Article Text

Abstract
Endurance athletes have a high prevalence of atrial fibrillation (AF), probably caused by exercise-induced cardiac remodelling. Athletes diagnosed with AF are often advised to reduce the intensity and amount of training but the efficacy of this intervention has not been investigated in endurance athletes with AF. Effects of detraining in endurance athletes with atrial fibrillation is a two-arm international multicentre randomised (1:1) controlled trial on the effects of a period of training adaption on AF burden in endurance athletes with paroxysmal AF.
One-hundred-and-twenty endurance athletes diagnosed with paroxysmal AF are randomised to a 16-week period of intervention (training adaption) or a control group. We define training adaption as training with a heart rate (HR) not exceeding 75% of the individual maximum HR (HRmax), and total duration of weekly training not exceeding 80% of the self-reported average before the study. The control group is instructed to uphold training intensity including sessions with HR ≥85% of HRmax. AF burden is monitored with insertable cardiac monitors, and training intensity with HR chest-straps and connected sports watches. The primary endpoint, AF burden, will be calculated as the cumulative duration of all AF episodes lasting ≥30sec divided by total duration of monitoring. Secondary endpoints include number of AF episodes, adherence to training adaption, exercise capacity, AF symptoms and health-related quality of life, echocardiographic signs of cardiac remodelling and risk of cardiac arrhythmias related to upholding training intensity.
Trial registration number NCT04991337.
Study protocol version 4.7 (Date 9 March 2023).
- Exercise
- Sports medicine
- Athlete
- Endurance
- Cardiology
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Endurance athletes have an elevated risk of atrial fibrillation associated with exercise-induced cardiac remodelling.
Despite a lack of evidence to suggest exercise recommendations, endurance athletes suffering atrial fibrillation are often advised to reduce the intensity and amount of exercise.
WHAT THIS STUDY ADDS
This is the first randomised controlled trial that addresses the feasibility and effects of a period of training adaption in endurance athletes with paroxysmal atrial fibrillation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study has the potential to provide scientific knowledge that could guide development of specific exercise recommendations for endurance athletes with atrial fibrillation.
Introduction
Endurance exercise and atrial fibrillation
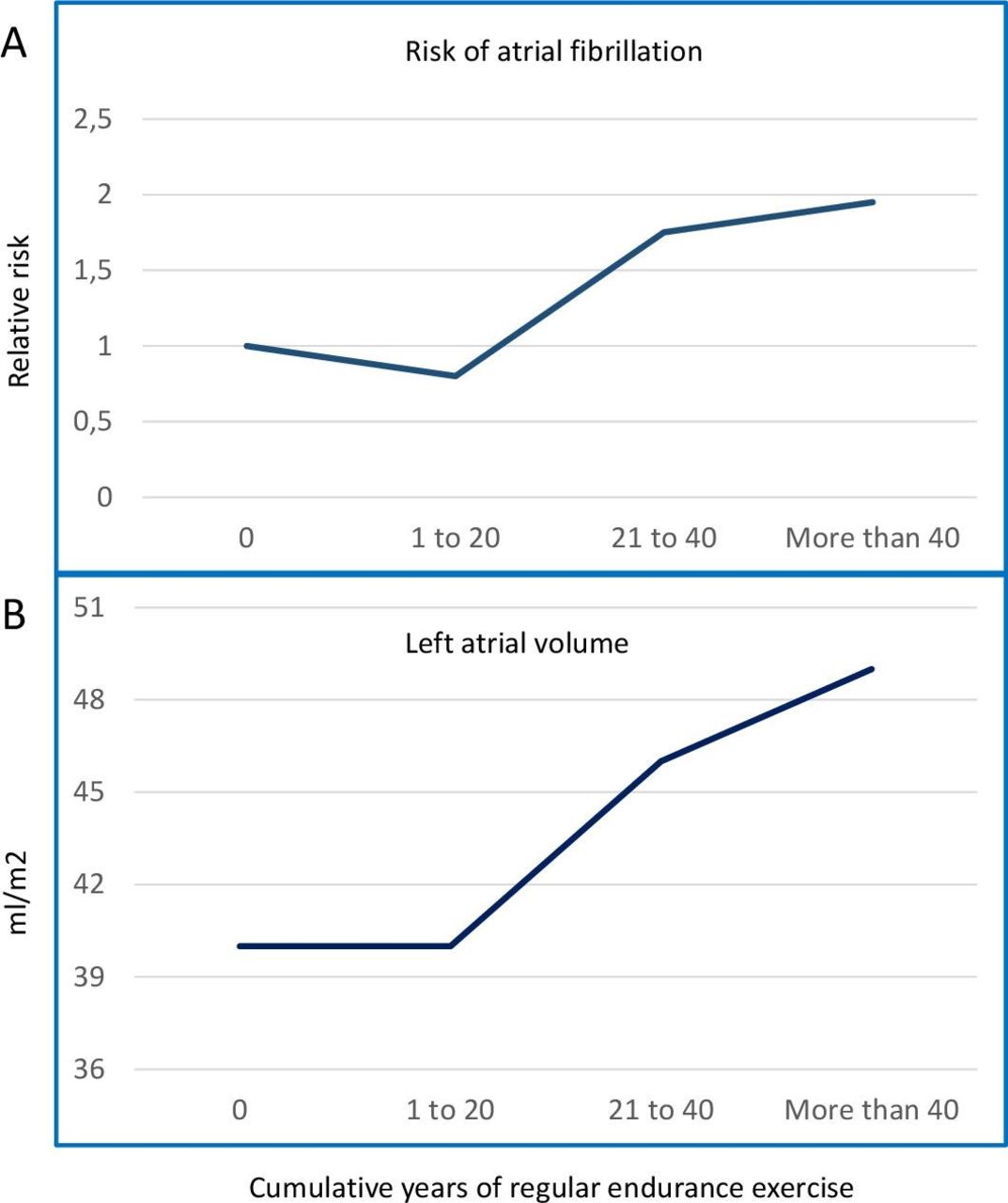
Compared with physical inactivity, moderate levels of physical activity reduce the risk of atrial fibrillation (AF).1 2 Studies of inactive AF patients have demonstrated that endurance exercise may reduce AF burden even during a short intervention period.3 Paradoxically, studies have demonstrated a high prevalence of AF among otherwise healthy male endurance athletes, suggesting vigorous endurance sport practice is a risk factor for the development of AF.4 5 A dose-response association between AF and cumulative exposure to endurance exercise was demonstrated among more than 3500 Norwegian men aged ≥53 years, where the risk of AF increased with 16% per decade of regular exercise.6 In a subset of these study participants, a similar relationship