Article Text

Abstract
Introduction The cardiovascular benefits of physical exercise are well-known. However, vigorous exercise has also been associated with adverse cardiac effects. To improve our understanding of cardiovascular adaptation to exercise versus maladaptation and pathology, the limits of adaptation should be firmly established using state-of-the-art diagnostic modalities. We therefore initiated the Evaluation of Lifetime participation in Intensive Top-level sports and Exercise (ELITE) cohort to investigate the longitudinal (beneficial and pathological) cardiovascular effects of intensive elite sports and exercise.
Methods and analysis ELITE is a prospective, multicentre, longitudinal cohort study. Elite athletes, from the age of sixteen, are recruited in The Netherlands. The primary objective is to determine the association between elite sports and exercise-induced cardiac remodelling, cardiac pathology, and health benefits over time. Secondary objectives include determining and identifying genetic profiles of elite athletes, and how these are associated with cardiac indices. ELITE will collect data from consultations, electrocardiography, echocardiography and cardiac magnetic resonance imaging, and training- and injury data. ELITE will also collect blood for biobanking and cardiogenetics. Follow-up will take place at intervals of two to five years, and after the elite athletes’ professional careers have ended. In addition, a subcohort of ELITE has been established to investigate cardiac sequelae following infections associated with myocardial involvement, including SARS-CoV-2. ELITE is a prospective observational study; therefore, analyses will be primarily explorative.
Ethics and dissemination This study has been approved by the Medical Ethics Review Board of the Amsterdam University Medical Centers (NL71682.018.19). The results of the study will be disseminated by publication in peer-reviewed journals (Netherlands Trial Register number: NL9328).
- Athlete
- Cardiology prevention
- Sports & exercise medicine
- Prospective
- Elite performance
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Minimum amounts of physical exercise associated with beneficial cardiovascular and general health are well known.
Extreme levels of exercise are potentially associated with detrimental cardiac effects.
It is unclear what the upper cardiovascular limits are for individuals engaging in (extreme levels of) sports and exercise.
WHAT THIS STUDY ADDS
Knowledge on cardiovascular remodelling, cardiac pathology and health benefits over time of elite sports and exercise.
Insights into genetic profiles and associations with cardiac indices in elite athletes.
Longitudinal assessment of cardiovascular athlete phenotypes, even after the elite athletes’ professional careers have ended.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Facilitate differentiation between exercise-induced cardiovascular remodelling and pathology.
Assist in personalising sports and treatment advice for athletes and patients at risk or with cardiovascular pathology who wish to engage in sports and exercise.
Establish comprehensive extreme phenotypes and genotypes in elite athletes, constituting the limits of cardiovascular adaptation to sports.
Introduction
Current sports and cardiovascular guidelines define the minimal amount of physical exercise and sports that are associated with cardiovascular and general health benefits.1 2 However, emerging evidence suggests that there is an upper limit to these health benefits and that physical exercise beyond these limits may have detrimental cardiac effects.3 First, numerous studies have described sports being associated with morphological changes such as cardiac dilatation, ventricular hypertrabecularisation and hypertrophy, the release of cardiac biomarkers (eg, troponins, natriuretic peptides), an increased risk of supraventricular arrhythmias, myocardial fibrosis and adverse events in (young) athletes with coronary anomalies.4 Second, the role of physical exercise and sports as a second hit or trigger for developing cardiomyopathies, and consequently progression of disease and risk of arrhythmias, remains largely unclear. Whereas in PKP2 mutation carriers, an association has been described between exercise and worse arrhythmogenic cardiomyopathy (ARVC) outcomes,5 6 for the majority of pathogenic mutations, data on this association are lacking. Consequently, there is an unmet need for clear sports-specific advice in asymptomatic individuals who are known to carry potentially pathogenic mutations. Finally, elucidating the association between sudden cardiac death and sports remains one of the central challenges in sports cardiology and sports and exercise medicine.
