Article Text

Abstract
Objectives The efficacy of exercise-based cardiac rehabilitation (CR) for patient outcomes is well established, with better outcomes when delivery meets recommended guidelines. The aim of this study was to assess how well Australian practice aligns with national CR guidelines for exercise assessment and prescription.
Method This cross-sectional online survey was distributed to all 475 publicly listed CR services in Australia and consisted of four sections: (1) Programme and client demographics, (2) aerobic exercise characteristics, (3) resistance exercise characteristics and (4) pre-exercise assessment, exercise testing and progression.
Results In total, 228 (54%) survey responses were received. Only three of five Australian guideline recommendations were consistently reported to be followed in current CR programmes: assessment of physical function prior to exercise (91%), prescription of light-moderate exercise intensity (76%) and review of referring physician results (75%). Remaining guidelines were commonly not implemented. For example, only 58% of services reported an initial assessment of resting ECG/heart rate, and only 58% reported the concurrent prescription of both aerobic and resistance exercise, which may have been influenced by equipment availability (p<0.05). Exercise-specific assessments such as muscular strength (18%) and aerobic fitness (13%) were uncommonly reported, although both were more frequent in metropolitan services (p<0.05) or when an exercise physiologist was present (p<0.05).
Conclusions Clinically relevant deficits in national CR guideline implementation are common, potentially influenced by location, exercise supervisor and equipment availability. Key deficiencies include the lack of concurrent aerobic and resistance exercise prescription and infrequent assessment of important physiological outcomes including resting heart rate, muscular strength and aerobic fitness.
- Cardiovascular
- Exercise physiology
- Exercise rehabilitation
- Heart disease
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The efficacy of exercise-based cardiac rehabilitation (CR) is well established.
Better patient outcomes when delivery matches guideline recommendations.
How well Australian CR adheres to national guidelines has not yet been evaluated.
WHAT THIS STUDY ADDS
Only three Australian guideline recommendations were consistently reported in current CR programmes: (1) assessment of physical function prior to exercise, (2) review of referring physician results and (3) prescription of light-moderate exercise intensity.
Guideline implementation was suboptimal for baseline haemodynamic assessment and the concurrent prescription of both aerobic and resistance exercise—elements that are associated with enhanced safety and better patient outcomes.
These deficiencies were more prevalent in regional/remote settings, without exercise physiologist supervision, and limited access to equipment. Given that Australian guidelines are themselves less rigorous/concordant with existing evidence than international ones, this implementation gap is highly relevant to effective clinical practice.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Future studies should include on-site auditing of CR protocols and outcomes to confirm the survey findings and evaluate future guideline adherence.
Nationwide reporting of individual programme outcome data, including patient-reported outcomes, is needed to evaluate and benchmark quality and effectiveness.
An update to the outdated national guidelines in conjunction with an educational initiative to aid dissemination is necessary to align service delivery with current evidence.
Introduction
Cardiac rehabilitation (CR) programmes include multidisciplinary interventions to improve health-related outcomes and reduce cardiovascular (CV) risk factors like physical inactivity, obesity, poor diet and smoking.1 CR reduces the rate of CV complications following acute cardiac events, surgical interventions and chronic heart failure, and CV and all-cause mortality.2 In addition, CR improves quality of life, and reduces the risk of hospital readmission and mortality in both coronary artery disease2 (CAD) and heart failure.3 In CAD specifically, aerobic exercise has been shown to reduce the rate of restenosis following angioplasty,4 in conjunction with favourable changes in aerobic capacity and vascular function.5
CR practice in Australia is informed by: (1) a 2004 national framework from the National Heart Foundation of Australia (NHF),6 (2) a 2015 guidance document outlining the core components of CR from the Australian Cardiovascular Health and Rehabilitation Association (ACRA)7 and (3) a 2020 standardised programme resource from the Victorian branch of the NHF.8 All three recommend light-moderate intensity aerobic exercise in addition to a comprehensive baseline assessment of clinical history and functional capacity. Both Australian and international guidelines also recommend resistance training to augment aerobic fitness and muscular strength,9 citing no additional risk of adverse CV events.10 This strong and consistent body of evidence has led to both aerobic and resistance exercise being included in both Australian and international CR guidelines11 (see online supplemental tables 1 and 2), although no prescriptive detail for resistance exercise is present in Australian guidelines.
