Article Text

Abstract
Objective To determine London emergency medicine (EM) doctors’ physical activity (PA) characteristics, awareness of PA guidelines and PA prescription practice from London emergency departments (EDs).
Methods An anonymous online survey of EM doctors working in London over 6 weeks between 27 April 2021 and 12 June 2021. Inclusion criteria included EM doctors of any grade currently working in London EDs. Exclusion criteria were non-EM doctors, other healthcare professionals and those working outside London EDs. The Emergency Medicine Physical Activity Questionnaire created consisted of two parts: part 1, on basic demographic data and the Global Physical Activity Questionnaire and part 2, focused questions around awareness of guidelines and prescribing characteristics.
Results 122 participants attempted the survey, of which 75 (61.5%) met the inclusion criteria. 61.3% (n=46) were aware of and 77.3% (n=58) achieved minimum recommended aerobic PA guidelines. However, only 33.3% (n=25) were aware of and 48% (n=36) achieved muscle strengthening (MS) guidelines. The mean sedentary behaviour time/day was 5 hours. 75.3% (n=55) of EM doctors thought it was important to prescribe PA, yet only 41.8% (n=23) prescribed PA.
Conclusions Most London EM doctors are aware of and achieve minimum aerobic PA guidelines. Encouraging MS awareness and activities, as well as PA prescribing, should be areas of focus. Larger studies should take place to assess EM doctors’ characteristics in UK regions and data using accelerometers to determine PA more precisely. Further research should also look at patient perceptions of PA.
- Physical activity
- Exercise
- Prevention
- Longevity
- Public health
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Lack of physical activity (PA) is the fourth-leading cause of global mortality. With mounting systemic pressures in the National Health Service (NHS) on urgent and emergency care, emergency medicine (EM) doctors, among others, are experiencing escalating burn-out rates, placing them at higher risk of non-communicable and communicable diseases, such as COVID-19. Meeting PA guidelines can improve physical and mental health and increase resilience in front-line healthcare staff such as EM doctors.
WHAT THIS STUDY ADDS
While only two-thirds of EM doctors know PA guidelines, over three-quarters achieve minimum recommended levels. Less than half of EM doctors achieve muscle strengthening guidelines, with only a third aware of them, while three-quarters of EM doctors feel it is important to prescribe PA, but less than a third do in practice.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study provides a baseline of EM doctors’ PA characteristics around awareness and achievement of PA guidelines as well as basic lifestyle medicine interventions around PA prescribing behaviours, which can be used to focus resources on improving the health of patients and healthcare staff alike.
Introduction
Lack of physical activity (PA) is recognised by the WHO as the fourth-leading cause of mortality worldwide. The latest evidence shows that one in four adults do not meet minimum recommended guidelines,1 which prompted a global action plan.2
Strong evidence underpins the widespread holistic benefits of PA in non-communicable diseases (NCDs).1 At the start of 2020, the WHO declared COVID-19 a global pandemic.3 Subsequent studies have shown the increased risk to health posed by front-line healthcare professionals (HCPs)4 and highlighted the protective effects of PA against infectious diseases, including COVID-19.5 6 PA can also increase resilience among staff,7 pertinent at times of increased psychological distress.8 Now more than ever, front-line HCPs must engage in self-care to maintain good health and reduce burnout.9 Awareness and subsequent achievement of weekly minimum PA guidelines is one such adjustable lifestyle factor to do this.9 10
Emergency medicine (EM) doctors have a duty to both themselves and their patients.11 A recent study by Crane et al showed that only 57% of EM doctors were considered active, with 55–64 years being the most active and 25–34 years being the least active.12 Chatterjee et al highlighted that 80% of general practitioners (GPs) in England were unfamiliar with PA guidelines,13 and Soegtrop et al showed that only 12.7% of Canadian (EM) doctors prescribed PA.14
In 2016–2017, over 4.1 million patients attended London emergency departments (EDs),15 just under half of the estimated London population at the time.16 With the Royal College of Emergency Medicine (RCEM) declaring ever-rising numbers of patients attending UK EDs, rising emergency admissions17 and emerging evidence that an increasing proportion of patients are seeking to use EDs for primary care,18 EM doctors are optimally placed to prescribe PA. A recent qualitative study by Osinaike and Hartley further supports this. Some junior doctors felt they had more contact time with patients than in a primary care setting.19
At the time of writing, no studies looked at these elements within this cohort. The primary aims were to determine London EM doctors’ own PA characteristics and their awareness of PA guidelines. The secondary aims were to determine PA prescription practice from EDs, perceived barriers and solutions to improve this.