Despite these knowledge gaps, an increasing percentage of the world’s population, and especially women, is engaging in sports and exercise at a far higher level than the minimal recommendations.7 8 Moreover, competitive and professional athletes continue to push the boundaries of what is thought possible in athletic performance. These developments emphasise the importance of determining whether there are upper limits for the amount of exercise and cardiac safety, and being able to identify individuals at risk of detrimental cardiovascular effects as a result of sports and exercise. Additionally, little is known about continued sports participation with various cardiac abnormalities. Certain countries and sports federations strongly restrict or disqualify athletes with (minor) cardiovascular abnormalities from sports participation, while the long-term consequences of these findings regarding cardiac safety and return-to-play protocols are still unknown. These knowledge gaps reflect, at their heart, a lack of prospective, comprehensive phenotyping and genotyping in individuals exposed to extreme sports volumes; that is, extreme phenotyping and genotyping studies, where the limits of healthy adaptation to sports are rigorously and elaborately described.
Therefore, we initiated the Evaluation of Lifetime participation in Intensive Top-level sports and Exercise (ELITE) cohort, aiming to investigate the longitudinal cardiac effects of intensive elite sports and exercise, cardiovascular adaptation and the development of cardiac pathology over time, in a large sample of elite athletes during and after their sports career. We also aim to provide a first insight into the genetic background of elite athletes and to compare these findings to the known genetic variability of the general population.
Methods
Study design
ELITE is a prospective, multicentre, longitudinal cohort study. To date (21-11-2022), 311 elite athletes have been included in this study in five medical centres in The Netherlands with sports cardiology expertise: (1) Amsterdam University Medical Centers (Amsterdam UMC), (2) University Medical Center Utrecht, (3) Tjongerschans hospital, (4) Maxima Medical Center,and (5) Gelderse Vallei hospital. Study participants are recruited through voluntary preparticipation cardiovascular screenings or by their personal sports physicians. After inclusion, ELITE collects data from all available cardiovascular examinations, such as preparticipation screening data, clinical cardiac analyses and training and injury data, including data collected in the Dutch National Olympic Committee & National Sports Federation (NOC*NSF) athlete management system (Smartabase) (figure 1). Additionally, ELITE will perform blood collection to determine cardiogenetic profiles and for biobanking. ELITE includes follow-up measurements of voluntary preparticipation cardiovascular screenings, which routinely take place at 2–5-year intervals, and consent is obtained to contact athletes for structured follow-up after cessation of their elite sports careers.
