Article Text

Abstract
Objectives High-intensity interval training (HIIT) during pulmonary rehabilitation in patients with chronic obstructive pulmonary disease (COPD) may alleviate the symptom burden, but the fidelity and tolerability of HIIT using long or short intervals in patients with COPD are unknown.
Methods Twelve patients with moderate-to-severe COPD were included in a randomised cross-over pilot study. They completed two supervised HIIT protocols (4×4 and 10×1). To compare the two HIIT protocols, completed training amount, exercise intensity and perceived tolerability (assessed by a 10-point Likert scale) were integrated in a red–amber–green rating system. If a training session received a red ranking, it was considered unacceptable, if it received an amber ranking it was applicable with precautions, and if it received a green ranking it was considered feasible.
Results All patients completed the total training amount in both protocols. The 4×4 protocol resulted in three amber training sessions due to low perceived tolerability. The 10×1 protocol resulted in two red training sessions due to intensity reductions, and two amber training sessions because of low perceived tolerability. There was no statistical difference in perceived tolerability or time spent with an HR ≥85% of HRmax.
Conclusions HIIT using longer intervals (4×4) at a relatively lower intensity resulted in higher fidelity expressed by fewer adjustments to the protocol, whereas there was no difference between protocols in perceived tolerance. The 4×4 protocol seems to have a higher fidelity compared with the 10×1 protocol in patients with moderate-to-severe COPD.
Trial registration number NCT05273684.
- Training
- Exercise rehabilitation
- Lungs
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
High-intensity interval training (HIIT) is recommended as a training regimen for pulmonary rehabilitation in patients with chronic obstructive pulmonary disease (COPD).
Many different protocols with differing intensities, number of intervals and work-to-rest ratios are currently used in COPD, but the fidelity and tolerability of these schemes has not previously been compared.
WHAT THIS STUDY ADDS
A single HIIT session using long (4×4 HIIT) intervals at a relatively lower intensity has a higher fidelity than short (10×1 HIIT) intervals at a very high intensity in patients with moderate-to-severe COPD, while the two protocols appear to be similarly tolerated.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
In rehabilitation programmes and future clinical trials in patients with COPD, 4×4 HIIT protocols at a relatively lower intensity may lead to higher patient adherence and thus potentially greater clinical efficacy than 10×1 HIIT at a very high intensity.
Introduction
Exercise intolerance is a main disabling factor for many patients with chronic obstructive pulmonary disease (COPD).1 The cause of exercise intolerance is multifactorial, and encompasses both pulmonary, cardiovascular and skeletal muscle dysfunction.2–5 Pulmonary rehabilitation (PR) is an important aspect of COPD management, with exercise training considered the most effective non-pharmacological component.1 Evidence shows that exercise training increases exercise tolerance, reduces symptom burden and improves quality of life, while also potentially reducing mortality, when supervised.6 7 However, when implemented as a part of PR, the optimal training modality to exert a clinically meaningful reduction in symptom burden remains to be determined.6 8 9
The rationale of using interval-based training in COPD has mainly been that working skeletal muscle can overcome intervals of high intensities without overloading the cardiorespiratory system,10 that is, aggravation of air flow limitations and potentially hyperinflation.11 Recently, a meta-analysis found that high-intensity interval training (HIIT) increased exercise capacity, forced expiratory volume in 1 s (FEV1) and quality of life in patients with COPD.12 It has been argued that even though interval-based training may increase symptoms of dyspnoea during exercise, it may be better tolerated than continuous training, because the periods of rest between intervals allow the patient to reverse dynamic hyperinflation.13 The work-to-rest ratio might be an important factor when designing the optimal HIIT protocol, to avoid aggravation of dynamic hyperinflation and enabling the beneficial effect of prolonging the exercise endurance time.13
Despite the beneficial clinical effects of HIIT in COPD, there is still no consensus regarding the length of intervals, intensities or work-to-rest ratios.6 Currently, a wide range of intervals durations are used, most frequently <2 min with intensities commonly related to the maximal workload (Wmax) and ranging from 90% to 140% of Wmax.12 Another factor that may affect patient adherence to a HIIT protocol is the intensity during intervals.14 However, no studies in patients with COPD have yet investigated whether the fidelity and tolerability differs between a HIIT protocol with short intervals at a very high intensity compared with a slightly lower intensity with longer intervals.