Methods
An anonymous online survey of EM doctors working in London, UK, during Spring 2021 over 6 weeks from 27 April 2021 to 12 June 2021.
Participants and procedure
Participants who met the inclusion criteria of EM doctors of any grade working in a London ED were invited to complete the voluntary survey. Exclusion criteria were: non-EM doctors, other HCPs and those working outside London EDs. According to Health Education England, the London School of EM has over 300 trainees,20 and an estimated 170 EM consultants are working in London. Furthermore, local EDs had 26 foundation year (FY) and junior clinical fellow doctors and 28 GPs, giving an estimated reach of 524 doctors. The target was to achieve as many responses as possible.
The survey was distributed via established local networks, including departmental, all grades of local doctor EM teaching networks and wider pan-London higher trainee EM teaching networks. This was done in a phased manner over the total 46 days the survey was live, with a reminder email sent after 1 month. The survey only allowed one response and submission per participant via internet cookies. Distribution was not done via social media platforms to reduce the risk of completion by responders not meeting inclusion criteria. The survey was administered via Opinio, a web-based survey tool used by University College London (UCL).21 Data were stored in compliance with UCL Research Data Policy.22 Consent was agreed on by the commencement of the survey. Participants could exit the survey at any time, and in line with consent, data from questions completed could be used in the analysis.
The Emergency Medicine Physical Activity Questionnaire created (online supplemental appendix A) was structured into two parts. After a local study group and feedback from a pilot questionnaire, part 1 focused on the primary aim of doctors’ PA behaviours with basic demographic data of personal and professional factors. Part 2 consisted of the widely used Global Physical Activity Questionnaire (GPAQ)23 involving: activity at work, travel to and from places, recreational activities, sedentary behaviour (SB) and muscle-strengthening activities. It also focused on the remaining aims, consisting of questions about awareness of guidelines and prescribing characteristics. To progress through the survey, participants had to complete each question appropriately and were prompted if needed. As per recommendations, participants could meet aerobic PA guidelines via a combination of moderate-intensity PA (MIPA) or vigorous-intensity PA (VIPA).1 Results are presented in line with the Checklist for Reporting Results of Internet E-surveys.24
Supplemental material
Measures