Supplemental material
Given that benefits of CR are expected when it is implemented with fidelity to guidelines, it is important to investigate how well Australian CR programmes adhere to current recommendations regarding optimal assessment and exercise prescription. Although previous CR surveys have described service characteristics, cohort demographics and broad exercise prescription practices,12 13 they have not included details on pre-exercise assessment, exercise modality and intensity, detailed analyses of potential factors, which may influence exercise testing and prescription, or concordance with national guidelines. Therefore, this investigation will gather information on current exercise assessment and prescription practices in Australian CR services to (1) evaluate the current state of practice and its fidelity to national guideline recommendations and (2) explore factors which may influence the effectiveness of CR service delivery around Australia.
Methods
The study was a cross-sectional survey of all publicly listed CR services in Australia, correct on 27 January 2017. Potentially eligible services were identified from the publicly available online directory, hosted on the ACRA website.14 Any services providing only telephone information were contacted to request email information. No exclusions were made based on any information provided within the database such as rehabilitation phase, type of services offered, location or funding model.
The survey was distributed via email on 1 February 2017 and was available for 4 weeks, with data collection ceasing on 28 February 2017. An initial email was distributed to the programme manager for all eligible services, outlining the purpose of the study and inviting them to complete the online survey. For emails that were ‘undeliverable’, a single follow-up telephone call was made to request updated email details. Two reminder emails were sent 1 and 3 weeks after the initial email to services who had not completed the survey nor declined participation in the study. To encourage completion, participants who completed the entire survey were entered into a prize draw for a tablet computer, fitness watch or small gift voucher.
The survey was hosted and designed within the Survey Monkey website15 and consisted of four sections: (1) programme and client demographics, (2) aerobic exercise training characteristics, (3) resistance training characteristics and (4) pre-exercise assessment, exercise testing and progression. Section 1 collected basic programme and client details including location, remoteness (defined using postcode and the Australian Statistical Geography Standard classifications),16 phase of rehabilitation, typical diagnoses, sex proportion, age range and supervisor qualification details. Sections 2 and 3 collected information on the use of aerobic and resistance exercise respectively, including exercise intensity, monitoring and reasons for selecting specific intensities. Exercise intensity was defined as per the American College of Sports Medicine17 and included very light-light (VO2max <45%, Borg RPE <11), moderate (VO2max 45%–59%, Borg RPE 11–12), hard (VO2max 60%–84%, Borg RPE 13–16) and very hard-maximal (VO2max ≥85%, Borg RPE ≥17). Section 4 gathered information on the type of pre-exercise assessment and exercise tests used and how exercise training sessions were progressed. The design of previous Australian surveys12 13 was considered to ensure novel information was collected. The survey primarily contained categorical variables with the option to include additional open-ended feedback on each question. To reflect the variable nature of clinical practice, participants could choose more than one option for many questions.
At the conclusion of data collection, survey responses were downloaded from Survey Monkey and stored on secure servers hosted by the University of Sydney. Data were subsequently coded and analysed using the SPSS Statistical Software V.22 (IBM). Incomplete surveys were not excluded from final analyses, however, analyses at the question-level included all available and valid responses. Categorical variables are presented as number (n) and proportion of overall responses to each individual question (%). Where appropriate, categories were collapsed for more concise and simplified comparisons, for example, exercise intensities ‘vigorous’ and ‘maximal’ were collapsed into a single ‘vigorous-maximal’ category (online supplemental table 3). Dependent variables were defined a priori as service demographics, screening and assessment type, exercise frequency and exercise intensity. Exploratory analyses examining potential relationships between dependent variables and categorical variables of interest used the Fisher’s exact test statistic, with p<0.05 accepted as statistically significant. Pearson’s χ2 statistic was deemed inappropriate due to the limited sample size.18 These detailed analyses are presented in online supplemental tables 4–6, along with OR and 95% CIs.