An increasing number of studies conducted in different patient populations including patients with COPD have shown improved exercise capacity after HIIT, using a protocol with interval durations >2 min with intensity quantified as a percentage of maximal heart rate (HR).15 16 Still, it remains to be determined whether HIIT using intervals of short duration is better tolerated and exhibits greater fidelity, that is, if patients adhere better, than HIIT based on longer intervals.
In the present randomised cross-over pilot study, we therefore, investigated the fidelity and tolerability of two commonly used HIIT protocols, which have both previously been shown to induce clinically meaningful improvements in exercise capacity in patients with moderate-to-severe COPD.15 17 We hypothesised that HIIT with short intervals (1 min) at a very high intensity would be better tolerated compared with longer intervals (4 min) at a relatively lower intensity, when implementing breaks of identical durations between intervals.
Methods
Study design, participants and randomisation
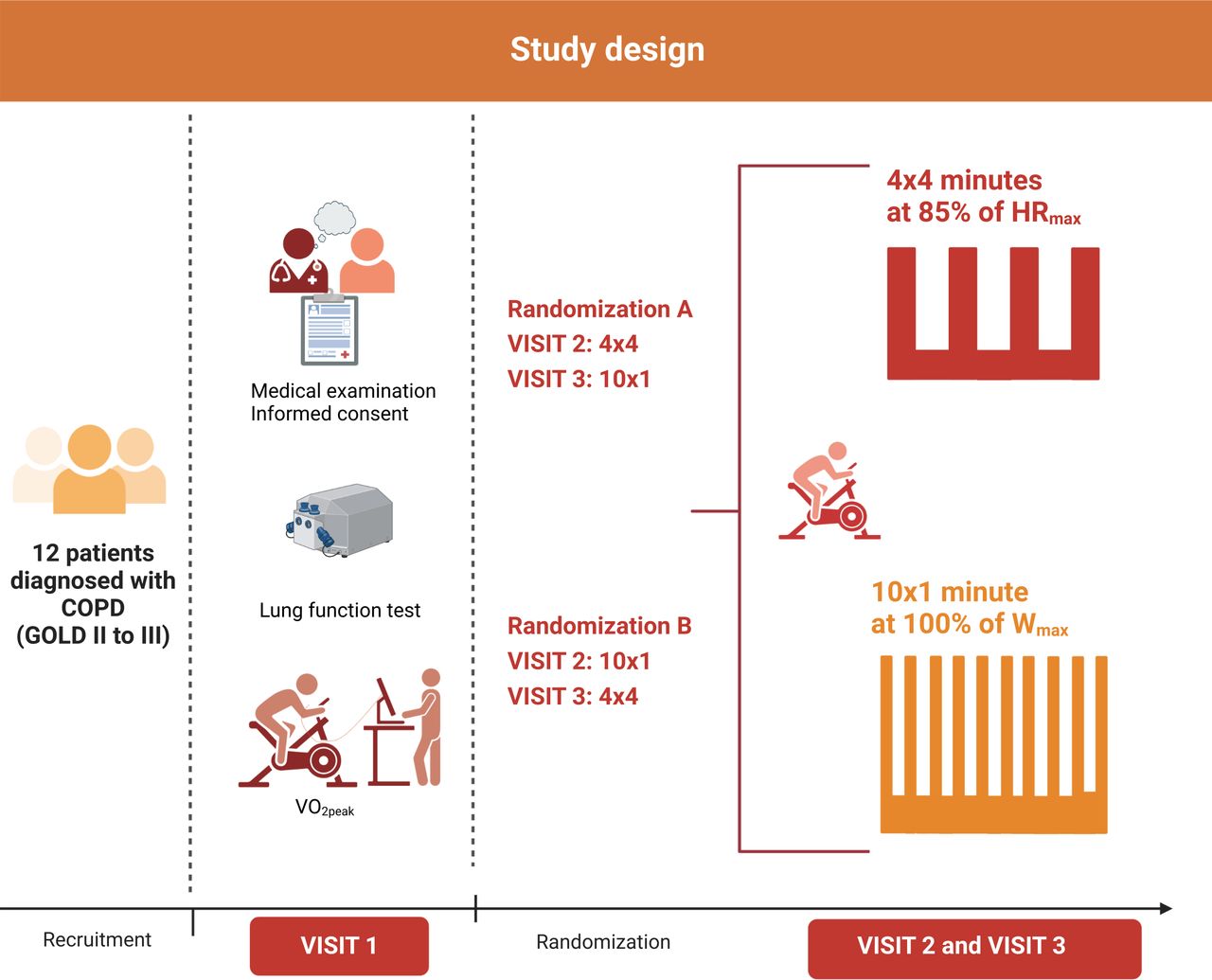
The design of the present pilot study is outlined in figure 1. Twelve patients diagnosed with moderate-to-severe COPD (Global Initiative for Obstructive Lung Diseases, GOLD II and III) were included from December 2021 to July 2022. A sample size of 12 was pragmatically chosen based on previous recommendations for pilot and feasibility studies.18

Overview of the study design. The patients completed two different HIIT protocols in a randomised cross-over design. Both protocols were initiated by a 10 min warm up at 30% of Wmax. Created using BioRender. COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Obstructive Lung Diseases; HIIT, high-intensity interval training; HR, heart rate; V̇O2peak, peak oxygen consumption; Wmax, maximal workload.
All patients were clinically stable and recruited from the primary healthcare sector and through advertisements. The inclusion criteria were moderate-to-severe COPD (GOLD II and III), age ≥18 but ≤80 years. Exclusion criteria were any known heart diseases, known vascular ischaemic disease, severe neurological disease, pregnancy, or symptoms of disease within 2 weeks prior to the study.
