Article Text

Abstract
Objectives To evaluate the difference between healthcare professionals (HCPs) and adults with spinal cord injury (SCI) in Asia regarding knowledge and interpretation of ‘exercise intensity’ for aerobic exercise prescription.
Methods and study design A survey was distributed to practising HCP and adults with SCI. It was completed in participants’ local language on topics related to the importance of exercise frequency, intensity, time and type; methods for monitoring and terms related to exercise intensity prescription. χ2 analysis was used to detect differences in HCP or those with SCI.
Results 121 HCP and 107 adults with an SCI ≥1 years (C1–L4) participated. Responses revealed 61% of all HCP ranked ‘intensity’ being most important whereas only 38% respondents from the SCI group ranked it as high importance (p=0.008). For those with SCI, ‘frequency’ was most important (61%) which was significantly higher than the 45% selected by HCPs (p=0.030). Of the 228 respondents on average only 34% believed that the terms, ‘moderate’ and ‘vigorous’ provided enough information for aerobic exercise intensity prescription. HCP most often used HR methods compared with the SCI group (90% vs 54%; p<0.01). Both groups frequently used the subjective measures of exercise intensity, for example, Ratings of Perceived Exertion (8%3 vs 76% for HCP and SCI), HCP also frequently used speed (81%) and SCI also frequently relied on ‘the affect’ or feelings while exercising (69%).
Conclusions These differences must be considered when developing clinical-practice exercise guidelines and health referral educational pathways for adults with SCI in Asia.
- exercise rehabilitation
- wheelchair
- exercise testing
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Many methods exist for prescribing/monitoring exercise intensity, however, the knowledge and practical use of these in different user groups has not been investigated.
WHAT THIS STUDY ADDS
Heathcare professionals (HCPs) ranked ‘intensity’ as their most important concept of the frequency, intensity, time and type principle, with the adults with lived spinal cord injury (SCI) highlighting ‘frequency’ as their most important concept.
The terms ‘moderate’ and ‘vigorous’ do not provide sufficient information for prescribing suitable exercise intensity for adults with SCI from Asian nations.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Given the dissonance in views, future work should explore how HCP can support the patient with SCI during rehabilitation so that when they move to the community, they can monitor their exercise intensity independently to achieve an effective exercise stimulus.
Introduction
It is widely accepted that maintaining a physically active lifestyle through participation in exercise for adults living with a spinal cord injury (SCI) should be encouraged.1–3 Health benefits include a lower risk of hypertension, diabetes, obesity, cardiovascular disease and consequently improvements in functional independence, social reintegration and psychological well-being are noted.4 5 Having clear guidance that describes the dose of exercise that is required for improving cardiorespiratory fitness and cardiometabolic health in adults with SCI,3 6 plays a pivotal role for healthcare professionals (HCPs). The composition of this HCP team during the rehabilitation phase within SCI services typically includes physiotherapists, occupational therapists, dieticians, social workers, clinical psychologists, nurses and doctors.
There has been a recent interest in the translation and evaluation of the international exercise guidelines for adults with SCI6 to better support the SCI community with aerobic fitness and strength training guidance to facilitate maximum independence. A recent 6-week exercise rowing (arms-only) intervention undertaken by Hasnan et al7 demonstrated that following the exercise guidelines was deemed an acceptable and feasible method for adults with SCI. Moreover, a mobile App (WHEELS) has also incorporated these bespoke SCI exercise prescription guidelines to target behaviour change to overcome additional social barriers using mobile health technologies.8 While encouraging, that the 2018 international guidelines are now in use in Europe and in Canada for studies aimed to understand neuropathic pain,9 they have been updated to include published studies from Asia to obtain greater global reach.10
Fundamental to the scientific guidelines is the prescription of exercise intensity using the terms ‘moderate to vigorous’, as intensity serves as a key stimulus for beneficial health and fitness adaptations.11 Within the exercise guidelines for non-disabled adults these intensities are clearly defined according to various measures (eg, % heart rate reserve), % heart rate (HR) max, % aerobic capacity, ratings of perceived exertion (RPE) and maximum exercise capacity using the metabolic equivalent of task).11 It has repeatedly been shown that working at a vigorous exercise intensity training leads to greater physiological adaptation than moderate intensity training,12–14 even when the total training volume is significantly reduced.15 Performing vigorous, rather than moderate, intensity exercise has also been shown to associate with lower risk of all-cause mortality.16 17 However, there is limited evidence regarding how to appropriately describe, set and guide exercise intensity thresholds for adults with SCI,18 and the terms ‘moderate to vigorous’ remain commonplace within SCI rehabilitation exercise interventions.2 19 20
Given the large number of adults with SCI affected by an array of cardiometabolic complications, with obesity being the most common,3 21 it is important that health referral pathways of supporting effective exercise programmes are encouraged. While Hoekstra et al22 have used community-engaged methods to translate the physical activity guidelines for use within Canada, we must step back to consider how different end-users (eg, HCP vs adults living with SCI) interpret the exercise intensity portion of such guidelines. Furthermore, any future translations should consider what information is needed to ensure that the prescribed exercise is of a sufficient intensity to lead to beneficial fitness and health adaptations. As such, the aim of this investigation was to evaluate the difference between HCP and adults living with SCI in Asia regarding knowledge and interpretation of ‘exercise intensity’ for exercise prescription.