Results
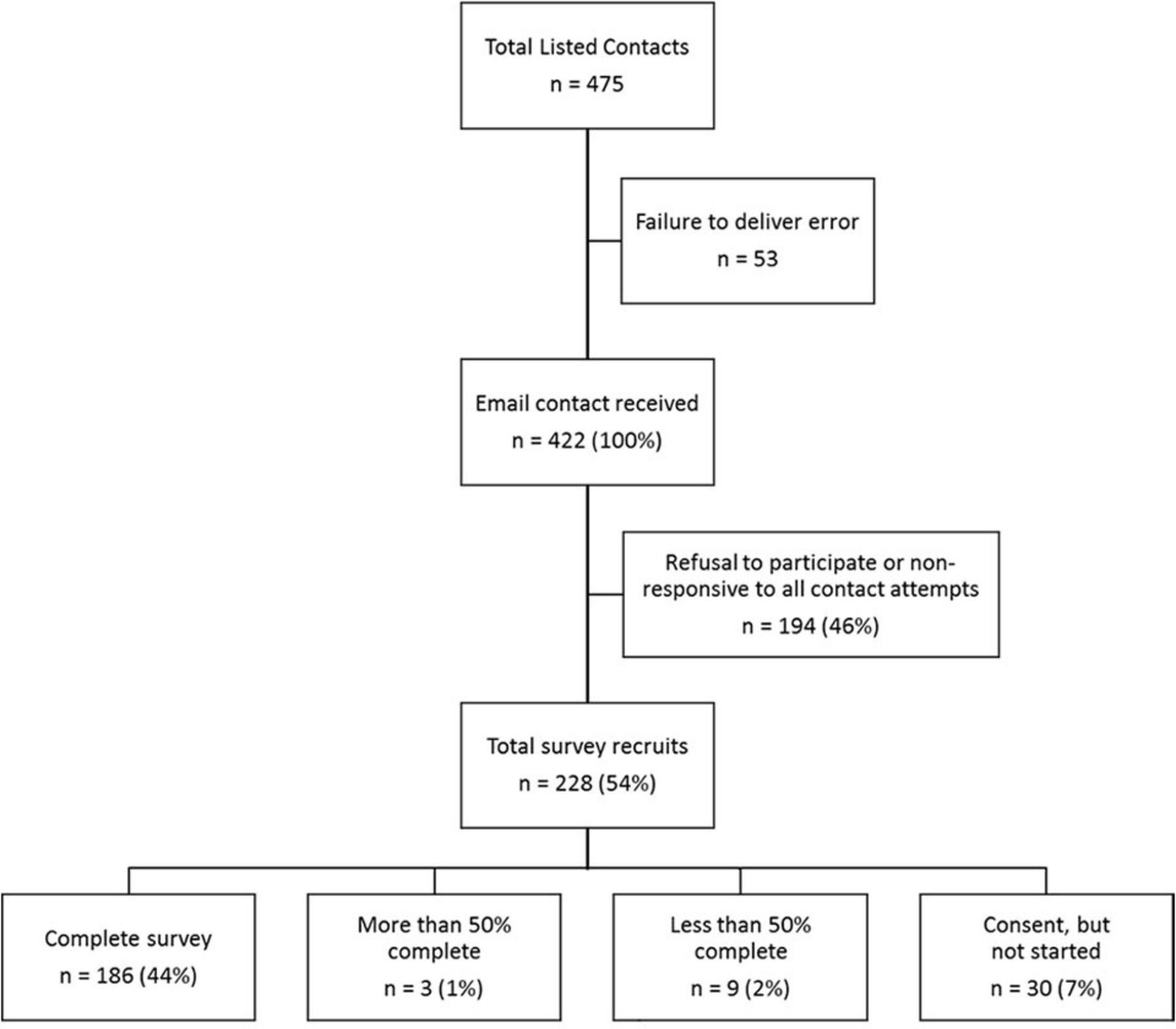
The survey was distributed to all 475 contacts listed in the ACRA database, with 422 emails received. In total, 228 (54%) responded, including 186 (44%) complete surveys, 12 (3%) incomplete surveys and 30 (7%) providing only consent but not commencing the survey (figure 1).

Flow of respondents through the recruitment phase. n, number of respondents; (%), proportion of total respondents that received email contact.
Service characteristics
New South Wales and Victoria represented 48% of total survey respondents (24% each; table 1). Queensland and Western Australia had the highest response rates, with 41% and 38% of listed services responding. The majority of respondents were located within metropolitan (Remoteness Area (RA) 1, 47%) and regional areas (RA2, 24%; RA3, 13%), with limited respondents in remote areas (RA4, 1%; RA5, 2%). A median of 2 (range: 1–6) different healthcare professional disciplines directly supervised exercise in each service. Nurses and physiotherapists were the most common exercise supervisors (70% and 68%, respectively), while exercise physiologists were present in only 30% of services (figure 2). Compared with regional services, metropolitan services enrolled more patients aged 50–59 (OR (95% CI): 3.59 (1.27 to 10.15); online supplemental table 4A), more inpatients (17.76 (2.31 to 136.49); online supplemental table 4B) and more patients with ‘Other CAD’ diagnoses (5.92 (1.29 to 27.16); online supplemental table 4C). Regional services enrolled more patients aged 70+compared with to metropolitan services (0.44 (0.23 to 0.84); online supplemental table 4A). Service remoteness was not associated with differences in exercise supervisor.

