Article Text

Abstract
Objectives The acute effects of aerobic exercise on cardiometabolic markers are well documented in younger healthy individuals, but the same effects in older adults have not been elucidated. As such, this study compares the acute effects of three different types of age-appropriate aerobic exercises on cardiometabolic markers.
Methods Healthy older golfers (n=25, 16 male and 9 female, 68±4 years) were enrolled in a randomised cross-over experiment. We compared the effects of three different acute aerobic exercises (18-hole golf, 6 km Nordic walk, 6 km walk) on blood pressure, blood glucose and blood lipid profile in a real-life environment.
Results In the between-group comparison, playing golf resulted in a difference in blood glucose (golf: 0.01±1.0 mmol/L, walk: 1.3±0.9 mmol/L, p<0.001) compared with walking and triglycerides (golf: 0.13±0.2 mmol/L, Nordic walk: 0.31±0.2 mmol/L, walk: 0.23±0.2 mmol, p=0.012) and high-density lipoprotein cholesterol (golf: 0.04±0.06 mmol/L, Nordic walk: −0.02±0.06 mmol/L, walk: −0.02±0.07 mmol/L, p=0.002) compared with Nordic walking and walking. In addition, all groups had significant decreases (p<0.001) in systolic blood pressure, and Nordic walking and walking also demonstrated a decrease in diastolic blood pressure (p<0.05).
Conclusion Acute bouts of aerobic exercise improved cardiovascular profile in healthy older adults. Despite the lower exercise intensity of golf, the longer duration and higher energy expenditure appeared to have a more positive effect on lipid profile and glucose metabolism compared with Nordic walking and walking.
Trial registration number ISRCTN10007294.
- golf
- exercise
- aging
- cardiovascular
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The acute effects of aerobic exercise and exercise-specific effectiveness on cardiometabolic markers in healthy older adults are unknown.
WHAT THIS STUDY ADDS
These findings represent the first scientific data on the acute effects of playing golf in healthy older adults compared with Nordic walking and walking.
Playing golf affects plasma lipid profile and glucose metabolism more positively than Nordic walking and walking.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These findings could help to elucidate the exercise-specific effectiveness of different types of age-appropriate aerobic exercise on cardiovascular disease risk factors. The study can, therefore, recommend exercise as a preventive factor for older adults and offers treatment strategies to improve cardiometabolic health in older adults who likely already have cardiovascular diseases.
Introduction
Cardiovascular diseases (CVDs) remain the leading cause of rising health costs1 and mortality among the elderly.1 2 Sedentary behaviour and physical inactivity are particularly emphasised as major modifiable cardiometabolic markers,3 which are reflected by the increased prevalence of hypertension, diabetes and dyslipidaemia in older adults.2
CVDs can be prevented by controlling key determinants of cardiometabolic markers, such as blood pressure (BP), blood glucose (BG) and lipids, through lifestyle modifications like exercise.1 Acute aerobic exercise (AE) on lipid profile, BP and BG has been shown to reduce cardiometabolic markers and improve cardiovascular health.4–11 However, most related studies have been restricted to younger individuals in clinical trials with an acute bout of exercise lasting 30–60 min at moderate to high intensity (VO2max 40%–75%) exercise.4–7 11–14 Furthermore, it seems that the effects of acute exercise on these key determinants vary depending on the exercise’s type, intensity and duration.6 15 16
Especially in the ageing population, which has an increased risk of CVDs, a better understanding of the exercise-specific effectiveness of different types of age-appropriate AE on cardiometabolic markers is necessary to recommend exercise as a preventive factor and a treatment strategy.1 2 Golf, Nordic walking and walking are popular age-appropriate forms of outdoor AE which can be considered safe and accessible for older people.15–17 This study investigated whether a single bout of three different types AE in terms of intensity, duration and energy expenditure (golf, Nordic walking, walking) affects the following cardiometabolic markers: systolic BP (sBP); diastolic BP (dBP); BG and lipid levels such as total cholesterol (TC), triglycerides (TGs), low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C).
