 16 % [78, 79]. The measurement of physical function is complex since it contains multi-dimensional constructs. After performing a systematic review, Dobson et al. [80] recommend further good quality research in investigating the measurement properties of PBMs in people with hip and/or knee OA. Following this conclusion, we would like to recommend investigating the possible added value of PBMs to currently used PROMs in predicting RTS after KA.
A lack of evidence is also apparent with regard to the rehabilitation of highly functioning individuals and those who wish to RTS after knee replacement, but there are some promising results that support a more aggressive rehabilitative approach [81]. Remarkably, hardly any information concerning rehabilitation could be extracted from the studies included in our review, while this seems to be a significant issue. We agree that muscular rehabilitation is important and Healy et al. [67] stated that stretching and strengthening programmes could enhance athletic performance after knee replacement, which could actually prevent injuries and protect joint reconstructions. We recommend performing more research on the (possibly protective) role of a more extensive rehabilitation after KA.
In the absence of consensus from the literature with respect to long-term survival rates especially after performing high-impact sports, there is a need for good quality prospective trials. From our review, it can be concluded that for some patients, some types of high-impact sports are possible after KA.
In the meantime, the ‘intelligent participation’ recommendations of Kuster et al. [37] should be considered. They do not only look at the impact of the sport on the joints, but also take into account prior experiences and the way a patient will perform his or her sport. If activities such as skiing, hiking or tennis were not to be performed as a regular endurance activity but on a recreational basis only, they would be less harmful. Moreover, when, for example, shortcuts and steep descents are avoided during hiking, walking slowly downhill and using ski poles can reduce knee joint loads by 20 %. It would also be acceptable for skilled skiers to ski on flatter slopes, avoiding hard snow conditions and moguls, for 1–2 weeks per year. However, it would seem unwise to start such technically demanding sports activities after knee replacement, due to higher joint loads in unskilled performers and because of the high risk of injuries such as periprosthetic fractures.
5 Conclusion
Our systematic review showed that return to sports and physical activity is possible after both TKA and UKA, with percentages varying from 36 % to more than 100 %. Participation in sports seems more likely—including to higher-impact types—after UKA than after TKA, although after both surgeries patients tend to return to lower-impact types of sports. Time to RTS took 13 weeks after TKA and 12 weeks after UKA, respectively, with low-impact sports making up more than 90 % of cases. However, overall study quality of the included studies was limited due to confounding factors being insufficiently taken into account in most studies.
References
Ethgen O, Bruyère O, Richy F, et al. Health-related quality of life in total hip and total knee arthroplasty. J Bone Joint Surg Am. 2004;86-A(5):963–74.
Maxwell JL, Keysor JJ, Niu J, et al. Participation following knee replacement: the MOST cohort study. Phys Ther. 2013. doi:10.2522/ptj.20130109.
Otten R, van Roermund PM, Picavet HSJ. Trends in the number of knee and hip arthroplasties: considerably more knee and hip prostheses due to osteoarthritis in 2030. Ned Tijdschr Geneeskd. 2010;154:A1534.
Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780–5.
Blair SN, Sallis RE, Hutber A, et al. Exercise therapy—the public health message. Scand J Med Sci Sport. 2012;22:24–8.
Kohl HW, Craig CL, Lambert EV, et al. The pandemic of physical inactivity: Global action for public health. Lancet. 2012;380(9838):294–305. doi:10.1016/S0140-6736(12)60898-8.
Haskell WL, Lee IM, Pate RR, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116:1081–93.
Garber CE, Blissmer B, Deschenes MR, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–59.
Dunlop DD, Song J, Semanik PA, et al. Objective physical activity measurement in the osteoarthritis initiative: Are guidelines being met? Arthritis Rheum. 2011;63(11):3372–82.
Ries MD, Philbin EF, Groff GD, et al. Improvement in cardiovascular fitness after total knee arthroplasty. J Bone Joint Surg Am. 1996;78:1696–701.
Ravi B, Croxford R, Austin PC, et al. The relation between total joint arthroplasty and risk for serious cardiovascular events in patients with moderate-severe osteoarthritis: propensity score. BMJ. 2013. doi:10.1136/bmj.f6187.
Losina E, Walensky RP, Kessler CL, et al. Cost-effectiveness of total knee arthroplasty in the United States: patient risk and hospital volume. Arch Intern Med. 2009;169(12):1113–22.