The GPAQ is a widely used 16-item PA questionnaire developed by the WHO to monitor VIPA, MIPA and SB in countries.23 It has been widely validated in large-scale populations.25–27 The GPAQ was originally designed to be used with an interviewer.23 However, a recent study showed the use of show cards had no significant impact on validity28 so show cards were not used.
The measures assessed the current state in ‘recent times’, during the easing of restrictions of a third national lockdown due to the pandemic.29 The survey had to be detailed enough to allow the opportunity for comparisons but short enough to encourage completion.30
Analysis
Raw data were checked after the survey submission deadline, and data were further excluded if the absence of a predetermined minimum required dataset, consisting of age, gender, grade, hospital and sufficient GPAQ completion. As this is novel research, descriptive statistics were used to analyse data. Means were used where data were normally distributed, and medians were used when data were not normally distributed. All analysis and statistical output were produced using Numbers (V.11.1 (7031.0.102)).31
Results
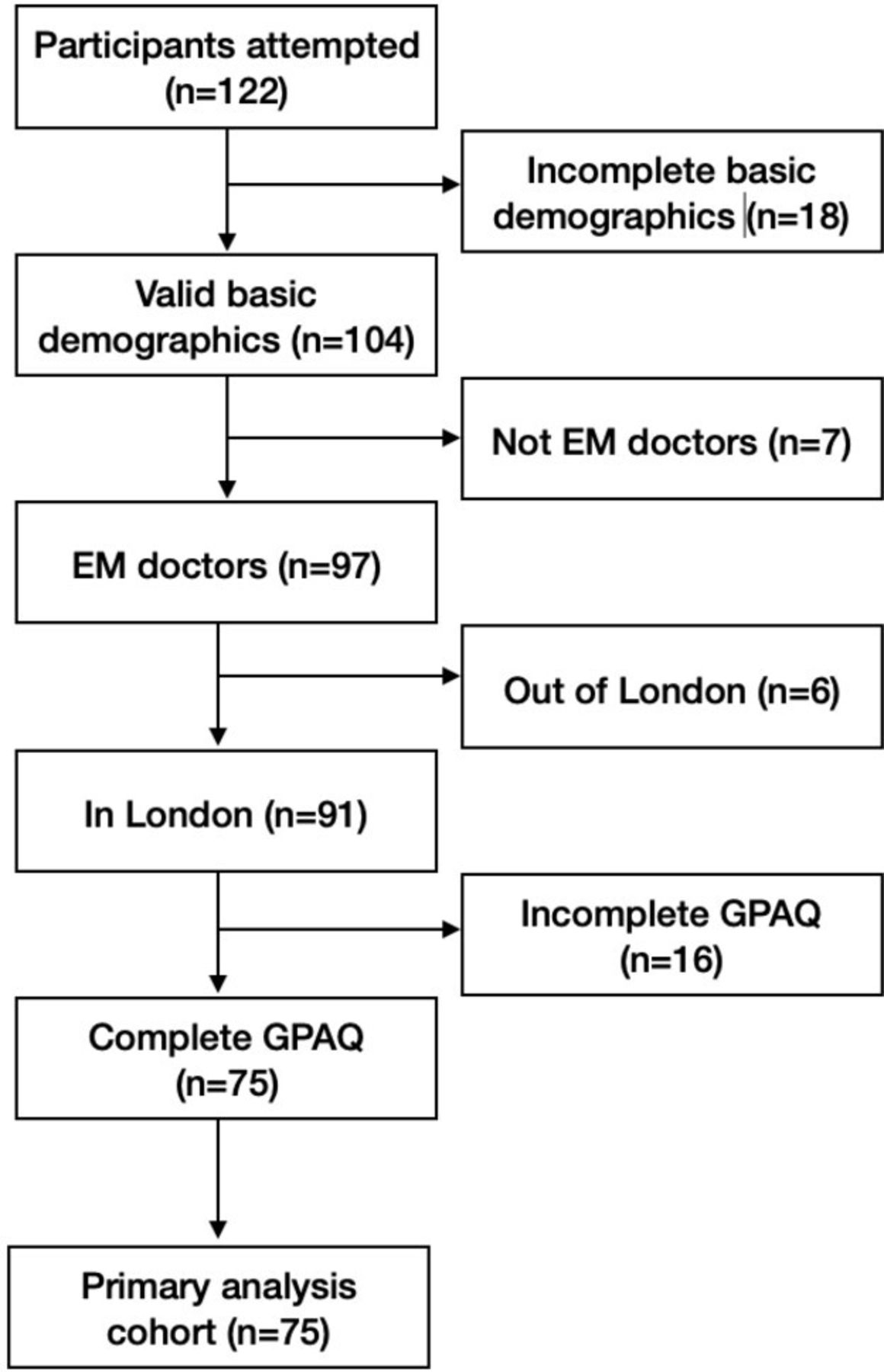
Enrolment is summarised in figure 1.

EMPAQ analysis flow chart. EM, emergency medicine; EMPAQ, Emergency Medicine Physical Activity Questionnaire; GPAQ, Global Physical Activity Questionnaire.
Overall, 122 participants accessed the survey, of which 75 (61.5%) were suitable for analysis. This represents a sample size of 14.3% from the available cohort of 524 doctors. Extrapolating workforce data from RCEM, there are an estimated 1968 EM doctors in London,32 meaning an estimated overall sample size of almost 1 in 26 (3.8%).
Sample characteristics
Study population demographics are summarised in table 1, and comprehensive study population demographics with associated key primary and secondary outcome characteristics are summarised in online supplemental table 1.
Supplemental material
Basic demographic characteristics
General characteristics
The median age of the study population was 33 years (mode 30 years, range 26–66 years). The mode age bracket was 26–30 years (n=28, 37.3%). Over half of the participants were males (n=40, 53.3%). Apart from FY1, all grades of doctors were represented, with middle-grade trainees/registrar-level junior doctors being most commonly represented (CT3–6), as shown in table 1. All three London region deaneries of EM were represented, with North West London (NWL) having the highest uptake (n=44, 58.7%). Almost all official UK government ethnic groups were represented,33 with the most common 3 groups being white British (n=34, 45.3%), Indian (n=11, 14.7%) and any other Asian (n=7, 9.3%). Marital status’ most common three categories were: in a relationship (n=37, 46.7%), followed by both single and married (n=18, 24%). The mean male body mass index (BMI) was 24.0 kg/m2 (range 19.1–31.6), and the mean female BMI was 22.9 kg/m2 (range 16.9–31.6).