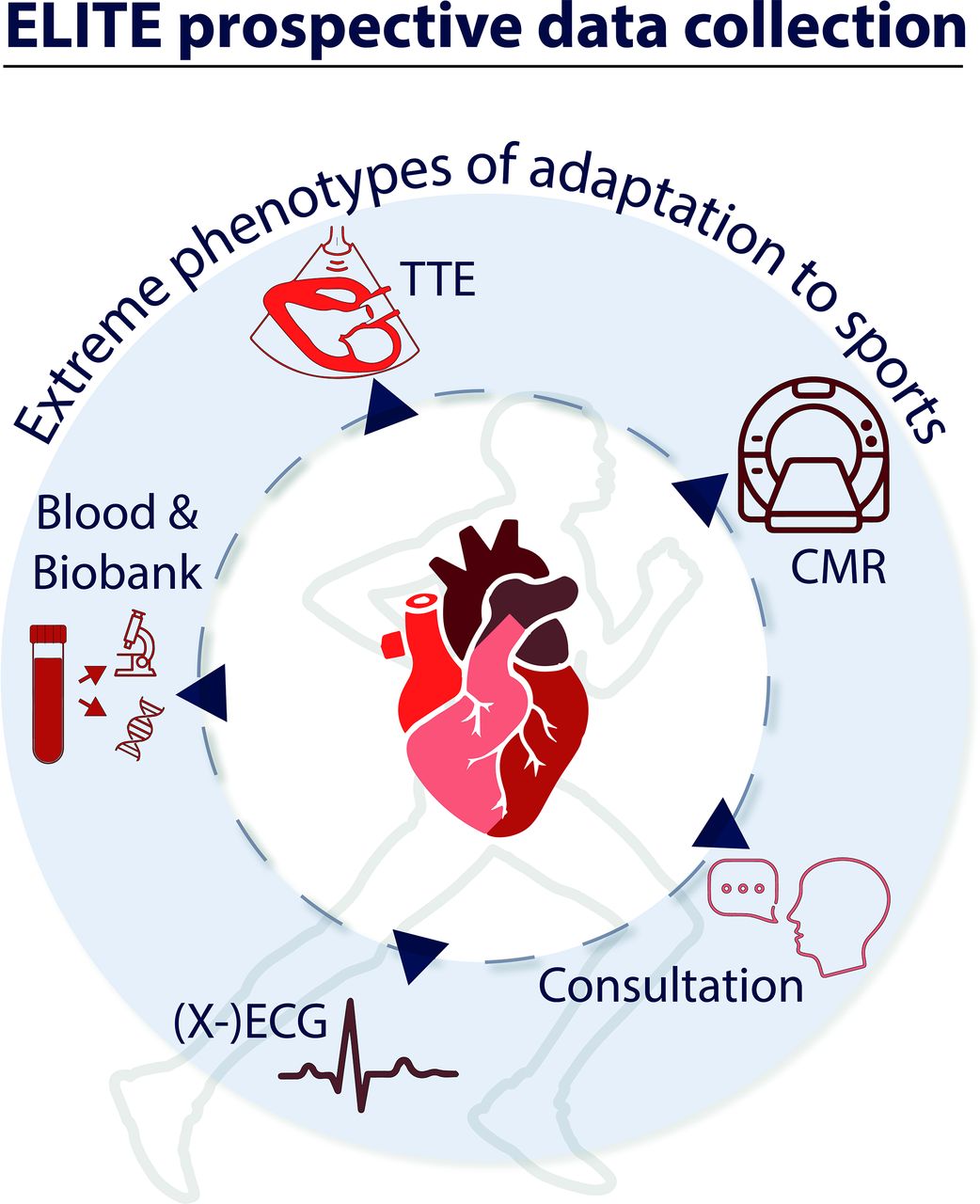
{kind=link}
Design of the ELITE study. CMR, cardiac magnetic resonance; ELITE, Evaluation of Lifetime participation in Intensive Top-level sports and Exercise; TTE, transthoracic echocardiography.
ELITE has been approved by the Amsterdam University Medical Centers Medical Ethics Review Committee (NL71682.018.19). This study is conducted according to Helsinki declarations and adheres to the CONSORT guidelines (Netherlands Trial Register Identifier NL9328).
Study objectives
The primary objective of ELITE is to identify the association and variance of various types of elite sports and exercise on exercise-induced cardiac remodelling, cardiac pathology and health benefits over time, in elite athletes. Secondary objectives include determination and identification of genetic profiles of elite athletes and investigation of how genetic profiles are associated with cardiac indices and various types of extreme levels of elite sports.
Study population
The ELITE study population consists of elite athletes participating at national, international, Olympic or Paralympic levels in the Netherlands. Elite athletes (ie, Olympians, Paralympians) are defined as individuals of young or adult age, who engage in regular exercise training and participate in official sports competitions, who generally exercise more than 10 hours per week, and aim to win or to improve their performance.1 To be eligible to participate in this study, a subject must be an elite athlete, aged 16 years or older and be motivated to participate in the voluntary cardiovascular preparticipation screening programme. Athletes will only be excluded from participation if they wish to withdraw from the study. After inclusion, athletes remain in the study regardless of sports participation and sports status.
Eligible athletes will be informed about the content and goals of ELITE during their voluntary cardiovascular preparticipation screening, and simultaneously asked for informed consent to be included in ELITE. Informed consent will be obtained by the investigators specified in the Medical Ethical protocol. Specific consent will be asked for: (1) inclusion into the cohort; (2) follow-up and collection of cardiac event and relevant clinical data; (3) data collection of cardiac examinations and from Smartabase® (including personal wearables); (4) blood samples for cardiogenetics and biobanking.