Bedair H, Cha TD, Hansen VJ. Economic benefit to society at large of total knee arthroplasty in younger patients: a Markov analysis. J Bone Joint Surg Am. 2014;96:119–26.
Naal FD, Fischer M, Preuss A, et al. Return to sports and recreational activity after unicompartmental knee arthroplasty. Am J Sports Med. 2007;35:1688–95.
Wylde V, Livesey C, Blom AW. Restriction in participation in leisure activities after joint replacement: an exploratory study. Age Ageing. 2012;41(January):246–9.
Seyler TM, Mont MA, Ragland PS, et al. Sports activity after total hip and knee arthroplasty. Sport Med. 2006;36(7):571–83.
McGrory BJ, Stuart MJ, Sim FH. Participation in sports after hip and knee arthroplasty: Review of literature and survey of surgeon preferences. Mayo Clin Proc. 1995;70(4):342–8.
Swanson EA, Schmalzried TP, Dorey FJ. Activity recommendations after total hip and knee arthroplasty: a survey of the American Association for Hip and Knee Surgeons. J Arthroplasty. 2009;24(6):120–6.
Cirincione RJ. Sports after total joint replacement. Md Med J. 1996;45(8):644–7.
Healy WL, Sharma S, Schwartz B, et al. Athletic activity after total joint arthroplasty. J Bone Joint Surg Am. 2008;90:2245–52.
Healy WL, Iorio RLM. Total knee arthroplasty. Clin Orthop Relat Res. 2000;380:65–71.
Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Phys Ther. 2009;89:873–80.
Zahiri CA, Schmalzried TP, Szuszczewicz ES, et al. Assessing activity in joint replacement patients. J Arthroplasty. 1998;13(8):890–5.
Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res. 1985;198:43–9.
Grimby G. Physical activity and muscle training in the elderly. Acta Med Scand Suppl. 1986;711:233–7.
Hayden JA, van der Windt DA, Cartwright JL, et al. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;144:427–37.
Lee D, Kim D, Scott R, et al. Intraoperative flexion against gravity as an indication of ultimate range of motion in individual cases after total knee arthroplasty. J Arthroplasty. 1998;13(5):500–3.
Brandes M, Ringling M, Winter C, et al. Changes in physical activity and health-related quality of life during the first year after total knee arthroplasty. Arthritis Care Res. 2011;63(3):328–34.
Kennedy DM, Stratford PW, Riddle DL, et al. Assessing recovery and establishing prognosis following total knee arthroplasty. Phys Ther. 2013;88(1):22–32.
Kristman V, Manno M, Côté P. Loss to follow-up in cohort studies: how much is too much? Eur J Epidemiol. 2004;19(8):751–60.
Hoozemans MJM, Knelange EB, Frings-Dresen MHW, et al. Are pushing and pulling work-related risk factors for upper extremity symptoms? A systematic review of observational studies. Occup Environ Med. 2014;71:788–95.
Williams DH, Greidanus NV, Masri BA, et al. Predictors of participation in sports after hip and knee arthroplasty. Clin Orthop Relat Res. 2012;470:555–61.
Lützner C, Kirschner S, Lützner J. Patient activity after TKA depends on patient-specific parameters. Clin Orthop Relat Res. 2014;472:3933–40.
Lee J, Song J, Hootman JM, et al. Obesity and other modifiable factors for physical inactivity measured by accelerometer in adults with knee osteoarthritis. Arthritis Care Res. 2013;65(1):53–61.
Kerkhoffs GMMJ, Servien E, Dunn W, et al. The influence of obesity on the complication rate and outcome of total knee arthroplasty: a meta-analysis and systematic literature review. J Bone Joint Surg Am. 2012;94:1839–44.
Vail TP, Mallon WJ. Athletic activities after joint arthroplasty. Sports Med Arthrosc. 1996;4:298–305.
Kuster MS, Spalinger E, Blanksby BA, et al. Endurance sports after total knee replacement: a biomechanical investigation. Med Sci Sports Exerc. 2000;32(12):721–4.
Jahromi I, Walton NP, Dobson PJ, et al. Patient-perceived outcome measures following unicompartmental knee arthroplasty with mini-incision. Int Orthop. 2004;28:1–4.
Walton NP, Jahromi I, Lewis PL, et al. Patient-perceived outcome and return to sport and work: TKA versus mini-incision unicompartmental knee arthroplasty. J Knee Surg. 2006;19(2):112–6.