Non-responder characteristics
Available data of non-responder participants (those who commenced the survey but provided incomplete data) are represented in online supplemental table 2. The limited data for incomplete basic demographics are variable with no obvious trends. The data for incomplete GPAQ overall shows that: younger age brackets, males, white and Asian ethnicities and those outside of NWL were less likely to complete this part of the survey.
EM doctors’ PA characteristics
Participants’ work, and recreational VIPA and MIPA data are represented in table 2. Most responders did not consider a typical day at work to consist of either VIPA (n=71,940.7%) or MIPA (n=54, 72.0%). However, over two-thirds said they did both recreational VIPA (n=51, 58.0%) and MIPA (n=53, 70.7%) for a median of 4 days/week and a median of 45 min and 60 min per day, respectively.
Participants’ work and recreational VIPA and MIPA
With participants able to select multiple answers, PA barriers and solutions to increase PA are represented in descending order in table 3.
Barriers as well as solutions to increase PA
Active transport characteristics
Most participants did walk or cycle for at least 10 min/day (n=51, 68.0%) for a median of 5 and a half days/week and 50 min/day, as per table 4.
Active transport characteristics
Muscle strengthening characteristics
Participant median times/week undertaking muscle strengthening (MS) activities involving all major muscle groups was 2 days (mode 0 days, range 0–7 days).
SB characteristics
The typical mean time/day spent sitting or reclining was 5 hours (median 5 hours, mode 3 hours, range 0–12 hours/day). Over half of the participants were aware of the latest PA and SB guidelines (n=46, 61.3%), as shown in table 5.
Awareness of SB and MS guidelines
Awareness of guidelines characteristics
Achievement of guidelines characteristics
Overall, over three-quarters of participants achieved typical weekly aerobic PA guidelines (n=58, 77.3%) either at work or recreationally, with over half achieving guidelines via active transport (n=41, 54.7%), as shown in figure 2. However, less than half of the participants achieved MS guidelines (n=36, 48.0%), and only one-third were aware of MS guidelines (n=25, 33.3%), as shown in figure 3.
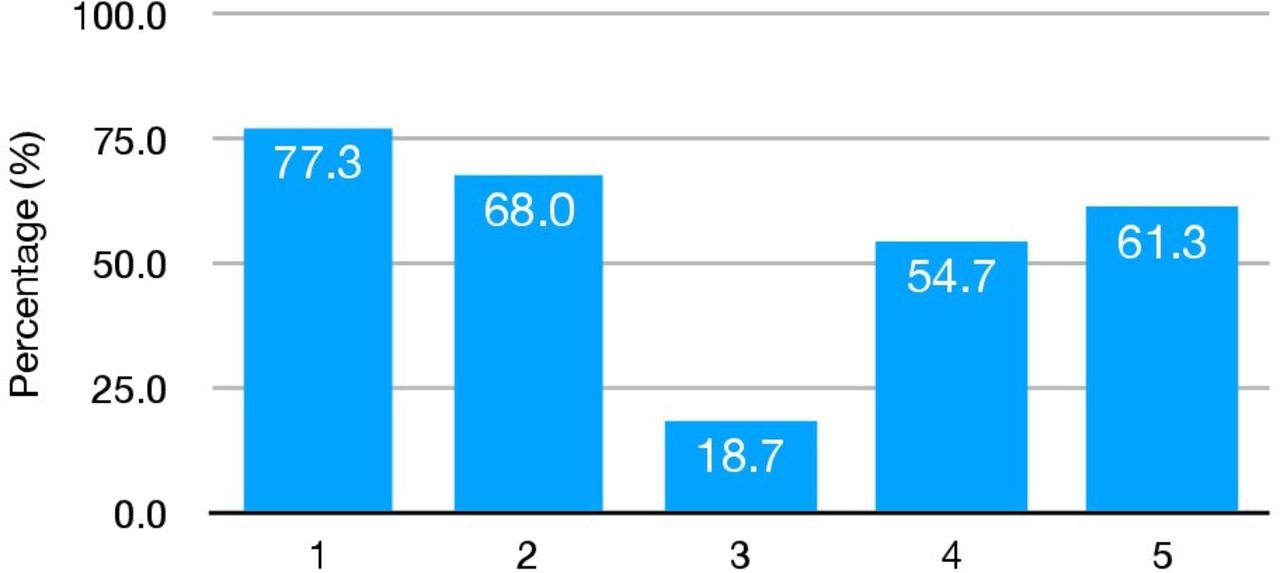
Percentage who: (1) overall achieve minimum aerobic PA guidelines recreationally or at work (n=58), (2) just recreationally (n=51), (3) just at work (n=14), (4) via active transport (n=41) vs (5) awareness of guidelines (n=46), respectively. PA, physical activity.