Methods
Study design
The study was designed as a 5-day randomised cross-over study. Healthy older golfers (n=25) completed three different exercise trials in a real-life environment, in random order and at a self-selected pace. The exercises included an 18-hole golf round in Tarina Golf’s old course (course profile: flat; length from red tees: 4477 m) by pulling-a-trolley walking in 2–3-player groups and predetermined walking routes (profile: flat; length: 6000 m) for Nordic walking and walking. The study protocol is presented in figure 1. Participants were divided for two separate weeks. In addition, using a cross-over design, participants were randomly divided into three groups (n=4–5), which participated in the exercise trials over a 5-day study protocol. For example, the golf group started with an 18-hole golf round on the first day (d1), then completed Nordic walking on the third day (d3) and finished with walking on fifth day (d5). On the second (d2) and fourth (d4) days, there was a 1-day wash-out phase between each exercise trial to minimise any carryover effect of training. All participants were asked to maintain their regular physical activities and nutritional habits and to report these by diary during the 5-day period.

Flow chart of study design.
Participants
Healthy golfers (> 65 years, body mass index (BMI)<35 kg/m2, golf handicap (HCP) ≤ 36, plays at least 18 holes once a week) were recruited from Tarina Golf’s (Siilinjärvi, Finland) official membership register. Recruitment occurred in August 2021; 60 volunteers (n=60) were interested in participating and 34 were recruited for the screening test. Inclusion criteria were male or female, > 65 years of age and BMI <35 kg/m2. Exclusion criteria were diagnosis of dementia, Alzheimer’s disease, Parkinson’s disease and CVDs. Long-term use of hyperlipidaemia and hypertension medication was allowed except for medication that might affect heart rate (HR), such as beta-blockers. The volunteers were measured at the University of Eastern Finland (Kuopio, Finland) for weight, height and body composition were registered using bioimpedance measurement (Inbody 720 1996),18 while waist and pelvis circumference and BP were measured using Omron M6AC.19 In addition, a Urho Kaleva Kekkonen (UKK) 6 min walking test20 was conducted to measure cardiorespiratory fitness, and a short physical performance test21 was used to monitor physical function. Volunteers’ health status and suitability for the study were evaluated by a doctor, and 26 participants were ultimately deemed eligible for the study.
Sample size
The required calculation of the sample size was performed for the main outcome variable of BG. Based on at least 21 participants, walking and golf have a significant statistical difference (p<0.05), assuming a BG concentration of 5.8 mmol/L after golf, 6.4 mmol/L after Nordic walking and 6.4 mmol/L after walking. The SD is 0.7.
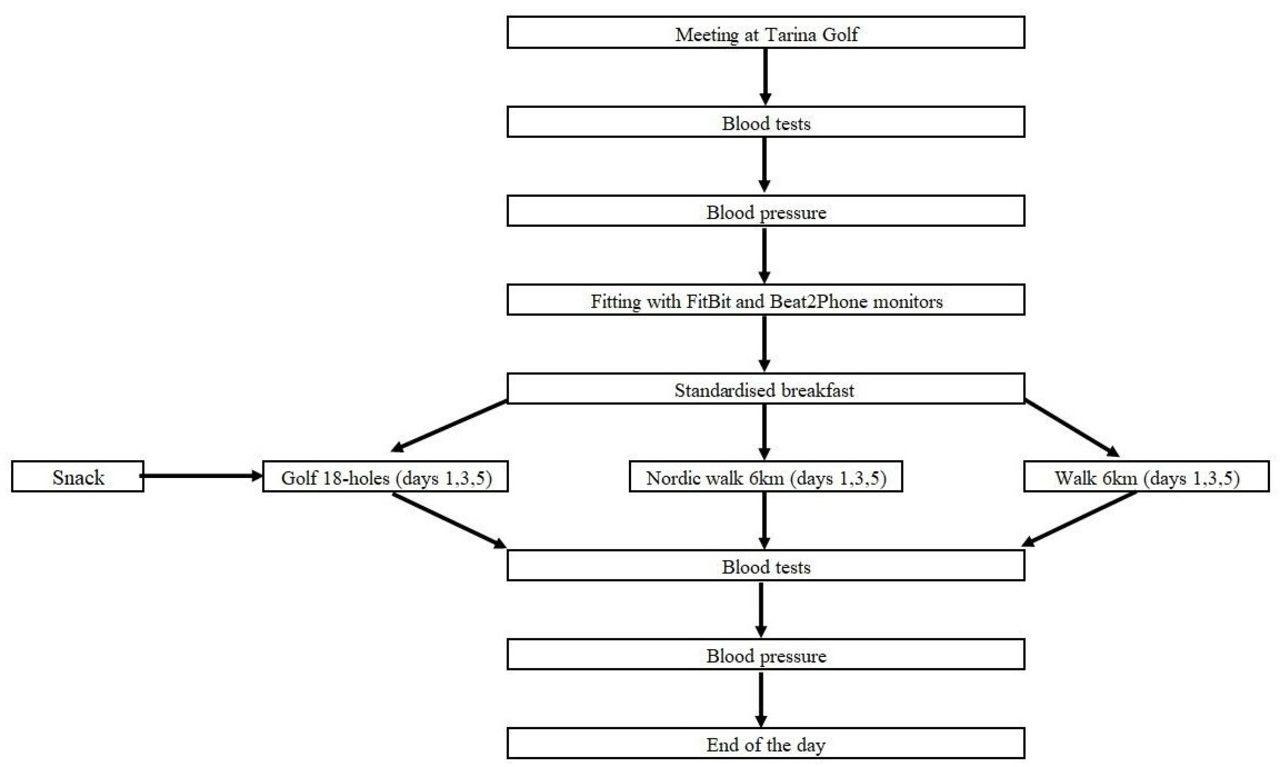
Experimental protocol