Chatterji U, Ashworth MJ, Lewis PL. Effect of total knee arthroplasty on recreational and sporting activity. Knee. 2005;75:405–8.
Bock P, Schatz K, Wurnig C. Körperliche aktivität nach knietotalprothesenimplantation. Z Orthop Ihre Grenzgeb. 2003;141:272–6.
Argenson JN, Parratte S, Ashour A, et al. Patient-reported outcome correlates with knee function after a single-design mobile-bearing TKA. Clin Orthop Relat Res. 2008;466:2669–76.
Lefevre N, Rousseau D, Bohu Y, et al. Return to judo after joint replacement. Knee Surg Sports Traumatol Arthrosc. 2013;21:2889–94.
Huch K, Müller KAC, Stürmer T, et al. Sports activities 5 years after total knee or hip arthroplasty: the Ulm Osteoarthritis Study. Ann Rheum Dis. 2005;64:1715–20.
Münnich U, König DP, Popken F, et al. Entwicklung der körperlichen und sportlichen Aktivität von Patienten vor und nach Implantation einer totalen Knieendoprothese. Versicherungsmedizin. 2003;55(2):82–6.
Pietschmann MF, Wohlleb L, Weber P, et al. Sports activities after medial unicompartmental knee arthroplasty Oxford III - What can we expect? Int Orthop. 2013;37:31–7.
Walker T, Gotterbarm T, Bruckner T, et al. Return to sports, recreational activity and patient-reported outcomes after lateral unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2015;23(11):3281–7.
Lo Presti M, Iacono F, Bruni D, et al. Return to sports activity after unicompartmental knee arthroplasty. J Orthop Traumatol. 2011;12(Suppl 1):S139.
Chang M, Kim S, Kang Y, et al. Activity levels and participation in physical activities by Korean patients following total knee arthroplasty. BMC Musculoskelet Disord. 2014;15(1). doi:10.1186/1471-2474-15-240.
Bradbury N, Borton D, Spoo G, et al. Participation in sports after total knee replacement. Am J Sport Med. 1998;26(4):530–5.
Fisher N, Agarwal M, Reuben SF, et al. Sporting and physical activity following Oxford medial unicompartmental knee arthroplasty. Knee. 2006;13:296–300.
Hopper GP, Leach WJ. Participation in sporting activities following knee replacement: total versus unicompartmental. Knee Surg Sports Traumatol Arthrosc. 2008;16:973–9.
Wylde V, Blom A, Dieppe P, et al. Return to sport after joint replacement. J Bone Joint Surg Br. 2008;90:920–3.
Diduch DR, Insall JN, Scott WN, et al. Total knee replacement in young, active patients. J Bone Joint Surg Am. 1997;79(4):575–82.
Keeney JA, Nunley RM, Wright RW, et al. Are younger patients undergoing TKAs appropriately characterized as active? Clin Orthop Relat Res. 2014;472:1210–6.
Naal FD, Impellizzeri FM, Leunig M. Which is the best activity rating scale for patients undergoing total joint arthroplasty? Clin Orthop Relat Res. 2009;467(4):958–65.
Alviar MJ, Olver J, Brand C, et al. Do patient-reported outcome measures used in assessing outcomes in rehabilitation after hip and knee arthroplasty capture issues relevant to patients? Results of a systematic review and ICF linking process. J Rehabil Med. 2011;43(5):374–81.
Jones DL. A public health perspective on physical activity after total hip and knee arthroplasty for osteoarthritis. Phys Sport Med. 2011;39(4):70–9.
Hartford JM. Sports after arthroplasty of the knee. Sports Med Arthrosc. 2003;11(2):149–54.
Mont MA, Rajadhyaksha AD, Marxen JL, et al. Tennis after total knee arthroplasty. Am J Sports Med. 2002;30(2):163–6.
Schmalzried TP, Shepherd EF, Dorey FJ, et al. The John Charnley award. Wear is a function of use, not time. Clin Orthop Relat Res. 2000;381(381):36–46.
Kuster MS. Exercise recommendations after total joint replacement. A review of the current literature and proposal of scientifically based guidelines. Sport Med. 2002;32(7):433–45.
Jones DL, Cauley JA, Kriska AM, et al. Physical activity and risk of revision total knee arthroplasty in individuals with knee osteoarthritis: a matched case–control study. J Rheumatol. 2004;31(7):1384–90.