was demonstrated between prolonged exposure to endurance exercise and cardiac remodelling, such as atrial enlargement7 8 (figure 1). The high prevalence of AF in endurance athletes has led to the hypothesis that exercise-induced cardiac remodelling is a proarrhythmic condition.9 10 During exercise, circulatory flow is increased up to eight times as compared with rest.11 In response to this haemodynamic stress, long-term endurance exercise is accompanied by structural, functional and electrical cardiac remodelling referred to as the ‘athlete’s heart’.12 Atrial enlargement is associated with pathological cardiac remodelling and an increased risk of AF in the general population.7 13 The extent of atrial remodelling associated with long-term endurance training can be profound.7 8 There is a lack of long-term data on cardiac effects of endurance exercise, and the pathophysiological mechanisms behind exercise-associated AF are only partly understood.
Training adaption
Although AF is not a life-threatening condition, high ventricular rates during exercise with AF may cause symptoms, haemodynamic compromise and safety concerns that contribute to a conservative approach among many physicians facing these athletes. The impact of altering endurance exercise load on AF burden in athletes suffering AF remains unexplored. Despite a lack of evidence, endurance athletes with AF have traditionally been advised to reduce both the amount and intensity of exercise, often referred to as detraining.14 This approach assumes that the exercise stimulus plays a causative role in the development of AF, and that continuation of the same stimulus could lead to further cardiac remodelling and ultimately disease progression. In an animal model, rats experienced increased AF inducibility after 16 weeks of endurance training on treadmill, with AF inducibility returning to baseline levels following 4 weeks of detraining.15 While exercise-induced ventricular hypertrophy and dilatation (‘athlete’s heart’) seems to be partially reversible by detraining,16–18 data regarding the effects of training adaption on atrial remodelling and exercise-induced AF in humans do not exist.
Present guidelines
While an expert position statement suggests that sports activities can be resumed after diagnostic workup if the episodes of AF are rare,19 The European Society of Cardiology guidelines on Sports Cardiology and Exercise, and guidelines for the management of AF suggest to counsel athletes that prolonged sport participation may promote AF.20 Thus, endurance athletes with AF and their physicians are left without specific recommendations regarding the preferred exercise intensity to improve symptoms and reduce the risk of AF recurrence. Studies have shown that many athletes with AF prefer to maintain exercise intensity and competitive activities irrespective of their diagnosis.21
Both safety questions and the effects of upholding high exercise volumes on the risk of AF recurrence were highlighted among the major knowledge gaps in the recently published ESC sports cardiology guidelines.19 Furthermore, neither adherence to training adaption, symptoms nor quality of life (QoL) have been studied in athletes receiving exercise restrictions. Consequently, we designed a randomised controlled trial (RCT) to investigate the effects of training adaption in endurance athletes with paroxysmal AF.