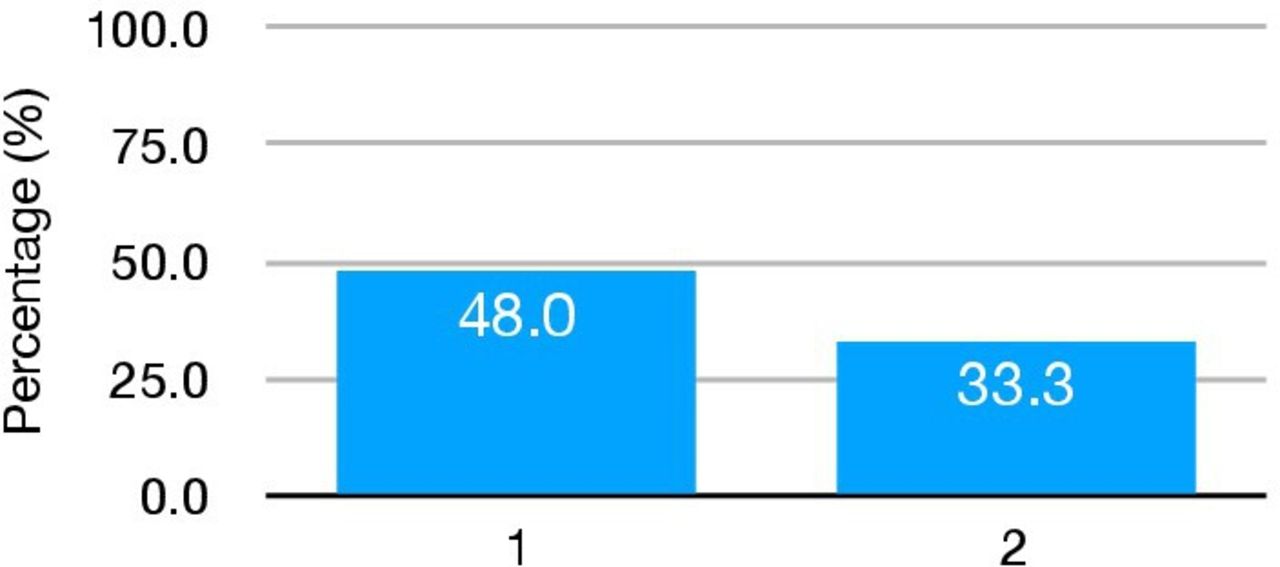
Percentage who: (1) achieve MS guidelines (n=38) vs (2) who are aware of MS guidelines (n=25). MS, muscle strengthening.
Online supplemental table 3 shows the characteristics when making comparisons across different categories, including (1) those who are both aware of and achieve minimum PA and MS guidelines (n=10, 7.5%); (2) those who achieve minimum PA and MS guidelines and also prescribe from ED when appropriate (n=11, 14.7%); (3) those who are aware of PA and MS guidelines and prescribe from ED when appropriate and (4) those who achieve all three of: aware and achieve minimum PA and SB guidelines and also prescribe from ED when appropriate (n=6, 8.0%), which is summarised in figure 4.