A general medical examination (including blood pressure and ECG) and standard lung function testing were conducted prior to inclusion. Lung function testing encompassed dynamic spirometry, whole-body plethysmography and single-breath carbon monoxide uptake measurements, which were performed in accordance with consensus guidelines,19–21 to obtain FEV1, forced vital capacity, total lung capacity, residual volume and diffusing capacity for carbon monoxide corrected for haemoglobin (DLCOc). Based on summary equations,22 23 the expected values according to height, age and sex were calculated to determine each lung function metric as % of predicted.
If the patients fulfilled the inclusion criteria, a whole-body dual-energy X-ray absorptiometry scan and measurements of oxygen consumption (V̇O2) during a maximal incremental cardiopulmonary exercise test (CPET) were performed. V̇O2 was measured breath-by-breath using a Quark gas analyser (COSMED Quark CPET System, COSMED Srl, Rome, Italy). CPET was performed on a bicycle ergometer (E839, Monark Exercise AB, Vansbro, Sweden) with a 5 min warm-up at 15 watts, followed by a 10–15 watt increase every minute until exhaustion. The increase in workload was set on an individual basis aiming for the test to terminate after 8–12 min. HR was measured in beats per minute with a smartLAB HR chest band compatible with the COSMED system (smartLAB, Dossenheim, Germany). After baseline tests, the patients were randomised to a HIIT sequence, and in a randomised cross-over design they completed and evaluated the two HIIT protocols (figure 1).
HIIT protocols
The HIIT protocols were preceded by a 10 min warm-up at 30% of Wmax, followed by a block of intervals. The 4×4 HIIT protocol consisted of four intervals each lasting 4 min. The intervals were initiated at 70% of Wmax to reach the target intensity of ≥85% of HRmax. Each interval was separated by a 3 min active break at 30% of Wmax. The 10×1 HIIT protocol consisted of 10 intervals, each lasting 1 min at 100% of Wmax, separated by a 3 min active break at 30% of Wmax. The block of intervals had a duration of 28 and 40 min for the 4×4 and 10×1 HIIT protocol, respectively, and was followed by a cool down period. The total training duration was 42 min for the 4×4 protocol and 52 min for the 10×1 protocol. HR was recorded using a Polar heart rate monitor (Polar V800, Polar Electro Oy, Kempele, Finland) with a H7 chest belt. All exercise sessions were supervised, and patients were verbally motivated during the intervals.