The experimental protocol is presented in figure 2. On experimental days, participants arrived at Tarina Golf Course (Siilinjärvi, Finland) at 7:00 hours following an overnight fast (<10 hours). First, blood samples and a BG finger-prick test were taken. Next, non-invasive BP was double-measured using a mercury sphygmo-manometer19 in a sitting position. Then, the participants were fitted with a FitBit Versa 3 on the wrist (USA)22 23—a device to measure exercise-specific distance, duration, pace, energy expenditure and steps. They were also fitted with a Beat2Phone ECG sensor with a chest strap (VitalSignum, Finland)24 25 to measure HR. Following blood samples and BP tests, food was controlled by having the participants consume a standardised breakfast (530 kcal) before the exercise and a snack (150 kcal) during the golf round. One hour after breakfast, each participant started the exercise trial. Participants were instructed to maintain a pace corresponding to a brisk walking speed during each exercise modulate. After the exercise modulates, the measurements were repeated immediately (<15 min). Participants were supervised to ensure consistent behaviour across each of the study trials. In addition, the estimated HR max was calculated as 220 bpm—age during each trial.

{kind=link}
{kind=link}
Flow chart of experimental day protocol.
Blood samples
Blood samples were drawn from the brachial vein after an overnight fast (10 hours) before and after the exercise. Participants were instructed to avoid caffeine, alcohol or physical activity the day before the sampling. Blood samples were collected into Li-heparin tubes for TC, HDL-C, LDL-C and TGs and EDTA tubes for haemoglobin A1c (HbA1c). HbA1c was measured only once before the first morning of the trial. BG was collected using a finger-prick test (Roche, Indianapolis, USA).26 The samples were delivered to a laboratory (ISLAB, KYS, Kuopio, Finland) on the same days as the trials. The concentration of TC, HDL-C, LDL-C, TGs and HbA1c was determined according to the manufacturer’s instructions (cobas 8000 (c 702)—analyser, Hitachi High Technology, Tokyo, Japan). Coefficient of variation for interassay of lipid analysis were less than 2.0% using reagents of the cobas c 702 systems (Roche Diagnostics, Mannheim, Germany).
Statistical analysis
All data were analysed using IMB SPSS Statistics V.27.0 (IBM). The Mann-Whitney U test was also used to compare the exercise-specific outcomes between genders. The Wilcoxon signed-rank test was used to compare cardiometabolic marker outcomes within-group pre-exercise and postexercise session. Due to these markers, the wash-out phase was calculated between day 1 and day 3. Due to the rather small sizes of the groups, the Kruskal-Wallis test was used to assess differences between outcomes in all three groups at baseline and their changes during the trial period. Significant interaction effects of within-subject factors were further analysed using the pairwise comparison, and the Kruskal-Wallis H test was used with post hoc. The significance level was set to p<0.05, and the CI limits were 95%.