Jassim SS, Douglas SL, Haddad FS. Athletic activity after lower limb arthroplasty: a systematic review of current evidence. Bone Joint J. 2014;96-B(7):923–7.
Iorio R, Healy WL, Applegate T. Validity of preoperative demand matching as an indicator of activity after TKA. Clin Orthop Relat Res. 2006;452(452):44–8.
Lahav A. Returning to sports after total joint replacement and tibial osteotomies: is it possible? Conn Med. 2012;76(8):483485.
Healy WL, Iorio R, Lemos MJ. Athletic activity after joint replacement. Am J Sports Med. 2001;29(3):377–88.
Golant A, Christoforou DC, Slover JD, et al. Athletic participation after hip and knee arthroplasty. Bull NYU Hosp Jt Dis. 2010;68(2):76–83.
Nicholls MA, Selby JB, Hartford JM. Athletic activity after total joint replacement. Orthopedics. 2002;25(11):1283–7.
Papalia R, Del Buono A, Zampogna B, et al. Sport activity following joint arthroplasty: a systematic review. Br Med Bull. 2012;101(1):81–103.
Kersten RFMR, Stevens M, van Raay JJAM, et al. Habitual physical activity after total knee replacement. Phys Ther. 2012;92(9):1109–16.
Scott CEH, Bugler KE, Clement ND, et al. Patient expectations of arthroplasty of the hip and knee. J Bone Joint Surg Br. 2012;94(7):974–81.
Vogel LA, Carotenuto G, Basti JJ, et al. Physical activity after total joint arthroplasty. Sport Health. 2011;3(5):441–50.
Boyd JL, Kurtenbach CA, Sikka RS. Patient-specific instrumentation and return to activities after unicondylar knee arthroplasty. Clin Sports Med. 2014;33(1):133–48.
Brosphy RH, Lin K, Smith MV. The role of activity level in orthopaedics: an important prognostic and outcome variable. J Am Acad Orthop Surg. 2014;22(7):430–6.
Williams DP, Price AJ, Beard DJ, et al. The effects of age on patient-reported outcome measures in total knee replacements. Bone Joint J. 2013;95-B(1):38–44.
Hossain FS, Konan S, Patel S, et al. The assessment of outcome after total knee arthroplasty: are we there yet? Bone Joint J. 2015;97-B(1):3–9.
Kuijer PPFM, Gouttebarge V, Brouwer S, et al. Are performance-based measures predictive of work participation in patients with musculoskeletal disorders? A systematic review. Int Arch Occup Environ Health. 2012;85(2):109–23.
Kuijer PPFM, Gouttebarge V, Wind H, et al. Prognostic value of self-reported work ability and performance-based lifting tests for sustainable return to work among construction workers. Scand J Work Environ Heal. 2012;38(6):600–3.
Dobson F, Hinman RS, Hall M, et al. Measurement properties of performance-based measures to assess physical function in hip and knee osteoarthritis: a systematic review. Osteoarthritis Cartilage. 2012;20(12):1548–62.
Lorenz DS, Salsbery MA. Return to high-level activity following knee replacement. Top Geriatr Rehabil. 2013;29(1):46–54.
Acknowledgements
The authors would like to thank Ms. Faridi S. van Etten-Jamaludin, librarian of the AMC, and Ms. Milou van Son, medical student, for their assistance in performing a systematic search of the literature and the inclusion of studies.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This review was part of a funded research project, supported by a grant from the NutsOhra Foundation.
Conflicts of interest
Suzanne Witjes, Vincent Gouttebarge, Paul Kuijer, Rutger van Geenen, Rudolf Poolman and Gino Kerkhoffs declare that they have no conflicts of interest relevant to the content of this review, and no further financial relationship with the organisation that funded the research. The researchers prepared and submitted this manuscript independently from the study sponsors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
40279_2015_421_MOESM3_ESM.docx
Supplementary material 3: Appendix S3. Levels of impact on knee joint of different types of sports participationa (DOCX 62 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Witjes, S., Gouttebarge, V., Kuijer, P.P.F.M. et al. Return to Sports and Physical Activity After Total and Unicondylar Knee Arthroplasty: A Systematic Review and Meta-Analysis. Sports Med 46, 269–292 (2016). https://doi.org/10.1007/s40279-015-0421-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-015-0421-9