Methods
Participants: A cross-sectional study was performed by means of paper survey that was anonymously distributed to (1) practising HCP in Asia specialising in SCI healthcare and (2) adults living with SCI in Asia (≥18 years old with traumatic or non-traumatic SCI, 1-year postinjury). It was completed in participants’ local language (Indonesian, Korean, Japanese and Thai). The procedures followed were in accordance with the ethical standards of the responsible committees on human experimental and with the Declaration of Helsinki in 2008, and informed consent was provided prior to completion of the questionnaire. Recruitment occurred between March and May 2021, using convenience sampling as most respondents were in or outpatients at each hospital and rehabilitation centres in participating countries. Individual hospitals approached their community-based organisations to recruit. The surveys were distributed by a direct hand-over to a respondent, an email to the selected subjects. We took a focus in Asia due to the timing of the survey, to align with the legacy of the Paralympic Games hosted in Tokyo 2021, where full consideration of the needs and interests of people with a disability was growing through awareness-raising activities.
Survey instrument and survey procedure: A self-designed questionnaire was developed collaboratively by the authorship team. It was initially drafted by specialists in exercise physiology (MH and VT) before all other authors commented and approved the final survey, based on their clinical expertise in SCI rehabilitation, and qualitative research methods. The questionnaire was tested for usability in a representative sample (n=4) comprising a medical doctor, physiotherapist, exercise scientist and an adult living with an SCI. It involved completing a single questionnaire with multiple-choice questions using a 5-point Likert scale. The questionnaire was designed in English but then translated into the local language. This involved forward translation into Bahasa Indonesian, Japanese, Korean and Thai languages. The Indonesian translation was completed by an English teacher and the other three translations were completed by physiatrists. The survey was then back-translated to English by another physiatrist (Indonesian, Thai) or a translator (Japanese, Korean) for data input and analysis. The final English-language version of the questionnaire can be found in online supplemental material.
Supplemental material
Supplemental material
Topics covered in the questionnaire included: the perceived importance of exercise frequency, intensity, time and type (FITT) principle; the terms ‘moderate’ and ‘vigorous’ in relation to aerobic exercise intensity prescription and cues associated with exercise intensity. The questionnaire also captured data pertaining to individual characteristics (eg, age, occupation, impairment) and took up to 40 min to complete.
Statistical analysis
The Statistical Package for the Social Sciences V.26 software (SPSS) was used to analyse the data. Data were evaluated by HCP and adults with SCI using χ2 analyses. For each question, percentages were calculated for responses to each question. Where appropriate, data were subsequently interpreted using ORs. Significance was determined at p<0.05.
Results
Demographics: A total of 228 responses were received (range 20–74 years, table 1). This sample was further divided into two categories (certified HCP (n=121; mean age 39±1 years) and adults with lived SCI ≥1 year ranging C1–L4 (n=107; mean age 46±13 years)). Participants were recruited from Indonesia, Japan, Korea and Thailand with HCP reportedly an average of 12±10 years’ experience and the adults with lived SCI an average of 15±12 years post onset of SCI. Physiotherapists accounted for the largest portion of the HCP respondents with 49% along with 30% of medical doctor, 18% of occupational therapist and 3% of nurse involved in rehabilitative treatments. Fifty-four of the adults with SCI were injured in the thoracic region, 31 the cervical, 15 the lumbar with 7 unable to recall the level of SCI. There were 46 responders with a complete (43%) and incomplete SCI (n=56, 52%) with n=5 unable to recall the severity of the SCI.