Fidelity and tolerability measures
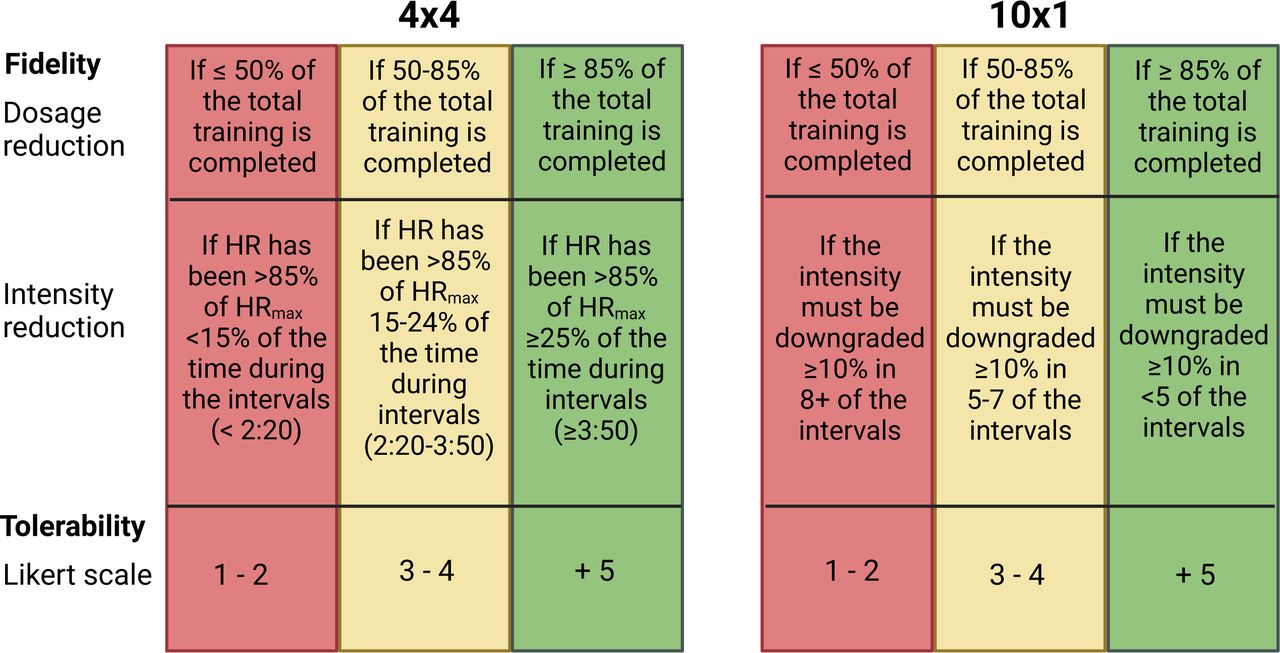
Fidelity was defined as adherence to the specific HIIT protocol and was evaluated by the need for either a reduction in training amount or intensity. In both HIIT protocols, the training amount was evaluated as the duration of the session completed, and intensity as the time spent with an HR≥85% of HRmax for the 4×4 HIIT protocol, and number of completed intervals at 100% of Wmax for the 10×1 protocol (figure 2).

Red–amber–green system. Red–amber–green system designed to evaluate the two HIIT protocols. Created using BioRender. HIIT, high-intensity interval training HRmax, maximal heart rate.
In the 4×4 HIIT protocol, the success criterion was to spend at least 25% of the intervals with an HR ≥85% of HRmax.24 The workload was increased by 10% if the HR was <85% of HRmax during the last minute of the 4 min interval, and likewise the workload was reduced if (A) rounds per minute (RPM) were <60 or (B) the HR exceeded 95% of HRmax.