Methods and analysis
Study design
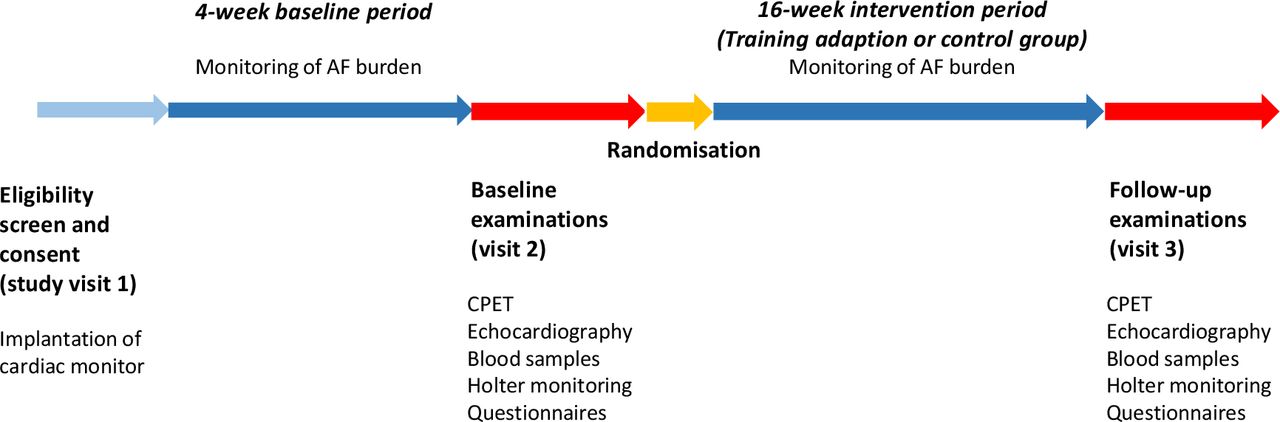
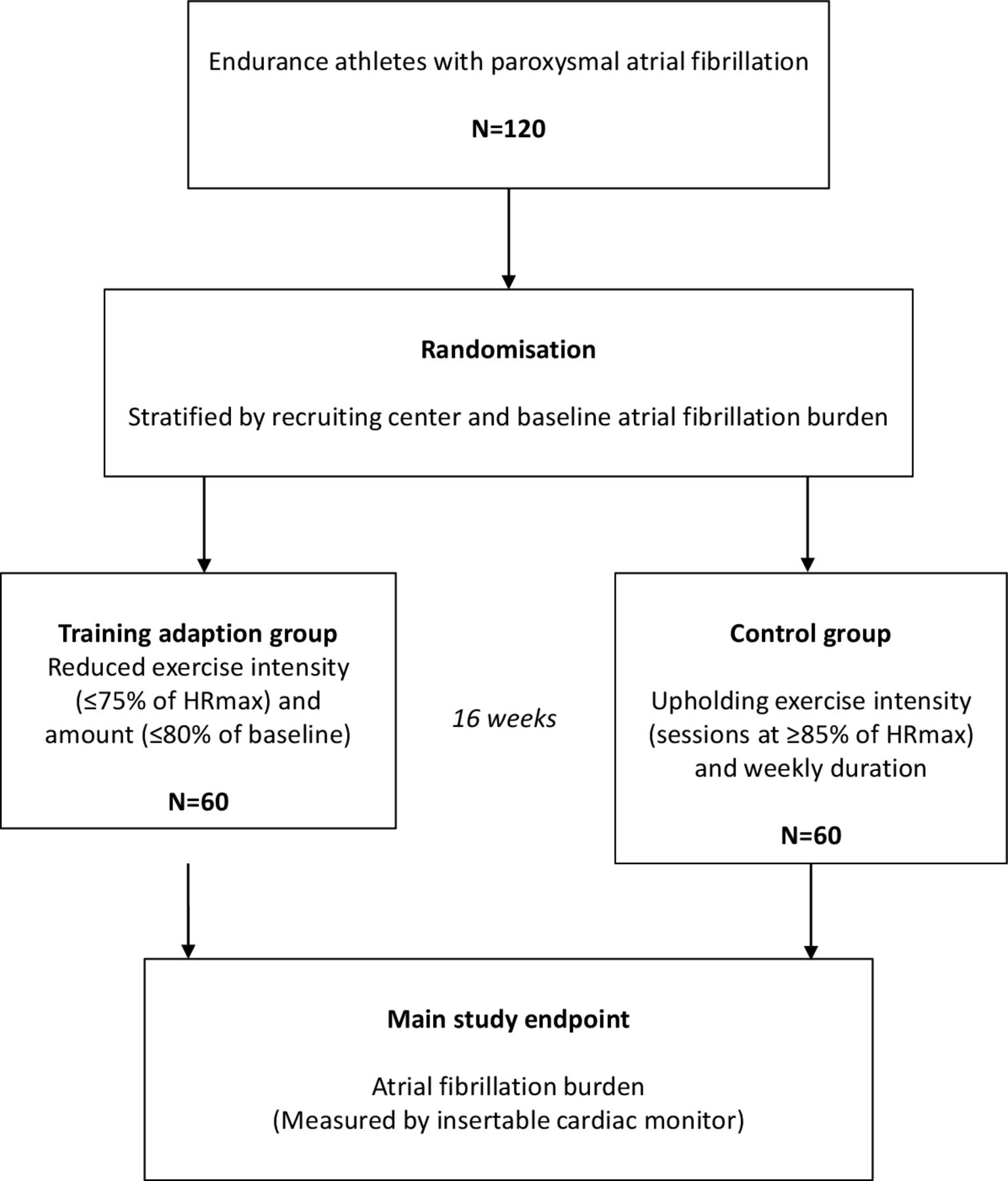
Effects of Detraining in Endurance Athletes with Atrial Fibrillation (NEXAF Detraining) is an international multicentre, two-armed, RCT with blinded endpoint evaluation (ClinicalTrials.gov Registry Identifier NCT04991337). The study protocol (V.4.7, 9 March 2023) is in accordance with the SPIRIT 2013 statement regarding standard protocol items for clinical trials (online supplemental table 1),22 and meets the requirements of the WHO Trial Registration Data Set (online supplemental table 2). Study participants are included at seven participating centres across three countries: Bærum Hospital, Bærum (Norway), St. Olavs Hospital, Trondheim (Norway), The Baker Heart and Diabetes Institute, Melbourne (Australia), The University Hospital of Leuven (Belgium), Antwerp University Hospital (Belgium), AZ Jan Palfijn Gent (Belgium) and Jessa Hospital Hasselt (Belgium). A total of 120 study participants will be randomised to an intervention arm with training adaption or a control arm upholding high intensity exercise for a period of 16 weeks (online supplemental graphical abstract, figure 2). All study participants receive an insertable cardiac monitor (ICM) during the first study visit for continuous monitoring of AF burden. Subsequently, participants will practice their regular exercise for 4 weeks to allow quantification of baseline AF burden. During the second study visit (week 5) participants will undertake baseline examinations, including echocardiography, cardiopulmonary exercise testing (CPET), questionnaire, blood samples, 24-hour ambulatory ECG and randomisation. All examinations will be repeated during a follow-up study visit after 16 weeks (figure 3).