Participant characteristics (mean±SD (range))
The FITT principle and appropriateness of the exercise prescription terms, ‘moderate’ and ‘vigorous’
The four aspects of the FITT principle were ranked by HCP and adults with SCI for aerobic exercise (table 2). Sixty-one per cent of all HCP ranked ‘intensity’ with greatest importance (rank 1+rank 2) which was significantly higher than the 38% respondents from the SCI group (p=0.008). A different pattern emerged for the adults with SCI where 64% of all respondents ranked ‘frequency’ with greatest importance (rank 1+rank 2), which was significantly higher than the 45% selected by HCP (p=0.030).
Ranking of the four aspects in order of importance when conducting aerobic exercise in the four Asian nations (count (per cent %))
When asked whether ‘moderate’ or ‘vigorous’ exercise intensity terms were suitable for exercise prescription, the HCP and adults with SCI did not differ significantly with their views. Of the 228 respondents on average only 34% believed that the terms, ‘moderate’ and ‘vigorous’ provided enough information for aerobic exercise intensity prescription.
Methods for monitoring exercise intensity
When asked how important do you think each of the methods are for prescribing aerobic exercise intensity, HCP chose objective measures, such as HR (89%) and/or oxygen uptake (78%), as their two most important ranked methods. RPE (ie, a subjective measure) was considered the third most important (66%) by the HCP. Figure 1 indicates the methods and importance of use for the HCP and SCI. There were no significant differences between groups, but most of the adults with SCI reported equal weighting to the importance of HR (57%), oxygen uptake (57%), power output (57%), speed (52%), feeling scale (55%) and RPE (54%) for prescribing exercise intensity. After completion of the survey, it was noted that the term ‘moderately’ was considered a neutral term and so the importance was taken from the ‘very-extremely’ responses.
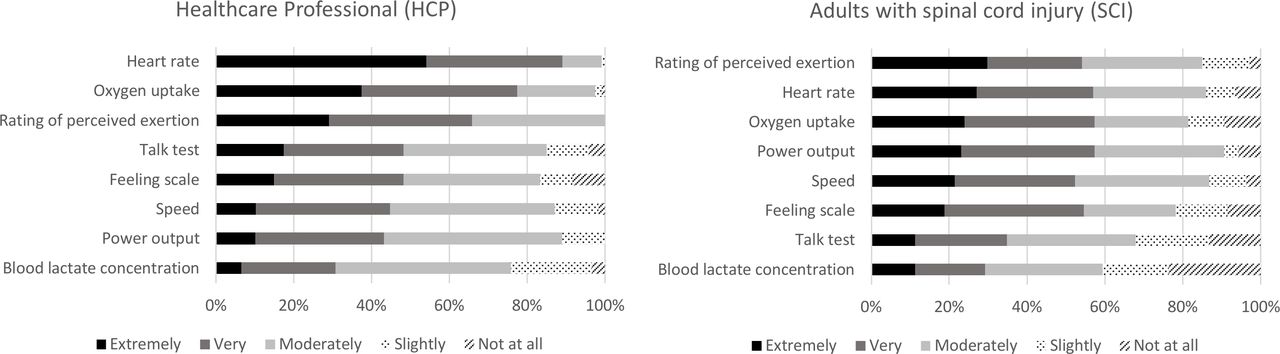
Respondent’s (HCP and SCI) categorisation to the question ‘How IMPORTANT do you think each of these measures are for prescribing AEROBIC exercise intensity’. Note: Participants were only able to select one response per exercise prescription method, and the phrase moderately was deemed a ‘neutral’ reply in the Asian to UK translation.