In the 10×1 HIIT protocol, the success criteria were to complete a minimum of 8 intervals at 100% of Wmax. If the patients failed to keep the pace >60 RPM for more than 5 s, the workload was reduced by 10% from the next interval.25
At the end of each HIIT session, tolerability was evaluated by the patient’s subjective perception of tolerance using a 10-point Likert scale.26 Immediately after the HIIT session, the patient was asked to what degree he or she agreed with the following statement: ‘How tolerable was today’s training?’ with 10 indicating completely tolerable and 1 indicating not tolerable at all.
Red–amber–green system
To achieve a formal comparison of the two HIIT protocols that accounted for both fidelity and tolerability, we used a red–amber–green System (figure 2), based on a similar rating system used in a recent study.25 This was based on (1) the patients’ adherence to the protocol, which encompassed completed training volume and intensity as indices of fidelity and (2) a 10-point Likert Scale-based assessment of perceived tolerability.
The completed training volume was evaluated as minutes completed in percent of prescribed in both protocols. The completed intensity was evaluated as time spent with an HR ≥85% of HRmax for the 4×4 protocol, and number of completed intervals at 100% of Wmax for the 10×1 protocol (figure 2). The lowest fidelity or tolerability score determined the overall red–amber–green rank of the given HIIT protocol. If the training session achieved a red rank, the session was considered unacceptable, where an amber ranking was considered applicable with precautions. If the HIIT session achieved a green rank, the session was considered acceptable and feasible.25 27
Other outcome measures
To compare the two HIIT protocols further, we assessed intensity as the achieved intensity during each HIIT protocol as time spent with an HR ≥85% of HRmax and the relative intensity, as the completed workload in % of Wmax. Furthermore, the rate of perceived exertion (RPE) was evaluated by the 6–20 Borg scale immediately after each HIIT session28 and enjoyability was evaluated by a 10-point Likert scale. Immediately after the HIIT session, the patient was asked to which degree he or she agreed with the following statement: ‘How much did you enjoy today’s training?’ with 10 indicating very enjoyable and 1 indicating not enjoyable at all.
Blinding and allocation to sequence generation
The patients were allocated to a random sequence and completed and evaluated the two HIIT protocols as described above. Randomisation was performed by a researcher with no other relation to this study than to generate a block randomisation schedule with no stratifications. The sequence generation was performed at https://www.randomizer.org/ and kept in a locked drive and concealed from the investigators enrolling and assessing patients. The block size was not disclosed to ensure concealment. The patients were blinded to the randomisation until the beginning of the first HIIT session. To maintain blinding, the HIIT allocation was delivered by email to the investigators after completion of the baseline testing. The investigators informed the participants just before each training session on which HIIT protocol to perform.
Serious adverse events and adverse events
Serious adverse event (SAE) was reported if the patients experienced any serious adverse reactions or if any serious events occurred during the study. Given that there is consensus that HIIT is safe and currently recommended for PR in COPD,1 safety was not considered an a priori outcome in this study, and there was thus no predesigned protocol for collection of adverse events (AE) related to symptom burden of COPD. However, intolerable dyspnoea and verbal complaints of peripheral fatigue were noted, together with any deviations from the prescribed protocol.
Statistics
Data are reported as mean (SD), mean difference (95% CI), as median (25th, 75th percentiles) and as absolute and relative frequencies. A paired t-test was used to compare the two HIIT protocols for achieved intensity (time ≥85% of HRmax), relative intensity (% of Wmax), RPE and Likert Scale Scores. All statistical analyses were performed using R statistical software V.4.1.1 (R Project for Statistical Computing) within RStudio statistical software V.1.4.1717 (RStudio) and a two-tailed p<0.05 was considered statistically significant.
Patient and public involvement
Patients and the public were not involved in the design and recruitment process of the study.
Results
A total of 15 patients were invited for baseline testing where 2 patients did not meet the inclusion criteria as they were both classified with GOLD I after lung function testing, while 1 patient resigned after baseline testing due to lack of time. The remaining 12 patients were randomised and completed both HIIT protocols. The two HIIT protocols were separated by a median of 4 days (2, 8)).
Eight patients were classified with GOLD II and four with GOLD III. Six patients had a moderate-to-severe reduction in diffusing capacity (DLCOc <60% of predicted). Baseline characteristics are presented in table 1.