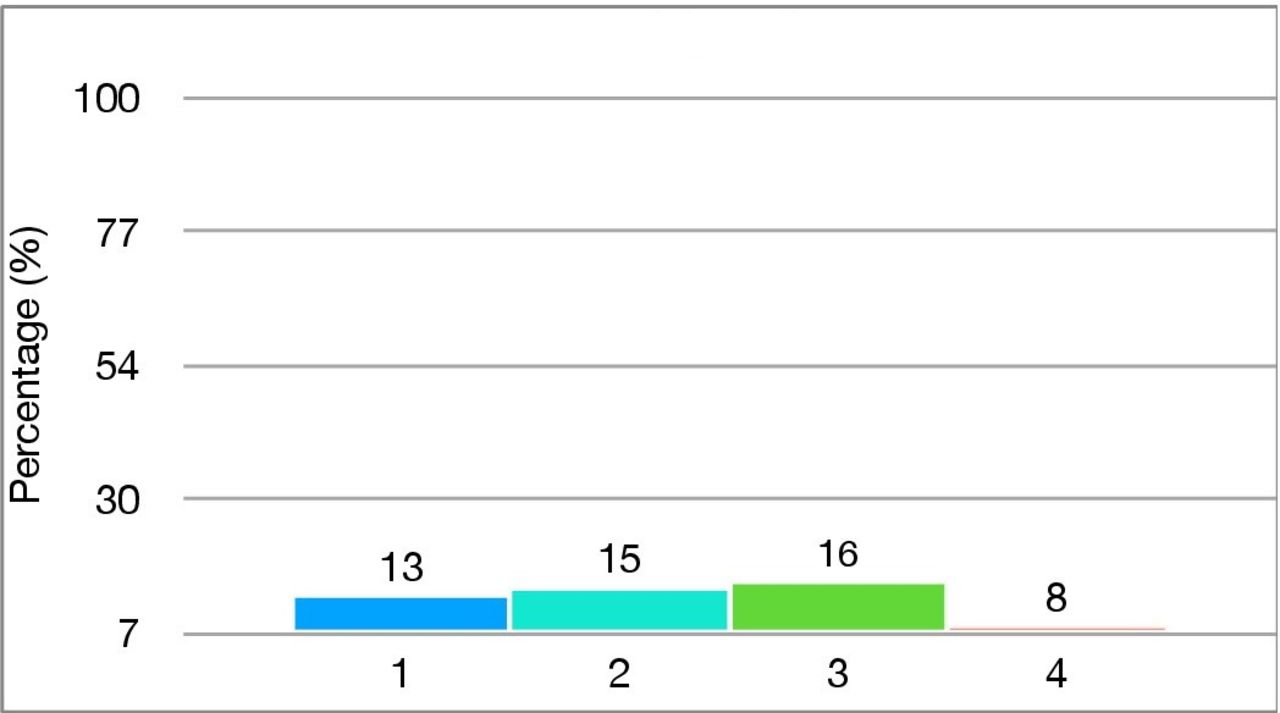
Percentage who: (1) aware and achieve minimum PA, MS, SB guidelines (n=10), (2) achieve minimum PA, MS guidelines and prescribe from ED (n=11), (3) aware of PA, MS guidelines and prescribe from ED (n=12) and (4) who are aware and achieve minimum PA, MS guidelines and prescribe from ED (n=6). ED, emergency department; MS, muscle strengthening; PA, physical activity; SB, sedentary behaviour.
Certain patterns can be seen across the four categories of comparison. First, those under 50 years (peaking with those aged 36–40) were present in all four categories, while, other than two in category 3, no one over age 51 was. In terms of gender, males achieved all four categories more than females. However, this difference was minimal. Ethnicity-wise, Arab and ‘white Irish’ appeared in all categories, followed by Indian, then ‘any other white background’ and ‘white British’. Being married, followed by being in a relationship (other than one separated in category 2 and one divorced in category 3), was also a trend seen. Current and ex-smokers achieved all four categories, as did those with no comorbidities (apart from two in category 3). This also applied to those with a healthy BMI, followed by those with an overweight BMI. EM middle-grade doctors (particularly SCF doctors) and GPs achieved higher in all four comparisons. However, FY2 doctors and consultants did not. All London regions attained comparable numbers across the categories, as did those with a good and above self-health rating.
Effects of COVID-19 pandemic characteristics
Overall the majority of participants thought that the COVID-19 pandemic had reduced their PA levels (n=40, 55.6%), increased their SB levels (n=46, 63.9%) and reduced their MS activities (n=38, 53.5%), as shown in table 6.
Effects of Coivd-19 PA characteristics
EM doctors prescribing characteristics
Just over three-quarters of participants thought it was important to prescribe PA from London EDs (n=55, 75.3%). However, fewer than half of those prescribed PA (n=23, 41.8%), as shown in figures 5 and 6, respectively. The top three barriers, followed by the top three solutions to prescribing PA, are shown in figures 7 and 8, respectively.

Do you feel it is important to prescribe PA from London EDs when appropriate? (n=73). EDs, emergency departments; PA, physical activity.