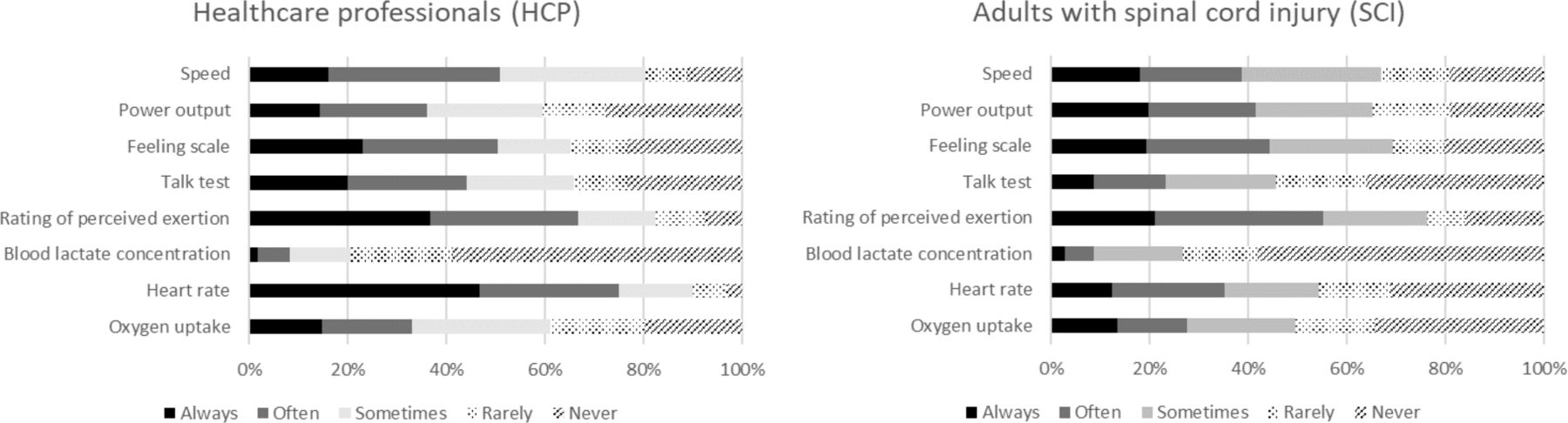
In total, 108 HCP and 57 adults with SCI frequently used HR methods across the categories of ‘sometimes to always’, for their exercise prescription (figure 2). The HCP most often used HR methods than the SCI group (90% vs 54%; p<0.01) for exercise prescription. Both groups frequently used the subjective measures of exercise intensity such as RPE (83% vs 76% for HCP and SCI), while the HCP also frequently used speed (81%) and SCI also frequently relied on ‘the affect’ how they felt while exercising (69%).

{kind=link}
{kind=link}
Respondent’s (HCP and SCI) categorisation to the question ‘How FREQUENTLY do you use each of these measures for prescribing AEROBIC exercise intensity’. Note: Participants were only able to select one response per exercise prescription method. Only significant difference was noted in the frequency of heart rate use (p<0.01) between groups.
Discussion
To our knowledge, this is the first study that has aimed to understand end-user perceptions (HCP and adults with SCI) of exercise intensity, to be able to inform guidelines for prescribing exercise in adults with SCI. The main findings were that certified HCP ranked ‘intensity’ as the key element of the FITT principle with the SCI group highlighting ‘frequency’ as their most important concept. Only 34% of all respondents believed that the terms, ‘moderate’ and ‘vigorous’ provided enough information for prescribing aerobic exercise intensity.
The present data showed HCP realise that ‘intensity’ for adults with an SCI is of great importance supporting the current non-disabled literature.14–17 Regardless of the ambulatory methods of adults with an SCI (eg, walking or wheeling), many exercise options are limited to the upper body involving small active muscle mass. The shift in prescribing vigorous-intensity exercise is most likely driven by not only the rise in levels of obesity,21 its increased media attention,23 but also the current debate that centres on whether moderate to vigorous is sufficient to induce meaningful improvements in risk factors for the prevention of cardiometabolic disease in adults with an SCI.24–26 Leicht et al24 stated that relative exercise intensity appears to be more important to the acute inflammatory response than modality, which is of major relevance for populations restricted to upper body exercise. We hypothesise that the dissonance in views, with the SCI group reporting that ‘frequency’ was most important (ie, more the better), showed a lack of knowledge and understanding of the physiological consequences of SCI and the lack of understanding of what intensity is. We obviously do not wish to discourage exercise, but this does add to the ongoing debate of what information adults with SCI need to be provided when moving from hospitalised rehabilitation to the community. We may have been less surprised if the SCI group had chosen exercise modality as their key FITT component as it is evident that higher HR are often achieved through functional electrical stimulation hybrid exercise7 27 than arm cranking or wheeling alone. This highlights the long-term challenges faced by HCP to translate evidence-based practice into improving patient knowledge about health and exercise as they are discharged into the community.