Summary of supervisors overseeing the exercise component of each programme, expressed as proportion of respondents (%; n=198). Note that (A) shows prevalence of supervisors where respondents could select more than one option, whereas (B) shows the cumulative prevalence of different supervisor combinations for the three most prevalent supervisor types. AHP, allied health professionals; EP, exercise physiologist; MD, medical doctor; OT, occupational therapist; Phys, physiotherapist; RN, registered nurse.
Characteristics of responding services, expressed as number of survey responses and proportion of responses within each characteristic
Pre-exercise assessment
The average number of assessments per service was 3±2, with only two respondents not reporting any initial screening or assessments (figure 3). Among the three key assessments recommended in the Australian guidelines (see online supplemental table 1), evaluation of physical function was the only procedure consistently reported (91%) by participating services. The other two recommendations, review of referring physician results and resting ECG or heart rate (ECG/HR), were reported substantially less often (75% and 58%, respectively). Two additional assessment domains recommended by international (but not Australian) guidelines, aerobic fitness and cardiac function, were reported infrequently (13% and 11%, respectively). The assessment of muscular strength was reported by 18% of participating services.

Summary of screening and testing procedures conducted prior to first exercise session, expressed as proportion of respondents (%; n=186). Note that each respondent was able to make multiple selections.
Metropolitan services more frequently assessed aerobic fitness, strength and resting ECG/HR than regional services (OR (95% CI): 3.59 (1.27 to 10.15), 5.44 (1.97 to 15.00), 2.29 (1.22 to 4.32), respectively, online supplemental table 5C). However, service location was not associated with the assessment of cardiac function, physical function, use of a physical examination or review of referring physician results. The presence of a supervising exercise physiologist was associated with an increased frequency of both aerobic fitness (OR (95% CI): 4.39 (1.83 to 10.53), online supplemental table 5F) and muscular strength testing (5.00 (2.27 to 11.04), online supplemental table 5F) compared with services without an exercise physiologist.
Exercise prescription
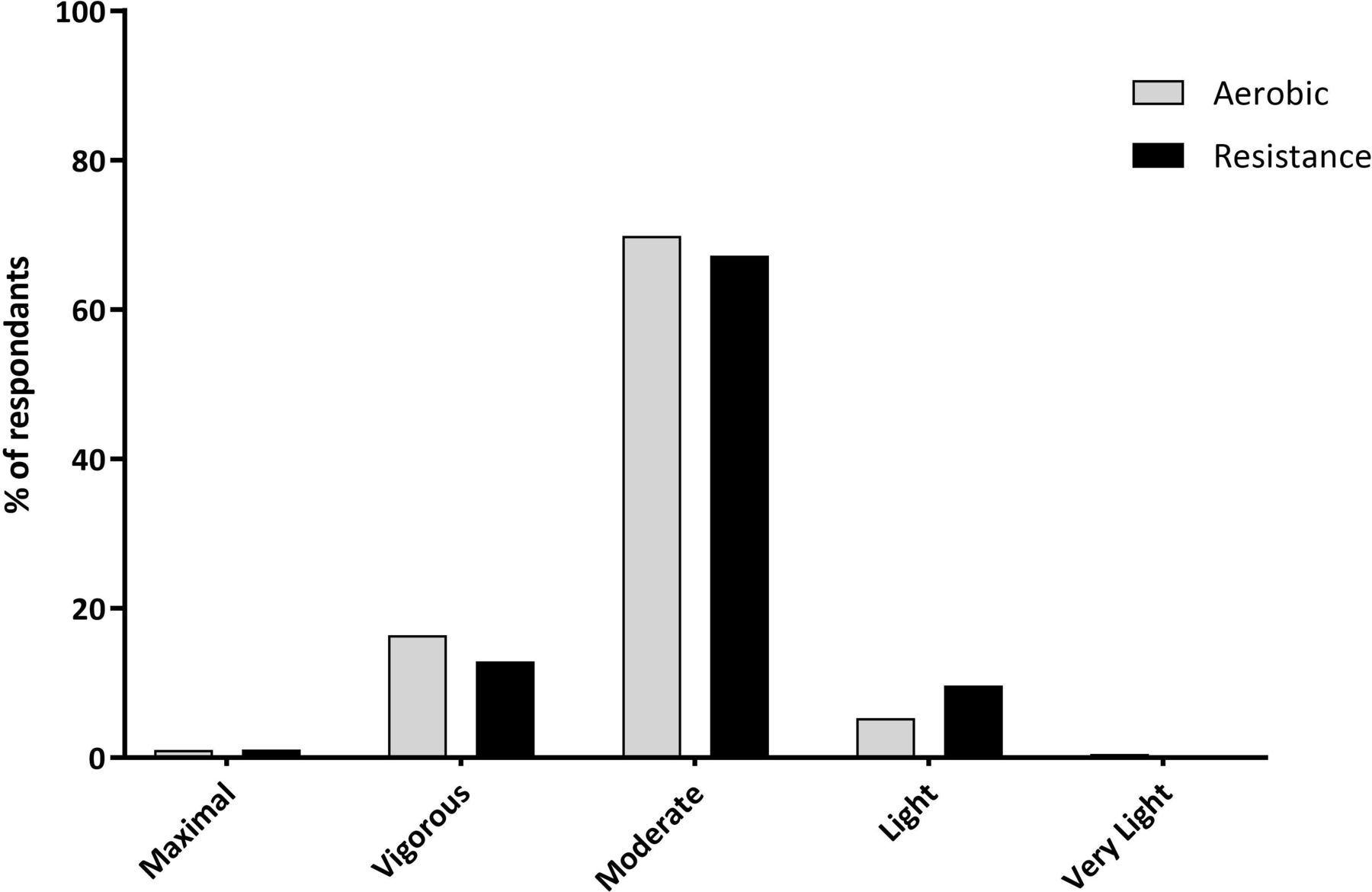