Baseline characteristics
Fidelity
The patients completed the 4×4 HIIT protocol with 41 (2) min and the 10×1 protocol with 51 (2) min, corresponding to a completion of ~98% of the total training duration for both protocols. All patients sufficiently completed the intensity in the 4×4 protocol and spent on average 24 (15) min with an HR ≥85% of HRmax. In the 10×1 protocol, 8 patients completed 10 out of 10 intervals at 100% of Wmax, 2 patients needed an intensity reduction in 5–7 out of 10 intervals and additionally 2 patients needed an intensity reduction in more than 8 out of 10 intervals.
Tolerability
On the 10-point Likert scale, the patients reported similar scores, with 1 indicating not tolerable and 10 completely tolerable, the average score was 7 (2) in the 4×4 protocol and 7 (2) in the 10×1 protocol (p=0.88).
Red–amber–green ranks
The ranks of the red–amber–green system are presented in figure 3. The 4×4 protocol yielded a total of three amber training sessions due to low score of perceived tolerability. The 10×1 HIIT protocol yielded two red training sessions because of extensive intensity reductions in >8 intervals, and two amber training sessions due to low scores of perceived tolerability as well as an intensity reduction in 5 and 7 of the intervals, respectively

Distribution of the red–amber–green training sessions. Number of red-amber-green training sessions within each HIIT protocol. Created using BioRender. HIIT, high-intensity interval training.
Other outcome measures
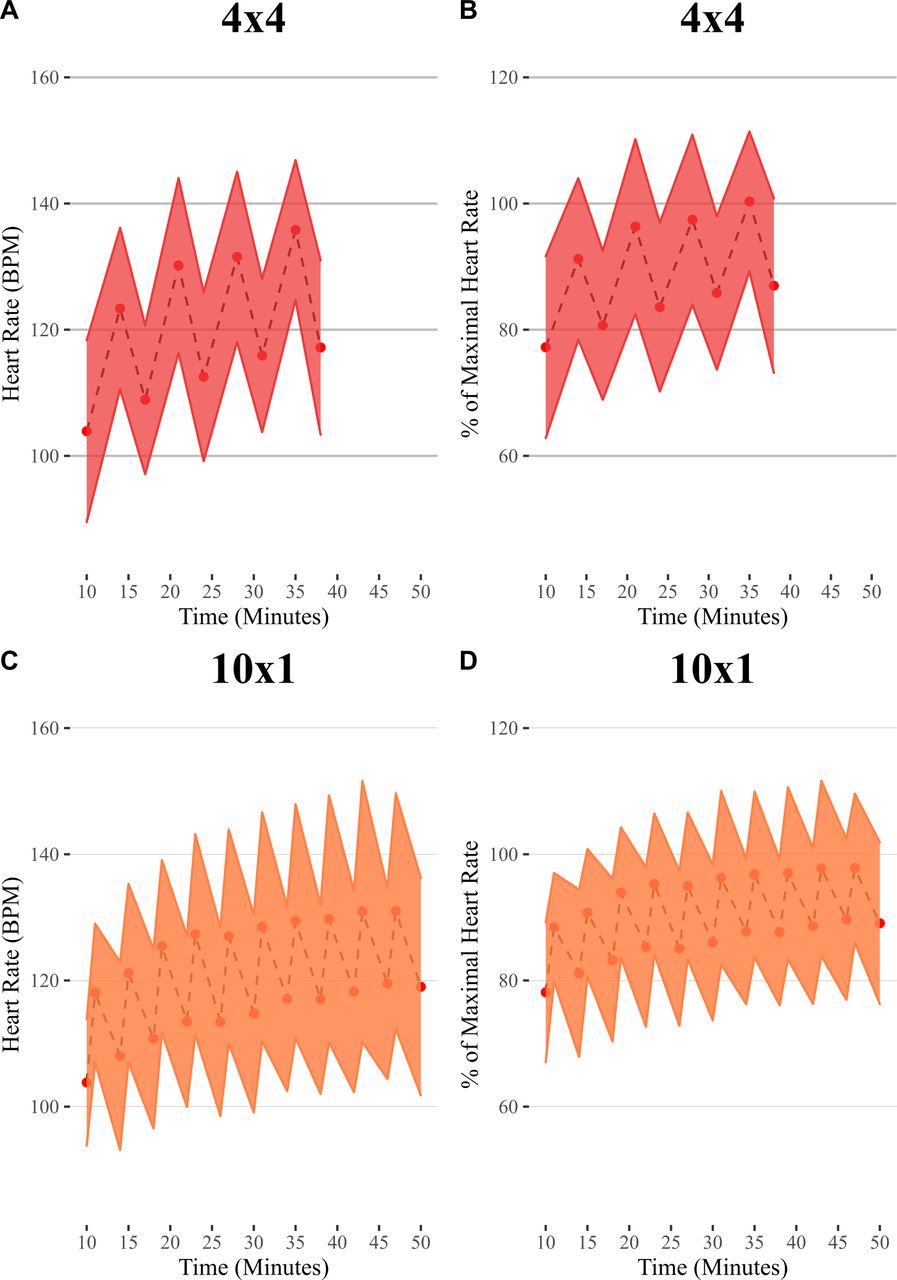
The relative intensity was 70.1% (6.9) and 94.2% (6.5) of Wmax in the 4×4 and 10×1 protocol, respectively. The relative intensity was significantly higher in the 10×1 protocol with a mean difference of 24.1% (95% CI 17.9% to 30.2%, p<0.0001). There was no between-protocol difference for achieved intensity (time ≥85% of HRmax) with a mean difference to the 10×1 protocol of 5 min (95% CI −1 to 12 min, p=0.11), RPE with a mean difference of 0.3 (95% CI −1.0 to 1.7, p=0.601) on the Borg scale or enjoyability with a mean difference of 0.6 (95% CI −0.7 to 1.9, p=0.349) on the 10-point Likert scale (figure 4). However, beyond the ≥85% of HRmax threshold, higher peak HR values were observed during 4×4 protocol than during 10×1 protocol as presented for absolute HR in figure 5A,B and for % of HRmax in figure 5C,D. No SAE occurred during any of the HIIT protocols. Three patients needed to stop cycling during their active break between intervals due to increasing leg fatigue. This pattern occurred during both HIIT protocols for the same individuals.