Supplemental material
Supplemental material
Supplemental material
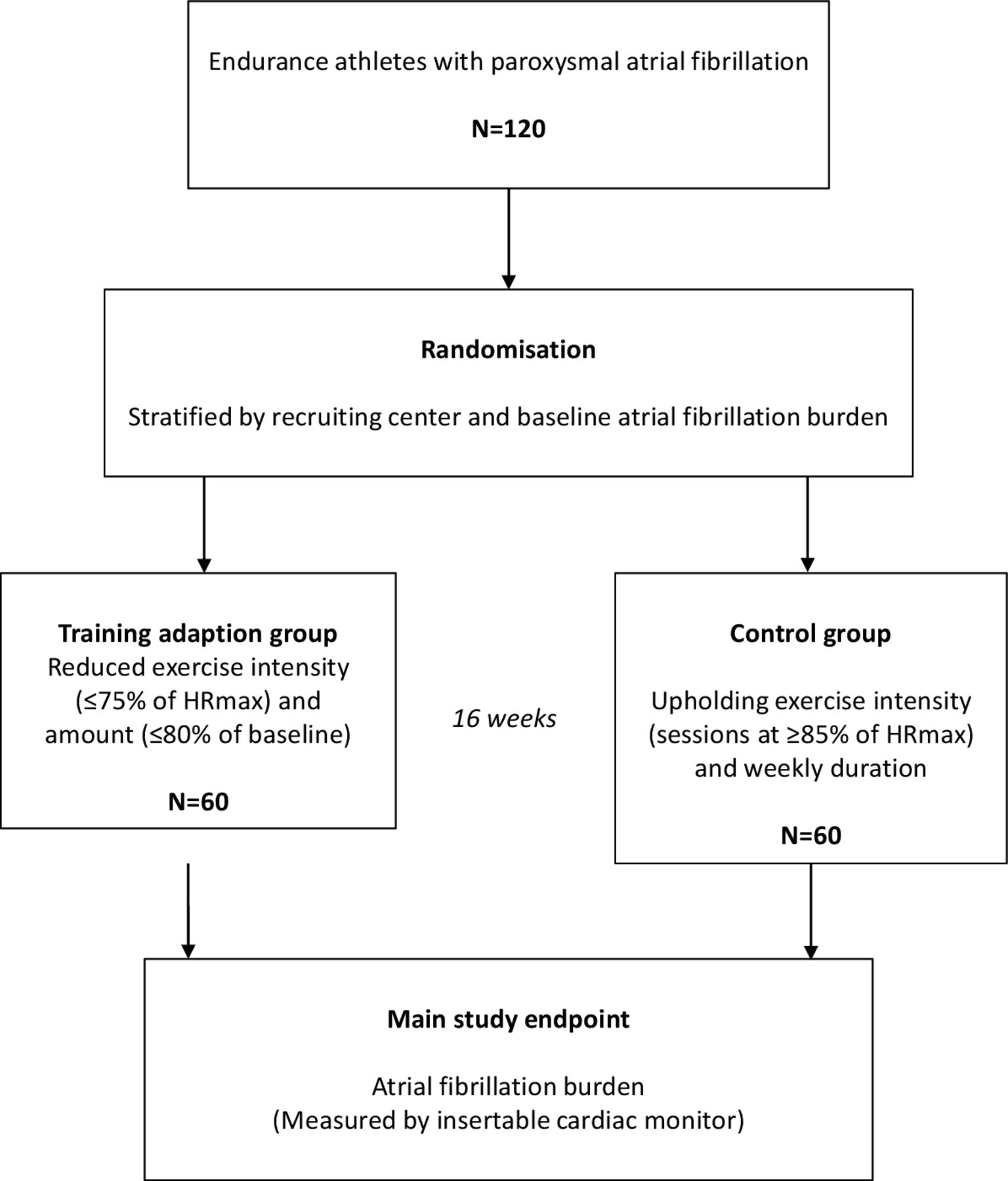
Study design. Overview of the design of the randomised controlled trial NEXAF Detraining. HRmax, maximum heart rate; NEXAF Detraining, Effects of Detraining in Endurance Athletes with Atrial Fibrillation.
{kind=link}
{kind=link}
{kind=link}
Study visit schedule and study procedures of the randomised controlled trial. AF, atrial fibrillation; CPET, cardiopulmonary exercise testing; NEXAF Detraining, Effects of Detraining in Endurance Athletes with Atrial Fibrillation.
Objectives and hypothesis
The primary objective of the study is to clarify whether a period of training adaption reduces AF burden in endurance athletes with paroxysmal AF. Secondary objectives are to study the adherence to training adaption, effects of training adaption on AF symptoms and health-related QoL, risk of cardiac arrhythmias related to upholding high-intensity training and to improve the understanding of underlying mechanisms for AF by studying structural and electrical cardiac remodelling. We hypothesise that a period of tailored training will reduce AF burden and improve QoL in endurance athletes with paroxysmal AF.
Endpoints
The primary endpoint is AF burden, as measured by continuous monitoring with ICMs and calculated as the cumulative duration of all AF episodes lasting ≥30 s divided by total duration of monitoring. All AF episodes will be adjudicated by a blinded endpoint committee consisting of two cardiologists, who will adjudicate AF episodes independently and reach consensus in the case of discrepancy. Table 1 shows an overview of study endpoints.