Results
Characteristics of study participants
Following the withdrawal of one participant, 25 participants (68±4 years; 16 (64%) males and 9 (36%) females) were eligible for the study. All participants engaged in each exercise modulate, with the exception of one person who did not complete the golf round due to health issues. The characteristics of the subjects are shown in table 1. The study participants had a mean age of 68±4 years, an HbA1c of 37.4±3.6 mmol/L and a VO2max of 33±4 mL/kg/min. Most participants were normal weight to overweight (25±2.5 kg/m2) and had elevated BP (144/89±18/12 mm Hg) and increased TC (5.5±1.2 mmol/L).
Characteristics of the participants
Acute responses to exercise-specific outcomes
The responses in exercise-specific outcomes are shown in table 2. The exercise-related outcomes of distance (p<0.001), time (p<0.001), steps (p<0.001) and energy expenditure (p<0.001) were significantly greater for golf compared with both Nordic walking and walking. However, the average HR of golf (p=0.050) was significantly lower. In addition, the only difference between genders was found in energy expenditure in golf (p=0.032) and walking (p=0.010) as men reported higher values. The average exercise intensity during each trial was 61% in the golf group, 77% in the Nordic walking group and 76% in the walking group.
Acute responses to exercise-specific outcomes
Acute responses to BP, BG and lipid levels
Participants’ acute responses to golf, Nordic walking and walking in terms of BP, BG and lipid levels are shown in table 3. Decreased sBP postexercise was observed in all groups (golf: p<0.001, Nordic walking: p<0.001, walking: p<0.001), while decreased dBP was found in the Nordic walking (p=0.038) and walking (p=0.022) groups. TC did not change throughout the study for the golf (p=0.152) or Nordic walking (p=0.126) groups, but it decreased slightly postexercise in the walking group (p=0.034). TG concentrations increased postexercise in all groups (golf: p<0.003; Nordic walking: p<0.001, walking: p<0.001). Similarly, LDL-C concentrations decreased slightly postexercise (golf: p<0.023; Nordic walking: p<0.019, walking: p<0.036). An immediate increase occurred only with HDL-C in the golf group (p<0.002). In addition, BG levels increased in the Nordic walking (p=0.003) and walking (p<0.001) groups, while the golf group maintained steady BG levels. However, we found that the golf group had significant differences in BG compared with the walking group (golf: 0.01±1.0 mmol/L, walking: 1.3±0.9 mmol/L, p<0.001) and TGs (golf: 0.13±0.2 mmol/L, Nordic walking: 0.31±0.2 mmol/L, walking: 0.23±0.2 mmol, p=0.012) and HDL-C (golf: 0.04±0.06 mmol/L, Nordic walking: −0.02±0.06 mmol/L, walking: −0.02±0.07 mmol/L, p=0.002) compared with Nordic walking and walking. Data from the wash-out period between d1 (pre-exercise) and d3 (pre-exercise) are presented in table 4. Only the golf group demonstrated a significantly lower TC (p=0.011) for approximately 40 hours after exercise.
Acute responses to blood pressure, blood glucose and plasma lipid levels
Wash-out period for pre-exercise of D1 and D3 to blood pressure, blood glucose and plasma lipid levels
Discussion
To author’s knowledge, this was the first study to compare the immediate postexercise effects of acute bouts of golf, Nordic walking and walking on cardiometabolic markers in healthy older adults. Our findings indicate that these acute bouts of AE improve the cardiovascular profile of healthy older adults. Playing golf in particular seems to have a more positive effect on lipid profile and BG.