Intensity, tolerability and enjoyability. (A) Intensity was evaluated as the time spent with a heart rate ≥85% HRmax. (B) Tolerability was rated on a 10-point Likert Scale. (C) Enjoyability was rated on the 10-point Likert Scale. The bar plot is showing data as mean with 95% CI. HRmax, maximum heart rate.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A graphical overview of the heart rate response to each HIIT protocol. A graphical overview of heart rate response for the two HIIT protocols. Both protocols were initiated with a 10 min warmup period. The 4×4 protocol was scheduled to last 42 min and the 10×1 protocol 52 min. (A) displays the 4×4 with absolute HR and (B) displays the 4×4 in % of HRmax, (C) displays the 10×1 with absolute HR and (D) displays the 10×1 in % of HRmax. Each dot s is the mean HR at the end of each interval/rest period and the shadow is the SD of the mean. HIIT, high-intensity interval training; HRmax, maximum heart rate.
Discussion
This study compared the fidelity and tolerability of two commonly used HIIT protocols, using different interval durations, in patients with moderate-to-severe COPD. Our findings suggest that HIIT implemented with longer (4 min) intervals and a relatively lower intensity has a higher fidelity compared with HIIT with intervals of shorter (1 min) durations at a very high intensity.
Fidelity and tolerability
To our knowledge, no studies have yet investigated the fidelity and tolerability of HIIT in patients with COPD and additionally no studies have compared HIIT based on short versus longer intervals. Previous studies indicate that the effect of HIIT on V̇O2peak is similar regardless of interval duration, intensity and work-to-rest ratio used, indicating that short and long intervals share a similar efficiency for increasing exercise capacity and decreasing symptom burden,14–16 29 and Wmax.14 16 17 However, given that our findings do point towards the 4×4 protocol having a higher fidelity than 10×1 protocol, the former may provide a greater efficacy in a real-life setting, as a greater level of patient adherence to the training protocol may be achieved. Because the measurements and comparisons of fidelity and tolerability of the two HIIT protocols are based on only two single training sessions, we nevertheless cannot exclude that our findings may have differed if this had been investigated over a prolonged training period corresponding to a PR programme.