Primary and secondary endpoints of NEXAF Detraining
Study population and eligibility criteria
Eligibility criteria include female and male endurance athletes aged ≥18 years, diagnosed with paroxysmal AF. Participants in this study are athletes of elite and recreational levels, who are performing structured, repetitive exercise aiming to improve their physical fitness and are engaged in regular endurance sports such as running and rowing for at least 5 hours/week or cycling and cross-country skiing for at least 8 hours/week on average, or a combination of these sports or other comparable endurance sports characterised by medium or high intensity.20 As weekly hours of exercise are an arbitrary measure, cut-offs are pragmatic choices and indicative.
We include athletes reporting at least two episodes of AF, of which at least one that has occurred during the past 6 months. To minimise the impact of other factors that may have caused AF or may affect AF burden, athletes with arterial hypertension and other cardiovascular risk factors or conditions are excluded from participating in the study. People at high risk of adverse cardiovascular events, including athletes with cardiovascular risk factors, a strong family history of coronary artery disease or sudden death or symptoms during activity, are excluded after a preparticipating screening by questionnaire.20 23 24 Box 1 shows the eligibility criteria for the study. To be included, participants must fulfil all inclusion criteria and have no exclusion criteria.
Eligibility criteria for Effects of Detraining in Endurance Athletes with Atrial Fibrillation
Inclusion criteria
Signed informed consent.
Age ≥18 years.
Diagnosed with paroxysmal atrial fibrillation (verified by ECG).