Acute responses to exercise-specific outcomes
In terms of HR and pace—which are intensity-related indicators—we observed predictable differences between golf, Nordic walking and walking. Previous studies have described Nordic walking as a more effective moderate-intensity exercise,26 27 whereas golf is considered low-to-moderate intensity28 29 because it involves stops, waiting and planning game strategy, thus lowering one’s HR during the game.30 In agreement with our findings, the significantly longer duration of completing a round of golf compared with other exercise types29 31 may explain why golf is a more effective exercise than Nordic walking or walking based on energy expenditure, steps and distance. The energy expenditure of golf—as a long-term, lower-intensity exercise—can also induce positive responses to the metabolism. No significant difference between these exercise-specific outcomes was observed for Nordic walking versus walking. Studies have indicated that Nordic walking requires active use of upper body muscles, which should lead to a higher HR and greater energy consumption compared with walking.27 28 32 33 The lack of any difference in our findings could be due to the evaluation technique as only 25% of participants had tried Nordic walking before.26 34
Acute responses to BG and blood lipids
In the between-group comparison, golf had a more positive effect on TGs and HDL-C than Nordic walking or walking. Golf also had a more positive effect on BG compared with walking. Interestingly, we found that golf seems to have a longer effect on TC compared with Nordic walking and walking. In addition, all the exercises reduced LDL-C and increased TGs. The exercise-specific mechanism of acute exercise on BG and lipids in healthy elderly people is not well known. Nonetheless, our study yielded similar results regarding the effectiveness of acute AE. Based on previous studies, the differences between golf, Nordic walking and walking can be explained by intensity, duration and energy expenditure even though acute effects of golf have not been studied before.5 32 33
Only a few studies with healthy adults have measured the differences in glucose concentrations between AE modalities. This is likely related to differences in carbohydrate metabolism due to the physiological differences of cycling and treadmill exercises in clinical conditions.33 This might be related to the total use of fatty acids (FAs) as an energy source. FA utilisation increases until the intensity of physical activity reaches approximately 60%–65% VO2max and 74% of the maximum HR, at which point an increase in the relative contribution of carbohydrate oxidation to energy expenditure occurs.10 This might clarify the previously reported view that the acute effect of exercise on glucose metabolism appears to require exercise near 70% VO2max.4 In our study, the intensity of golf was approximately 61%, while for Nordic walking and walking it was 76%–77% of the maximum HR. Golf affected BG more efficiently compared with walking due to a longer exercise duration, despite the lower intensity. This observation supports that a longer AE duration seems to provide a larger window for glucose concentration homoeostasis to be achieved.16 The absence of a difference in BG between golf and Nordic walking may be explained by Nordic walking requiring more muscle work, leading to a more positive impact on BG. Most studies have reported that a moderate-intensity exercise duration of around 45–60 min decreases glucose by an average approximate change of −0.83±1 mmol/L in healthy younger participants (31±21 years).35 However, in this study, BG was measured only once immediately (t=15 min) after the exercise session. Thus, there is a possibility that BG increases immediately after Nordic walking and walking but starts to decrease after a few hours as they are more intense activities than golf.
It was recently discovered that even one bout of moderate intensity AE is associated with regulation of the lipid profile, decreased concentrations of TC and LDL-C and increased HDL-C.9 Thus, in sedentary individuals, lipoprotein and lipid changes can occur even after a single exercise session where one expends at least 350 kcal.36 In this study, participants’ energy expenditure was over 350 kcal in all groups. Golf had a longer-lasting effect on reducing TC despite its lower intensity, and an immediate decrease in TC postexercise was observed in walking. It appears that an acute reduction in TGs and an increase in HDL-C seem to be related partly to the AE’s total energy expenditure, intensity and duration4 5 as well as the type of the exercise.32 In this study, only golf increased HDL-C immediately postexercise. The greater energy expenditure in golf can explain this increase compared with Nordic walking and walking, as supported by the finding that after a single exercise session, an acute increase in HDL-C was reported after energy expenditure of 350–400 and 1000 kcal in moderately fit and well-trained individuals.4 HDL-C levels were shown to be more sensitive to AE than LDL-C and TG.37 We found decreases in LDL-C and increases in TG levels in all groups. Most past studies have focused on examining a single 30–90 min acute bout of moderate intensity (60% VO2max) AE (eg, walking, jogging, cycling) in normal to overweight healthy middle-aged men to lipid profile.4 6 7 11 These studies reported that TGs significantly decreased by 8% after an acute bout of AE compared with resistance and combined exercise, but there was no difference in HDL-C or LDL-C.11 In addition, Gill et al6 examined the effects of 90 min of walking on a treadmill at moderate intensity (60% Vo2max) on serum lipid profile in middle-aged men (51±6.1 years) and reported reduced postprandial TG concentration.6 We did not observe reduces in TGs in this study. TGs can be unchanged for 4 hours postexercise, but they may occur 18–24 hours after the exercise bout.4 38 As our blood samples were taken immediately (t=15 min) after the exercise, TGs were likely still elevated as them was an energy source during the exercise.