Sample size considerations
Exercise-induced cardiac remodelling in elite athletes performing at the upper limits of intensive exercise has been described predominantly in men and cross-sectional studies with small sample sizes.9 Therefore, ELITE aims to qualitatively assess extreme phenotyping in elite athletes, to serve as a unique sports-specific baseline reference for the boundaries of extreme cardiac phenotypes. In addition, genotyping and second hits, such as inflammatory diseases, have to date not been assessed in large elite athlete cohorts, but mainly in smaller cohorts or through survey data, demonstrating an incidence of 0%–5% of inflammatory cardiac sequelae.10 Therefore, ELITE aims to include the whole Olympic, and Paralympic Dutch selection, with a minimum of 1000 elite athletes (~40% female athletes) of various sports disciplines. While this study is mainly exploratory, based on population prevalences and existing data in (subelite level) athletes, with a sample size of 1000 athletes we expect to identify 8% (n=84) athletes with dimensions as seen in dilated cardiomyopathies,11 and 1.7% (n=17) athletes with a wall thickness within ranges compatible with the diagnosis of hypertrophic cardiomyopathy (≥13 mm).11 Additionally, we expect to identify 24% (n=240) of male athletes with RV dimensions exceeding the upper limits of normal for the general population—hence with suspicion of ARVC based on morphological criteria,12 and up to 5% (n=50) with postinflammatory cardiac sequelae.10
Data collection
ELITE will collect data obtained from voluntary cardiovascular screenings, in addition to training and injury data, including data from the NOC*NSF athlete management system (Smartabase), and perform ELITE-specific data collection/investigations consisting of determinations of exercise-induced electrical, functional, structural and peripheral changes. The voluntary cardiovascular preparticipation screening and data collection are part of the voluntary usual care of elite athletes. The additional measurements of ELITE consist of blood collection for biobanking and cardiogenetics.
National cardiovascular (pre)participation screening (SMART)
In 2019, the SMART (Selective Medical Advanced CaRdiovascular Top-level sports—screening) project was launched.13 The SMART project was cocreated by the national Olympic committee (NOC*NSF) and the Sports Section of the Netherlands Society of Cardiology. SMART constitutes a uniform, voluntary national preparticipation screening strategy for elite athletes participating in Dutch sports competitions. This periodic screening consists of (1) sports physician consultation and physical examination; (2) electrocardiography (ECG); (3) cardiopulmonary exercise testing (CPET); (4) laboratory testing, in addition to strictly protocolised (5) transthoracic echocardiography (TTE); and (6) cardiac magnetic resonance (CMR) imaging. The SMART screening aims to identify individuals with a clear and prohibitive risk of sudden cardiac arrest using state-of-the-art diagnostic modalities and includes periodic follow-up, according to findings, in general every 2–5 years.
Smart preparticipation protocol
Resting ECG
Standardised digital 12-lead supine resting ECG will be performed. Measurements and quantification of the ECG will be assessed according to the international recommendations for electrocardiographic interpretation in athletes.14
CPET
CPET will be performed preferentially using a cycle ergometer or a treadmill. We will use raw and unfiltered breath‐by‐breath gas analyses of O2 and CO2, integrated pulse oximetry (SpO2) with preferably an earlobe or forehead sensor for continuous measurements and continuous 12‐lead ECG monitoring. Cycle ergometer tests are recommended in SMART, but sport-specific tests are allowed, for example, for Paralympic athletes.
TTE
TTE is used to describe the standard of conventional cardiovascular measurements in elite athletes, including assessment of systolic and diastolic function of the left ventricle (LV) and right ventricle (RV), valvular function, cardiac and vascular dimensions and myocardial deformation. Images, measurements and quantification of the examination will be performed by accredited sonographers, assessed according to the echocardiography (and sports cardiology) guidelines of the European Society of Cardiology, and reviewed by a local expert (sports)cardiologist.15
CMR protocol and analysis
Each athlete will undergo CMR according to standardised protocol, preferentially on a 1.5 Tesla MRI scanner, with a dedicated body coil for cardiac measurements and ECG gating. The CMR protocol includes:1 cine imaging of long-axis views (two-chamber, three-chamber and four-chamber LV views) and short-axis from apex to atrioventricular junction,2 native and postcontrast T1 modified look locker inversion recovery sequence (MOLLI) mapping short-axis slices;3 LGE images (phase-sensitive inversion recovery sequence; PSIR) in two-chamber, three-chamber, four-chamber, and short-axis views;4 three-dimensional respiratory navigator gated ECG triggered whole-heart dataset in diastole (see online supplemental material for detailed CMR imaging protocol).