Athletes reporting >5 (running, rowing) or >8 (cycling, cross-country skiing) weekly hours, respectively, of endurance sport practice,
At least two anamnestic (self-reported) episodes of atrial fibrillation, of which one during the last 6 months.
Use a smartphone and agree to connect their sports watch with a web-based platform for monitoring of exercise.
Exclusion criteria
Permanent atrial fibrillation.
Cardiac conditions (including valvular heart disease of moderate or greater severity, symptomatic ischaemic heart disease).
Suspicion of undiagnosed ischaemic heart disease.
Left ventricular ejection fraction <45%.
Arterial hypertension (>140/90 mm Hg).
Diabetes mellitus.
Hyperthyroidism.
Smoking during the last 5 years.
Alcohol intake >20 alcohol units/week.
Use of illegal or performance enhancing drugs.
Body mass index >30 kg/m2.
Injuries preventing physical exercise.
Pregnancy.
Participation in conflicting intervention research studies.
Planned atrial fibrillation ablation within the next 6 months.
The individual refuses to have an insertable cardiac monitor, blood samples taken or be part of the detraining group.
Informed consent
Eligible participants receive written and oral information about the study and must sign an informed consent form approved by the ethical committee for medical research of the respective study centres.
Atrial fibrillation monitoring
We insert a wireless ICM (Confirm Rx, Abbott, Sylmar, California, USA) subcutaneously near the left parasternal area over the third or fourth intercostal space at 45° to the sternum in men and 10°–15° in women. At the end of the procedure, we confirm reliable signal quality and R-wave sensing using an external programmer. ICMs are programmed to detect and record arrhythmic events defined as AF episodes lasting ≥30 s, pauses ≥3 s, bradycardia with heart rate (HR) ≤30 beats per minute (bpm) and tachycardia lasting ≥12 beats with a HR ≥180 bpm. In participants with a measured maximum HR (HRmax) >170 bpm, we programme the ICM to detect tachycardia when HR exceeds the recorded HRmax by ≥10 bpm. The device connects via Bluetooth and a smartphone application, and the data are uploaded to a secure server every 24 hours. Summarised reports of data from the ICM are generated every fourth week during the entire study period, reporting total time in AF, number and duration of AF episodes, pauses, bradycardia and tachycardia episodes. The ICM will be removed after the study or kept for up to the battery life expectancy of 2 years, on the participants’ request.
Intervention
The study participants are randomised 1:1, stratified by recruiting centre and AF burden during the 4-week baseline observation (<4% or ≥4%), to training adaption (intervention) or a control group. The participants are assigned to each group using a predefined permuted block randomisation to avoid imbalanced data. The allocation sequence was prepared by a statistician not directly involved in the study and is unavailable to the study personal and is implemented at each participating centre during the second study visit by use of sealed envelopes.
The training adaption is individually tailored, based on HRmax and the self-reported average weekly hours of training during the past 6 months. The intervention group is instructed to avoid high-intensity exercise corresponding to a HR >75% of HRmax, and a total duration of exercise (hours/week) corresponding to <80% of the self-reported average weekly amount of exercise (hours/week) for a period of 16 weeks. The control group is instructed to perform at least 3 weekly sessions of high-intensity training, corresponding to a HR of ≥85% HRmax, and otherwise continue endurance exercise as usual, for a period of 16 weeks. For practical reasons, we have chosen to define exercise intensity as a percentage of the individual’s HRmax. We use the highest reliable HRmax value measured in sinus rhythm via ECG monitoring during the CPET or during exercise with a HR chest-strap and a connected sports watch. To avoid caveats related to the use of HRmax in participants using beta-blockers, we use the HRmax derived from CPET performed while the participant has taken their medication.
Based on a pragmatic approach, we have defined training adaption as reducing exercise intensity to ≤75% of HRmax, corresponding to the threshold for moderate intensity suggested in exercise guidelines for the general population.25 Furthermore, to avoid compensation of the reduced intensity by increased training volume, participants are instructed to reduce their weekly hours of endurance exercise by 20%. Based on previous studies of detraining in animal models and athletes, we considered a period of reduced training intensity of 16 weeks to be sufficient to affect AF burden and at the same time acceptable to the athletes.15–17
Exercise monitoring
Participants are instructed to wear a HR monitor strapped around the chest and a sports watch when exercising throughout the entire study period. The HR chest-strap and watch connect using Bluetooth technology. We make use of the study participants’ personal sports watches. Alternatively, study participants receive a HR chest-strap (Garmin HRM-PRO) and sports watch (Garmin Forerunner 745) for the study period. The sports watch connects with Bluetooth technology to a web-based platform (Fitrockr, Digital Rebels, Berlin, Germany or TrainingPeaks, Louisville, Colorado, USA). We register the total amount of exercise and time during exercise sessions at different HR zones, <61%, 61%–70%, 71%–75%, 76%–80%, 81%–84%, 85%–90% and >90% of HRmax, respectively. This exercise monitoring allows assessment of adherence to the study intervention.