Acute responses to BP
We found that all three exercise types decreased sBP and that Nordic walking and walking also reduced dBP. An acute bout of exercise can reduce BP during the recovery period.39 A recent meta-analysis supported that sBP decreased significantly regardless of exercise modality and that the longer the exercise session duration is, the greater the sBP reduction.40 Most studies have examined an acute bout of 20–40 min of low-intensity to high-intensity (40%–70% VO2Max) AE (eg, walking, cycling) among men with normal to high BP.12 41 It seems that the acute effect of exercise on BP is a low threshold phenomenon observed after energy expenditures requiring only 40% maximal capacity.4 In this study, sPB decreased immediately postexercise in every group. The reduction in sBP was quite similar in the Nordic walking and walking groups; this was expected as these are more intense AEs than golf. In a recent study, Ebine et al reported that the ground golf protocol reduced mean arterial BP in older adults (66±1.5 years).42 In our study, there was also a statistically significant reduction in sBP despite the lower intensity of golf. The results indicate that golf, Nordic walking and walking might have similar postexercise hypotension effects in healthy older adults. The lack of dBP in golf was expected as dBP does not change during acute low-intensity exercise.39 One past study found that walking does not reduce dBP,40 but another study also reported that dBP does not change during acute low-intensity exercise.39
While this study is focused on acute changes on cardiometabolic markers, it is important to consider the clinical significance of findings regarding the cardiometabolic markers measured. All type of AE, regardless of intensity or duration, appeared to produce favourable effects on BP in older adults. The same effect can be achieved by about 60 min of brisk walking or playing an 18-hole golf round. Aside from this finding, there were no moderate or large clinically significant changes in the other cardiometabolic markers.
Study limitations
Performing a study in a real-life environment according to typical standards allows for high generalisability, but not all factors can be controlled as in a laboratory setting. The small sample size and Fitbit Versa 3 data accuracy, especially on energy expenditure, should be considered carefully when evaluating the results. Due to the trial protocol, we recruited only golfers in the study as it was impossible to assign non-golfers to play a round of golf. Nordic walking was a new type of exercise for most participants, which may have led to poor technique and thereby decreased the effectiveness of the Nordic walking activity. Those who regularly play golf may have better overall health and be in better physical fitness, which limits the generalisability of the results to all older adults or to those with chronic conditions.
Conclusion
In conclusion, all three types of AE improved the cardiovascular profile in older adults when performed in acute bouts despite differences in duration and intensity. However, the lower exercise intensity of golf compared with Nordic walking and walking, the longer duration and higher total energy expenditure involved in playing golf seem to positively affect lipid profile and glucose metabolism. These age-appropriate AEs can be recommended to healthy older adults as a form of health-enhancing physical activity to prevent CVDs and can also be used as a treatment strategy to improve cardiometabolic health among those who already have a CVD.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by the Ethics Committee, Hospital District of Northern Savo Committee (reference number 1073/2021). Every potential participant was informed about the aims and procedures of the study both verbally and in writing.
Acknowledgments
The authors wish to express their gratitude to the study subjects, the personnel of the University of Eastern Finland for the sample and Tarina Golf for use of its facilities.
References
Footnotes
Twitter @juliakettinen, @venojarvi
Contributors JK, MV and HT contributed to the design of the study. JK coordinated the trial and data collectionand is the study guarantor. MV assisted with recruitment and data collection as well as assisted with biochemical analysis. JK wrote the statistical analysis plan and the paper. MV and HT reviewed and edited the paper. All authors approved the final version of the manuscript.
Funding This study was investigator-initiated and funded. Vital Signum donated the Beats2Phone devices.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.