Of those who feel it is important, do you prescribe PA from London EDs when appropriate? (n=55). EDs, emergency departments; PA, physical activity.
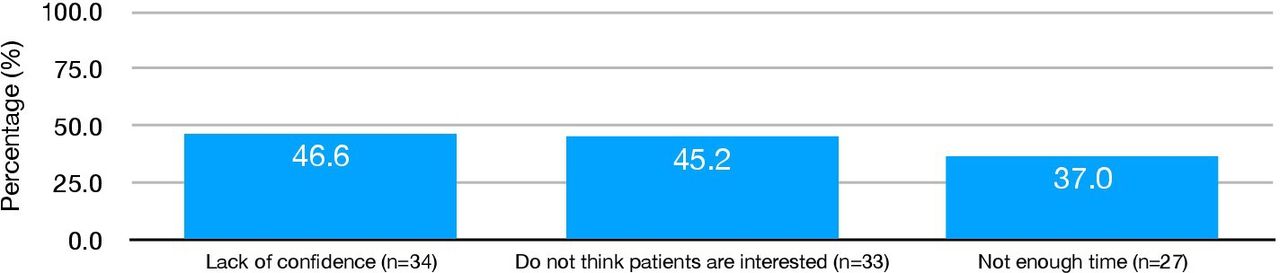
Top three barriers to prescribing PA from London EDs (n=73). EDs, emergency departments; PA, physical activity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Top three solutions to help you increase PA prescription from London EDs (n=72). EDs, emergency departments; PA, physical activity.
Discussion
This survey of 75 London EM doctors demonstrated that over three-quarters achieved the minimum recommended levels of PA as set out by both UK guidelines34 and, more recently, the WHO 2020 guidelines.35 However, less than two-thirds were aware of such guidelines. The same proportion of three-quarters feel it is important to prescribe PA from London EDs, yet less than one-third do.
Note that 4 (5.3%) and 21 (28.0%) participants considered typical daily work to be VIPA and MIPA, respectively. Other than a few limited situations, such as chest compressions during cardiopulmonary resuscitation, which is, fortunately, still considered uncommon,36 daily work is not expected to consist of VIPA or MIPA. Explanations were clearly made before each relevant question to clearly define VIPA and MIPA (online supplemental appendix A), which still suggests a lack of understanding of the intensity of PA.
Compared with Crane et al, our EM doctor cohort overall was just over 20% more active,12 with over 71.4% compliance in all age brackets. No other studies were found at the time of the write-up looking at the PA of EM doctors. Compared to the Adult Active Lives Survey May 2020/2021 Report, our cohort is a minimum of greater than 10.5% more active overall. In agreement, males are just more active than females, mixed and white groups are more active than Asian or Black ethnic groups, and our cohort maintained activity levels as age increased. Doctors are considered higher socioeconomic groups, thus having similarly higher activity levels than lower groups which may help explain this.37
Less than half of participants achieved MS guidelines, with only one-third aware of them, and this reduces with age. This aligns with why in the latest UK CMO guidelines, MS activities were highlighted as an area requiring public health focus.34 MS activities and those that incorporate balance are important to reduce both fall risk and subsequent injury risk from falls, which make up the largest number of ED attendances in older adults, having a significant impact on morbidity, mortality as well as economic.38
Participants spent an average of 5 hours/day sitting, so 3–5 hours/day less when compared with a healthy adult population by Metcalf et al (8–10 hours/day),39 Laeremans et al (08:55 hours/day)40 and roughly half the time/day when compared with a national Canadian population using accelerometers (~9.7 hours/day when comparing similar age groups).41 The day-to-day job as an EM doctor is relatively active and non-sedentary, involving many changes in position and light-intensity PA, such as walking, to engage patients and complete tasks. Schaller et al, however, did show the underestimating of SB using the GPAQ by 122 min/day (02:02 hours/day)42 and Cleland et al by over half.27
Our category 1–4 comparisons highlight some trends that could serve as a baseline for characteristics of those being aware and achieving PA guidelines and prescribing PA. These data can help focus resources on higher age brackets, selected ethnicities, extremes of BMIs, those with comorbidities, more junior and senior grades, and those with lower self-health ratings.