Blood samples
Fasting blood samples for analyses of biomarkers for cardiovascular risk factors are collected at rest at baseline and follow-up. Serum and plasma are stored at −80°C for subsequent batch analyses of biomarkers relevant for AF. In addition, we collect blood samples before and at maximal effort during CPET to assess the acute response to exercise (High-sensitive Troponins, NT-proBNP).
Questionnaires
At baseline and follow-up, the participants are asked to fill out the Atrial Fibrillation Effect on QualiTy-of-life questionnaire (AFEQT), assessing severity and frequency of AF symptoms, daily activity, treatment concerns and satisfaction.26 We score the AF symptom severity from none (1) to disabling (4) using the Modified European Heart Rhythm Association Symptom Scale.27 At baseline, we also obtain patients characteristics, self-reported history of endurance exercise and frequency, duration and triggers of AF episodes. At follow-up, participants are requested to fill out a questionnaire concerning AF treatment during the study and their experience with the ICM and the study intervention.
Transthoracic echocardiography
Transthoracic echocardiography is performed in sinus rhythm with a study-specific protocol in line with current recommendations.28 29 For assessment of cardiac structure and function, we perform resting two-dimensional (2D) and three-dimensional (3D) transthoracic echocardiography using the Vivid E95 ultrasound system (GE Healthcare, Horten, Norway). Images are obtained using a 1.5-4MHz matrix-array transducer (GE 4Vc-D Matrix 4D cardiac probe, GE healthcare, Horten, Norway). 2D-greyscale, colour Doppler and tissue Doppler imaging data will be obtained, in addition to 3D of the left atrium. A physician blinded to the participant’s clinical and study information will analyse the acquired images offline (Echo Pac, V.204, GE Vingmed Ultrasound, Horten, Norway). We assess systolic and diastolic volumes of both atria and the left ventricle, and right ventricular size. Comprehensive two-dimensional speckle tracking analyses will be performed of all four chambers, combined with established Doppler parameters to obtain information about systolic and diastolic function.
Cardiopulmonary exercise testing (CPET)
We perform CPET using a study-specific protocol. A standard 12-lead ECG is recorded at rest and throughout the test.23 Peak oxygen consumption (VO2peak) is measured in sinus rhythm using one of three predefined continuous ramp bicycle protocols, based on the patient’s estimated physical capacity. All protocols start with 2 min rest on the bicycle, followed by a 3 min steady state warm-up at 40 or 50 W before gradually increasing resistance at a rate of 20–30 W/min until exhaustion, corresponding to 17–20 on the Borg 6–20 scale.30 In the recovery phase, the participant will stop cycling completely and rest for at least 6 min, until normalisation of blood pressure. VO2peak is defined as the maximal value obtained from a 30 s rolling average of the six consecutive highest VO2 values recorded from the 5 s averaged data.
24-hour ECG monitoring
We use ambulatory 24-hour ECG monitoring at baseline and follow-up to assess arrhythmias that are not properly registered by the ICM and that may be induced by the maximal effort during CPET.
Adverse events
Any unfavourable and unintended sign, symptom or illness that develops or worsens during the trial period will be reported as adverse events (AE). A serious adverse event (SAE) is defined as death, any life-threatening event or any inpatient hospitalisation. In the analyses, AE will be summarised per treatment group by event type, intensity, seriousness and relationship. The timing of SAE will be categorised as occurring during exercise, within the first hour postexercise, or 1–24-hour postexercise. The activity at the time of the event will be further characterised as occurring during training or competition, at rest or during sleep.31 All SAE will be reported to the Study Safety Monitoring Committee (SMC) that will independently evaluate the safety of the study. Formal interim analyses of AE summarised per treatment group will be reported to study SMC after 25% and 50% of the participants have completed the study.
Blinding
This is an open label study and participants are not blinded to group allocation. Researchers and staff are unblinded during all procedures. AF burden will be adjudicated by a blinded endpoint committee.
Data management
Data sources are stored at each participating centre according to local procedures. Data entry is performed by local study personal using a web-based electronic case report form (Ledidi Core, Oslo, Norway). After study completion, before database lock and unblinding, all data from 10% of the participants will be checked by a monitor not involved in the study for consistency with source data. Due to the non-commercial nature of the study, the type of intervention and relatively small study size, we considered a data monitoring committee and formal interim analyses not to be required. The final dataset will be accessed by a statistician blinded to group allocation, and researchers will be blinded when performing statistical analyses.