Supplemental material
CMR data analyses will be performed by a dedicated core-lab consisting of the ELITE investigators, expert radiologists and imaging cardiologists with extensive experience in the quantitative analyses of athlete CMR data. CMR analyses will primarily be performed in Circle Cardiovascular Imaging (cvi42, Calgary, Alberta, Canada), but other software packages may be applied, as appropriate. Contours will be automatically determined using an artificial intelligence integrated tool and manually corrected when needed. Maximal and minimal volumes of the left and right atrium will be derived from the two-chamber and four-chamber views by a (bi-) planar approach. Short-axis cine imaging will be used to determine LV and RV end-diastolic and end-systolic volumes and LV mass, using LV endocardial and epicardial contours and RV endocardial contours, by a summation of disks-approach and indexed for body surface area according to Mosteller. The presence of late gadolinium enhancement will be determined by using phase-sensitive inversion recovery images through visual identification and defined using a threshold of six standard deviations above normal myocardium signal intensity. T1 mapping measurements will be performed in all acquired slices (basal, mid-ventricular and apical). Native and postcontract T1 relaxation times will be calculated within a 15% margin of epicardial and endocardial contours. Extracellular volume will be determined using native and postcontrast T1 mapping and blood haematocrit, as previously described.16 T1 slices with poor quality (ie, due to movement or artefacts) will be excluded from analysis. T1 mapping times are reported as z-scores for the respective CMR imaging machines taking into account gender specific normative value (after establishment of normal values in a control population). Aortic dimensions will be measured, and the origin and course of coronary arteries will be determined using three-dimensional whole heart imaging.
Laboratory assessment
Blood collection for the laboratory assessment preferentially coincides with the CMR examinations. Blood will be collected through the intravenous system, before contrast administration. If unsuccessful or when blood collection is done separately from the CMR, blood will be drawn from an antecubital vein by venepuncture. Samples will be processed at the laboratories of general clinical chemistry of respective study sites according to their standard assay procedures, to define cardiac biomarkers, kidney function, inflammation and cholesterol levels.
Biobank
In addition to the standard laboratory assessment, blood samples will be collected and stored at the Amsterdam UMC Biobank for genetic analyses, which primarily focus on performance and cardiomyopathy and ion-channel associated genes.17
Follow-up measurements
Follow-up measurements will take place according to age and potential findings of the participating athlete (table 1).
Follow-up measurements of ELITE
COMMIT subcohort
After the advent of the new coronavirus, a subcohort of ELITE was established to investigate cardiac sequelae following SARS-CoV-2 infection. In short, ELITE – COMMIT (COVID-19 Myocardial Manifestations in Intensive Top-level sports and exercise) aims to prospectively investigate the long-term cardiac outcomes of SARS-CoV-2 infection and related cardiac sequalae. The objective of COMMIT is to investigate immunological patterns, myocardial involvement prevalence and clinical consequences including postinflammatory (SARS-CoV-2) cardiac sequelae. COMMIT has been approved by the Amsterdam University Medical Centers Medical Ethics Review Committee (NL71682.018.19), and additional consent will be asked for this study.
Proven SARS-CoV-2 infection is defined according to a positive PCR, or antibody test (before vaccination), or in the presence of typical COVID-19 symptoms for infected individuals in the time-frame before testing for SARS-CoV-2 became commonly available. Athletes with a novel, primary SARS-CoV-2 infection are offered to undergo voluntary SMART preparticipation protocol screening, excluding the CPET examination. Additionally, blood samples will be obtained for SARS-CoV-2-immunological testing, and serum will be separated and stored for future research related to SARS-CoV-2 and exercise-induced cardiac remodelling. Athletes showing perimyocardial involvement after SARS-CoV-2 infection will be referred for clinical monitoring, including intensive (24 hours to 4–8 days) rhythm monitoring (Holter and Philips biosensor) and repeat CMRs, according to current insights and guidelines.