Data were collected during easing measures of the third UK COVID-19 lockdown, so it was important to try to gauge the effects of the pandemic on overall activity levels at work and recreationally. Our data suggest an overall negative impact on all three aspects of reducing PA, increasing SB and reducing MS activities, in line with other studies.43 44 Gym access, organised sport and social opportunities were gradually reintroduced.29 Moreover, increased remote working or teaching with the use of online technologies leading to reduced commuting would all likely have negatively impacted participants’ PA, SB and MS activities in line with a recent systematic review.45 On the other hand, it is promising to see that under half of the participants either did not change or increase their PA (n=32, 44.4%) and MS activities (n=33, 46.5%), while just over one-third maintained or decreased their SB (n=26, 36.1%) during this period of disruption, which could be due to development of new positive habit formation46 or higher work-based activity due to the pandemic. Organisations and policy-makers should consider undertaking further research and look into infrastructure improvements or rotas changes, given the solutions to enhancing PA centred around the lack of available on-site facilities and shift work.2 47
Our PA prescription data builds on the limited data available and could serve as a new baseline for future research, as no barriers highlighted were directly related to COVID-19. Over three-quarters of participants think it is important to prescribe PA, yet well under half do. This is, at least, almost threefold what was reported by Soegtrop et al.14 Theirs, in line with this study, also highlighted lack of time as a barrier to PA prescription. Additionally, Osinaike and Hartley identified a lack of knowledge and confidence from inadequate undergraduate and postgraduate medical training and insufficient senior support as barriers to brief PA counselling, which should be urgently addressed by responsible medical training establishments. Supporting doctors' PA habits could also positively reinforce their PA prescribing practice.19 Another barrier highlighted was concern over patient interest in receiving PA advice. One in four patients would do more PA if advised by an HCP, so further work is needed.48 In addition to the suggested solutions (figure 8), simple steps such as screening patients for PA, motivational interviewing49 and creating multidisciplinary links with primary care and other fields, for example, physiotherapy, strength and conditioning coaches, could be avenues to explore to improve patient PA uptake.
Studies have shown that habitual PA is associated with a 30%–40% lower risk of severe infectious disease (including COVID-19) after accounting for confounders,5 6 so now is as an important time as ever with the growing issues of rising physical inactivity,1 rising NCDs50 and increasing number of patients receiving their care from EDs.17 These simple solutions should be trialled, and a follow-up study should be conducted looking for improved parameters of PA for EM doctors, increased awareness and increased prescribing.
Our study is limited by a small sample size (we were unable to contact those who provided incomplete survey data as this was an anonymous survey) and retrospective data collection occurring during the tail end of the unprecedented COVID-19 pandemic, which should be factored in if using specific data on EM doctors’ own PA characteristics as a baseline. Only MS frequency was used in line with the GPAQ. However, there could be vast variations in intensity and time spent doing this activity, so eliciting health benefits here is limited. Further limitations in keeping with survey studies also apply, including response bias and social desirability bias. Studies have also shown that in self-reported PA surveys, participants significantly overestimate their PA levels using the GPAQ42 by up to 2–3 fold,26 so further research should consider pairing PA survey data with accelerometers. Although survey completion time was typically between 5 and 7 min, EM doctors are busy, shift work is unpredictable and front-line staff have suffered psychological distress during the pandemic.8 All these factors could have deterred potential participants from completing the survey.
Conclusion
Based on survey data, most London EM doctors know and achieve minimum PA guidelines. Encouraging MS awareness and activities should be an area of focus. Only a minority of London EM doctors prescribe PA from London EDs, despite acknowledging it is important. Future work incorporating both top-down and bottom-up system approaches should be employed to monitor London EM doctors’ PA characteristics and their own PA guideline adherence and improve PA prescription to enhance patient care.
Further research should take place to assess EM doctors’ characteristics in UK regions. Larger studies incorporating the use of accelerometers in this cohort to more precisely determine PA levels are needed, as well as research to understand patient perceptions around receiving PA advice from EDs when appropriate.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
As this was an anonymous survey of NHS staff, in line with UCL Ethical Research Guidelines, no ethics committee approval was required.Available at: https://www.ucl.ac.uk/research-ethics/ethical-approval/do-i-need-ucl-ethical-approval. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank the Royal College of Emergency Medicine (RCEM) for the endorsement of the study. The authors would also like to thank London emergency medicine doctors for their consent and time to take part in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KK, ET and ML conceived the study idea. KK designed the study, collected and analysed data and wrote the manuscript with supervision from ET. ET and ML reviewed data and contributed to the final manuscript. ML is the author aciting as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.