Most (97%) programmes prescribed exercise, however, only 74% and 65% reported ‘always’ prescribing aerobic or resistance exercise, respectively, with only 58% reporting they ‘always’ prescribed both types simultaneously and were thus concordant with guidelines to prescribe both exercise modalities. Consistent with Australian guidelines, moderate intensity exercise was most consistently reported, making up 70% of aerobic and 67% of resistance exercise prescription responses, while 16% and 13% of respondents reported a higher intensity ceiling for their patients (figure 4). Common aerobic exercise modalities were indoor cycling (90%), treadmill walking/running (81%) and indoor/outdoor walking/running (70%). Resistance exercise was most commonly performed using free weights (95%), resistance bands (69%) or the patient’s own bodyweight (68%).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of highest reported intensity, expressed as proportion of respondents (% Aerobic, n=189; resistance, n=186).
Both aerobic and resistance exercise prescription frequency and intensity were associated with the exercise equipment used in services. The use of an indoor cycle, rowing ergometer or any type of resistance training equipment was significantly associated with a higher prevalence of concurrent exercise prescription (p<0.05). Additionally, the services that used weight-lifting machines more commonly prescribed vigorous-maximal intensities rather than low-moderate intensities of resistance exercise (OR (95% CI): 4.25 (1.76 to 10.27), online supplemental table 6H). Somewhat surprisingly, vigorous-maximal intensities of resistance exercise were also more commonly prescribed than low-moderate intensities in services using body weight resistance exercises (4.00 (1.14 to 13.97), online supplemental table 6H). Neither remoteness or supervisor discipline were associated with differences in the intensity or frequency of aerobic or resistance exercise, nor the concurrent prescription of both.
Adherence to national/international guidelines was the most commonly reported reason for exercise intensity selection in aerobic (80%) and resistance exercise (68%). During aerobic exercise, respondents more frequently reported that intensity was selected to minimise cardiac-related safety concerns than to minimise musculoskeletal concerns (60% vs 37%, p<0.001), whereas during resistance exercise, musculoskeletal concerns were more frequently reported than cardiac-related concerns (58% vs 53%, p<0.001). The most frequently reported ways that aerobic and resistance exercise were progressed were through intensity (83% and 86%, respectively) and volume/time (63% and 75%, respectively). Progression of exercise via increases in duration or frequency of sessions was less common, while retesting exercise performance to establish a new maximal capacity was reported by less than 12% of respondents.