Data analysis plan
ELITE is a prospective observational study, hence analyses will be primarily explorative. Quantitative data will be analysed using R (V.4.1.2 or higher).18 Descriptive analyses will be performed to summarise incidence and prevalence for outcome variables of interest stratified by gender, age, type of sports, training volume and other groups of interest. Normality of continuous variables will be assessed by histogram, QQ-plot and by use of the Shapiro-Wilk test. Normally distributed data will be presented as means and SD; non-normally distributed data will be reported as medians with IQRs. Categorical variables (including family history, type of sports and genetics) will be presented as numbers and percentages. Regression analyses will be performed, linear for continuous outcomes and logistic for categorical outcomes. Multivariate regression analyses will be performed to correct for possible confounders, and potential confounders will be added to the regression models to observe whether the associations change considerably. Effect modification will be tested by adding interaction terms to the regression model and, if present (ie, with a statistically significant interaction term), will be shown by stratified presentation of the results.
Discussion
ELITE is a prospective cohort study and aims to identify changes in cardiac indices over time in elite athletes engaging in various types of extreme-level sports. The primary objective of ELITE is to identify the effect and variance of various types of elite sports and exercise on exercise-induced cardiac remodelling, cardiac pathology and health benefits over time in elite athletes. Secondary objectives include genetic profiling of elite athletes and determining how these genetic variations are associated with cardiac indices and performance in various types of elite sports, next to postinfectious (eg, SARS-CoV-2) immunological patterns, prevalence of myocardial involvement and potential clinical consequences hereof. As such, ELITE constitutes a unique initiative to establish extreme phenotypes and the cardiac limits of sports.
The grey zone between adaptation to sports and cardiac pathology, and even more complex, the effects on sports when cardiac pathology is present, constitute central challenges for clinicians and other involved healthcare professionals. Establishing the limits of cardiac physiology and adaptation are mandatory steps in generating an evidence-based context for both differentiation between adaptation and pathology and to provide patients and athletes with personalised sports advice.1 19 ELITE will be the first study to prospectively investigate the limits of extreme phenotypes and cardiac physiology and adaptation in a large sample of exclusively elite athletes participating in highly variable sports disciplines. This is of particular importance, as elite athletes dictate the upper limits of normal for central parameters such as biventricular volumes, function and other morphological features. Prospective and ongoing evaluation is mandated, as athletes continue to push the boundaries of performance, as seen by numerous new world-records each year. Extreme achievements account for demands on cardiac physiology which have not earlier been documented, and understanding the cardiac consequences hereof will be of importance for the professional athlete and for the large group of recreational athletes and individuals who wish to engage in (high intensity) sports.
Different athletic disciplines demonstrate sport-specific variations of static and dynamic stress components, which contribute to different phenotypes of exercise-induced cardiac remodelling. Although varying theoretical frameworks have been developed to explain these changes,1 20 to date a comprehensive, data-driven framework based on comprehensive phenotyping, including CMR data, in elite athletes has not yet been established. ELITE constitutes a first step towards establishing such a data-driven framework, which will help clinicians improve risk stratification, provide insights into sports in the presence of myocardial diseases and determine reference levels for sports-specific cardiac remodelling. Additionally, comparisons with historical cohorts of patients with cardiac pathology such as cardiomyopathies or myocarditis will serve as a fundamental backbone to analyse the association between specific sports and cardiac (mal)adaptation, with current state-of-the-arts diagnostic modalities.