It has previously been proposed that patients with COPD may be at a better chance of reducing the degree of dynamic hyperinflation between intervals when the work-to-rest ratio is relatively high.13 However, four of the patients needed an intensity reduction during the 10×1 protocol due to increasing leg fatigue and not due to dynamic hyperinflation as expected. These findings are supported by a previous study showing that leg fatigue was the most common reason for exercise termination, followed by dyspnoea in patients with COPD.30 Since the 4×4 protocol was completed at a relatively lower intensity compared with the 10×1 protocol, this could indicate that it is not the work-to-rest ratio, but rather the intensity, that is important to achieve protocol adherence. We can only speculate on the cause of leg fatigue, but one explanation could be the increasing competition of blood flow distribution between the pulmonary system and skeletal muscles during intervals,31 where the relatively higher intensity or the longer training amount in the 10×1 protocol likely plays a role. This is supported by previous findings that HIIT based on 2 min intervals at an intensity at 90% of Wmax was poorly tolerated in ~25% of the participants, thus requiring up to 9 training sessions before protocol adherence could be achieved.14
Despite the lower fidelity of the 10×1 protocol, we found no differences in achieved intensity or perceived tolerability between the protocols, even though the relative intensity differed between protocols. This must, however, be considered in the context of the design of the study. Due to increasing leg fatigue and inability to maintain RPM >60, the workload in the 10×1 HIIT protocol was extensively downregulated in four cases. The measure of tolerability and achieved intensity could therefore potentially be different between protocols if downregulation of the workload in the 10×1 HIIT protocol was not accepted.
Limitations
This study has several limitations. The two HIIT protocols were not matched for duration, resulting in the 10×1 HIIT protocol lasting 10 min longer, despite spending a shorter total duration of time at high intensity (4×4: 16 min vs 10×1: 10 min). Thus, we cannot rule out that a difference in the total training amount may have affected our results.
The study was not powered to calculate statistical differences between protocols, which increases the risk of a type 2 error. The between-protocol mean difference of 5 min (95% CI −1 to 12) might, therefore, have clinical importance in terms of longer interventions such as PR. Implementing the 10×1 protocol 3 times a week for 12 weeks could potentially result in almost 200 min more at high intensities (HR >85% of HRmax) compared with implementing the 4×4 protocol, suggesting that the 10×1 protocol could elicit larger clinical benefits over a prolonged period. Nevertheless, if the patients do not tolerate the 10×1 protocol, this might not be the case.
Conclusion
The fidelity of a 4×4-based HIIT was found to be greater than that of 10×1-based HIIT in patients with moderate-to-severe COPD. This was likely because of much higher required intensities during the relatively short intervals of the latter, which may predispose to leg fatigue. In PR for COPD, the use of HIIT based on relatively long intervals may thus provide a greater efficacy, as a higher level of patient adherence to the training protocol may be achieved.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Both oral and written consent was obtained prior to participation in the study, which was approved by the Ethical Committee for the Capital Region of Denmark (H-20052659) and conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We gratefully thank physiotherapist Jeanett Guldager Olsen (Municipality of Hvidovre, Denmark) for a great collaboration.
References
Footnotes
Twitter @NymandStine, @cresp_research @ronan_berg @cfas_dk
Contributors SBN: data collection/extraction, data analysis, data interpretation, first draft, revisions. JH: data collection/extraction, data interpretation, revisions. MR-L: conception and idea, method development, design, data interpretation, revisions. IER: data collection, design, revisions. UWI: method development, data interpretation, revisions. RHC: design, data interpretation, revisions. RMGB: conception and idea, method development, design, data interpretation, revisions, supervision. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. RMGB: guarantor of the work, and thus responsible for the overall content, including the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This work was supported by a grant from the Svend Andersen Foundation. The Centre for Physical Activity Research (CFAS) is supported by TrygFonden (grants ID 101390 and ID 20045).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.