Statistical considerations
We consider a mean difference in the burden of AF of 0.5% between the detraining group and the control group to be clinically meaningful. A 0.5% difference with a SD in each group of 1% was used to calculate a minimum sample size of 64 participants per group using an independent samples t-test and β=0.2 (power 80%) at α=0.05. However, the primary analysis will be a linear mixed model for repeated measurements and a sample size estimation based on t-test provides thereby a conservative estimate. We also performed a power calculation based on a study of Malmo et al,3 for the outcome difference between the groups in change of AF from baseline to follow-up. In that study AF burden measured with ICMs was reduced by 41% (−3.3% (SD 7.2) from a baseline value of 8.1% (SD 11.2) after a 12-week exercise intervention, compared with+4.2% in the control group). Based on t-tests of means, to detect a difference in change in AF burden of 7.5% between the groups with β=0.2 (power 80%) and α=0.05, a minimum of 28 participants per group is required. Because the baseline AF burden is likely to be lower in the current study than in the study by Malmo, we suggested 60 participants per group. Since we cannot rule out a possible worse outcome in the intervention group, we plan to use a two-sided hypothesis test.
All randomised participants will be included in the main analysis of primary and secondary endpoints. Since adherence to detraining is a secondary outcome measure, major comparisons between randomised groups will be performed by the ‘intention-to-treat’ principle, meaning that patients will be analysed according to the planned intervention. However, some analyses may also be performed using ‘per-protocol’ or ‘as-treated’ data. We define adherence to the detraining intervention as ≥80% of total volume of endurance exercise during the study period performed at an intensity corresponding to a HR of ≤75% of HRmax, based on the exercise monitoring with chest-straps and sports watches.
We plan to publish a detailed statistical analysis plan separately before randomisation of the last study participant.
Trial status
The study has been approved by the ethical committees of the Norwegian Regional Committees for Medical and Health Research Ethics, the Alfred Hospital Human Research Ethics committee, Melbourne, Australia and the Ethics Committee Research UZ/KU Leuven, Belgium. The first study participant was included at Bærum Hospital on 5 January 2022. As of 10 March 2023, 23 participants have been included at three study centres, 9 of which have completed the study. Recruitment is expected to be completed within 2 years, and the results will be communicated through publications.
Clinical implications
Cardiac arrhythmias in athletes represent a major challenge for sports cardiologists. Ventricular arrhythmias and sudden cardiac death in young athletes have been the main focus of research and discussions in this field. AF is a less severe but much more prevalent condition, especially in middle-aged and older male athletes. While several studies and meta-analyses have related the risk of AF to endurance sport practice, the mechanisms underlying this association have been less studied. With the aim to design an intervention that is sufficient to have an effect, but also acceptable to athletes and feasible in real-life, the training intervention in the current study represent a pragmatic compromise with regards to intensity and amount of exercise and duration of the intervention period. Female athletes have been underrepresented in previous studies and the association between endurance exercise and AF is less clear in female compared with male athletes. With the aim to increase the knowledge regarding exercise-induced cardiac remodelling and arrhythmias among female athletes, both female and male athletes are included.32
Conclusion
Endurance athletes with AF and their physicians are left without specific recommendations regarding the preferred exercise intensity to improve symptoms and reduce the risk of AF recurrence. This RCT addresses the feasibility and effects of training adaption in endurance athletes with paroxysmal AF and has the potential to guide development of exercise recommendations for athletes with AF.
Supplemental material
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics approval Ethics committee reference number Norway: REK sør-øst A/212748, Australia: HREC/76210/Alfred-2021 Project No. 470/21, Belgium: Ethics Committee Research UZ/KU Leuven/ S65930. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank Kristine Seland Folkenborg and Vigdis Bache-Semb, Bærum Hospital, for their contribution to the practical organising of the study, Trond-Inge Weatherup, Vestre Viken Hospital Trust, for his contribution with the data management, Are Hugo Pripp, University of Oslo, for assistance with power calculations and statistical considerations, Hilde Larhammer, Bærum Hospital, Asher Knudson and Tor Håkon Grønli, Abbott Norway, for assisting with ICM implantations and programming and Marte Meyer Walle-Hansen, Bærum Hospital, for her help with the figures. This work was executed within the framework of the research consortium the Norwegian Exercise and Atrial Fibrillation Initiative (NEXAF) (online supplemental file 3).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors have contributed to the design of the study. TA and MM drafted the manuscript. All authors read and contributed to the manuscript, gave approval and agreed to be accountable for all aspects of the work.
Funding This study is funded by The Norwegian Health Association and Vestre Viken Hospital Trust, Norway.
Disclaimer The funders did not have any role in the study design and will not have any role in the collection, management, analysis and interpretation of data or in the writing of the report or decision to submit the report for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.