ELITE will collect data for cardiogenetic analyses. Genetic causes that underlie cardiomyopathies and ion-channel diseases are currently being investigated across multiple fields of cardiology and is of particular interest in sports cardiology, as genetic causes potentially account for ~25% of sudden cardiac death in young athletes.1 Traditionally, the presence of a pathogenic variants has been considered a contraindication to competitive sports, but recent guidelines have adopted a more liberal and risk-based approach.1 However, with the use of widespread (commercial) genetic testing, new challenges are imminent, as the prevalence of variants in disease-associated genes has not been determined in (elite) asymptomatic athletes. Additionally, the effects of exercise on cardiac remodelling in athletes with said genetic variants are unknown, with the exemption of some variants associated with arrhythmogenic cardiomyopathies, such as PKP2, where exercise has been associated with a worse prognosis.5 6 Finally, and controversially, we have previously reported that some specific variants in genes associated with cardiomyopathies could have a beneficial effect on physical performance.21 Therefore, ELITE and the ELITE biobank can provide new insights into the complex interplay between genetic variants in athletes performing at the highest level of sports and cardiovascular disease, with as final aim to prevent potential unnecessary cessation of sports careers in athletes with benign variants or variants with no detrimental effects through sports, and to improve the detection of athletes at risk for developing cardiovascular pathology.
Strengths and limitations
There are several strengths to our study. First, ELITE is a multicentre prospective cohort study, investigating cardiac indices over time in elite athletes participating in all types of sports, including young athletes and athletes that eventually retire from their sports careers. Currently, most studies investigating cardiac sequelae in athletes have been cross-sectional, and little is known about the potential reversibility of exercise-induced cardiac remodelling after sports career cessation, and potential interactions with conventional risk factors developed later in life. Second, our study includes comprehensive cardiovascular screening examinations over time, including ECG, CPET, blood measurements, TTE and routine CMR. We are the first to introduce such an in-depth standardised screening in a large group of elite athletes—athletes with abnormal findings in conventional preparticipation screenings, which will provide the opportunity to assess what the added diagnostic value is of individual diagnostic modalities to standard preparticipation screenings. Finally, the ELITE biobank will provide insights into genetic profiles of elite athletes.
Some aspects of our study warrant consideration. First, ELITE includes athletes who play and train for Dutch teams, which potentially can result in a lack of racial and genetic diversity. However, to prevent this, we explicitly include elite athletes of non-Dutch origin playing for teams originating in The Netherlands. Second, examinations included in ELITE will have some heterogeneity. Different vendors for diagnostic modalities (eg, TTE and CMR) and software can lead to subtle differences in values of, for example, 2D-strain and parametric mapping. We aim to ameliorate these potential differences through core-lab analysis and rigorous collection of scanner-specific normal values. Finally, the ELITE biobank could potentially lack power to detect rare genetic variants or polygenetic combinations. However, due to the comprehensive phenotyping and uniform data collection, collaborations with comparable initiatives are possible to increase the sample size.22
Conclusion
The ELITE prospective, multicentre longitudinal cohort study will investigate sports-specific, extreme cardiac phenotypes and genotypes in a large group of elite athletes. ELITE will provide insights into the longitudinal cardiac effects of extreme levels sports and exercise, cardiovascular adaptations and the development of cardiac pathology over time during and after the cessation of a sports career. Furthermore, ELITE will provide novel insights into the genetic background of elite athletes and the complex interplay between genetic variability and cardiac indices. Finally, ELITE will provide normative values of limits of healthy adaptation to sports, that is, extreme phenotyping, which will facilitate our understanding of pathology and health and assist in the differentiation between sports-specific cardiovascular adaptation and pathology for elite athletes, and for recreational athletes and patients who wish to engage in sports and exercise.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Amsterdam University Medical Centers Medical Ethics Review Committee (NL71682.018.19). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JCvH and SMV are joint first authors.
Collaborators ELITE Consortium: RD van Luijk-Snoeks, AM van den Berg-Faay, M van Eerden, JC van Hattum, SM Verwijs, SM Boekholdt, M Groenink, RN Planken, A van Randen, AJ Nederveen, MH Moen, CACM Wijne, JJN Daems, BK Velthuis, DAJP van de Sande, R Spee, ST de Vries, MJ van der Veen, YM Pinto, AAM Wilde, HT Jørstad.
Contributors All authors have been substantially involved in the preparation of this manuscript and are in agreement with the contents of this paper. In addition, to the best of our knowledge, there are no financial or other conflicts of interest for any of the named authors.
Funding Harald T Jørstad has received funding for ELITE from Amsterdam Movement Sciences (P1A210AMC2018) and NOC*NSF, and for COMMIT from the Netherlands Heart Foundation (01-001-2020-T079).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.