While HCPs in Asia may understand the importance of physical activity/exercise counselling, the implication of these findings is that exercise guidelines cannot simply use the terms ‘moderate to vigorous’ within guideline descriptors. This study highlighted some important differences between HCP and adults with SCI, in terms of the methods/cues used for monitoring exercise intensity. The results are perhaps not surprising when considering the end-user groups involved. For example, HCP are typically working in a hospital or rehabilitation centre where they are likely to have equipment and tools at their disposal for making physiological measurements (eg, oxygen uptake). Adults with SCI, on the other hand, are unlikely to use such measures due to the cost of equipment and the specialist technical expertise required to operate the equipment and interpret or understand the data. That said, the findings revealed greater uptake in the use of RPE with agreement that this was a preferred option. Indeed, the use of RPE offers an accessible form of exercise prescription as it is simple to understand, inexpensive and easy to implement11 and the Borg (6–20 scale) has been shown to be reliable depending on the participants’ fitness level as well as the exercise modality used.19 In non-disabled individuals, HR is a common method to gauge the intensity of aerobic exercise, so it was not surprising to see this option being important to the SCI group. That said, we were surprised to see this method chosen by the HCP as for those with a high-level SCI (above the sixth thoracic vertebrae (T6)), impaired sympathetic innervation of the heart28 reduces the validity of HR as a method of exercise intensity regulation in this population.19
Clinical implications
This study offers an important foundation for development of clinical practice guidelines for adults with an SCI, by highlighting differences between the end-user groups in Asia. Initiatives such as a health referral pathway around the ‘messaging’ of exercise intensity would have to be tailored to the needs and preferences of the specific end-user to facilitate appropriate exercise intensity prescription. For example, HCP needs to understand that once the patient with SCI is discharged from hospital, that they need to understand and have confidence with how they can monitor their exercise intensity independently. That said, to achieve an effective exercise stimulus, the term ‘intensity’ is operationally more difficult to define compared with frequency and duration. Hence, further work is warranted to explore how exercise intensity can be best described to ensure uniform exercise intensity prescription between individuals.
Strengths and limitations
Strengths of this study were that it is the first of its kind to assess and compare views of a large number of HCP and adults with an SCI that had ≥1 years of lived experiences and the HCP represented a wide number of clinical SCI rehabilitation roles in Asia. Only a few participants failed to complete all questions and it is important to note, the survey was limited to multiple-choice questions with responses given on a 5-point Likert scale because of the COVID-19 pandemic to allow responses to be completed in less than 1 hour. It may have been more suitable to include some more open-ended questions to gain a more detailed insight on some of the specific areas, yet we sought to keep the survey short and simple for the busy clinical staff at the time of a global health pandemic. It is also not known how transferable these findings are to other countries since in Asia the exercise professionals are not independent and medical doctors may dictate what is performed in a rehabilitation context. Therefore, due to cultural and contextual differences, future work is warranted to explore if these findings exist in European of North America countries.
Conclusions
Differences existed between HCP and adults with SCI with their understanding and interpretation of monitoring exercise intensity. Our findings highlight a long-term challenge with the development of exercise guidelines as adults with SCI were less familiar with the importance of exercise intensity, and the fact that only 34% of our total sample felt the terms ‘moderate’ and ‘vigorous’ provide enough information for exercise prescription. That said, a revelation of this study was the knowledge and usage of RPE by both HCP and adults with SCI which is a simple tool to use. Future research should focus on educational strategies to ensure that adults with an SCI receive appropriate support to avoid any misunderstanding of how to best prescribe aerobic exercise in the community.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The Ethics Committee of Loughborough University (UK) #2021-3242-2831; Universitas Airlangga (Indonesia) #1408/KEPK/VIII/2019, Wakayama Medical University (Japan) #3109, Ajou University (Korea) #AJOUIRB-SUR-2021-051 and Mahidol University (Thailand) #093/2021.
Acknowledgments
The authors would like to thank the participants for their time taking part in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KSJ, MH, FT, VT and YM conceived and designed the project and played an important role in interpreting the results. CC, MKK, S-HY, PL, DT, PP, PC, IN, DAU and YU acquired data and participated in meetings to discuss the findings. KSJ, MH and VT participated in meetings to discuss the findings, support was provided at Loughborough University (Dr Claire Madigan) for the statistical analysis. KSJ, CC, MKK, S-HY and YM worked on the language translation. KSJ, MH and VT wrote the first draft of the manuscript. VT is the guarantor of the study. All authors helped to draft or revise sections of the manuscript for important intellectual content, approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Funding Funding for this project was provided by Joint Usage/Research Center of Sport for Persons with Impairments authorised by the Ministry of Education, Culture, Sports, Science and Technology, Wakayama Medical University, Japan (grant number SP2020-01) and a funding from the Peter Harrison Foundation which supports the operations of the Peter Harrison Centre for Disability Sport, Loughborough University, UK.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.