Discussion
The key finding of this investigation was that only three Australian guideline recommendations were consistently reported in current CR programmes: (1) assessment of physical function prior to exercise, (2) review of referring physician results and (3) prescription of light-moderate exercise intensity. Importantly, current practices appear suboptimal in elements associated with better patient outcomes and enhanced safety such as the pre-exercise assessment of resting ECG/HR and the concurrent prescription of both aerobic and resistance exercise, which were not reported by a large proportion of responding services (42% for both). Exploratory analyses revealed that these deficiencies were more prevalent in regional/remote settings, without exercise professional supervision, and limited access to equipment. Given that Australian guidelines are themselves less rigorous/concordant with existing evidence than international ones,11 this implementation gap is relevant to effective clinical practice, suggesting the need to improve service delivery in Australian CR.
Our survey fills a significant knowledge gap. Among previous CR surveys, only four have presented data on exercise intensity,12 13 19 20 two within Australia. Our findings share some consistency with results from previous Australian surveys. Specifically, the majority of survey responses were from New South Wales and Victoria,13 exercise was commonly supervised by a nurse or physiotherapist,12 and walking or indoor cycling were the most common aerobic exercise modes.12
Pre-exercise assessments
In concordance with Australian guideline recommendations, assessment of physical function and physician referral, and prescription of light-moderate exercise intensity were consistently reported by the majority of programmes, independent of service location and supervisor type, and consistent with previous Australian surveys.12 13 High uptake of physical function assessments may be related to the testing method employed, with the 6 min walk test (6MWT) the most common assessment of physical function in Australian CR practice.12 Importantly, the 6MWT is a valid and reliable outcome measure in CR,21 which has strong prognostic value with mortality if less than 300 m,22 and is easily implemented in most clinical settings with minimal equipment or personnel required. Consequently, the 6MWT is recommended in European guidelines as an accepted assessment of exercise tolerance in CR, where access to an exercise stress test is not possible.23 In the Australian context, where our study found a low uptake of exercise capacity assessments, 6MWT may be a useful alternate method of assessing the functional response to CR, where mean pre–post improvement has been reported to exceed 20% in a single-centre study of 2524 CR participants.24 However, observational data from Australia suggest that exercise capacity assessments are needed in practice to accurately classify initial exercise capacity and subsequently tailor exercise prescription in CR.25
The specific assessment of resting ECG is recommended in major North American and European guidelines,23 26 despite the inconclusive prognostic benefit in high-risk cohorts.27 In the present study, 42% of services failed to assess resting ECG/HR. This deficiency was more apparent in regional services compared with metropolitan ones, and in services not often using costly exercise equipment, suggesting that funding or equipment limitations may play a role implementation of this recommendation. A previous Australian survey investigating the implementation of psychosocial assessments in CR found that time, funding and resources were the key barriers to a more comprehensive assessment uptake,28 similar to what we observed in exercise assessment and prescription elements described above. Only one previous CR survey in North America has reported on guideline-recommended ECG assessment, similarly finding that a resting ECG was performed in 47% of phase II programmes in the state of Ohio, USA.29
Exercise modalities
Most surveyed services (97%) prescribed exercise, however, 47% failed to meet the national recommendations to concurrently prescribe both aerobic and resistance exercise. The uptake of concurrent exercise was more prevalent in services with access to resistance exercise equipment and aerobic exercise ergometers. The concurrent prescription of both aerobic and resistance exercise is recommended in all major international CR guidelines,23 26 and is efficacious for improvements in CV risk factors like obesity, cardiorespiratory fitness, plasma lipids, inflammation and psychological health.30 The positive effect of aerobic exercise on cardiorespiratory fitness is well established,31 however, recent meta-analyses have shown that the inclusion of resistance exercise has an additive effect on cardiorespiratory fitness compared with isolated aerobic exercise programmes in CAD,9 32 thus highlighting the importance of including both exercise modalities for optimal outcomes. In addition to this aerobic fitness benefit, with advancing CV disease (CVD), the role of skeletal muscle becomes increasingly important for the maintenance of physical function, quality of life and independence, particularly in the most deconditioned cardiac patients with chronic heart failure and cardiac cachexia.33 Notably, high intensity resistance training improves skeletal muscle impairments and exercise capacity in chronic heart failure, largely explained by skeletal muscle adaptations rather than central cardiac adaptations.34 Furthermore, the inclusion of resistance training becomes increasingly more important with ageing patients given its unique ability to address age-associated comorbidities including falls, osteoporosis, frailty and sarcopenia,35 which are not improved with aerobic training.
Aerobic exercise intensity
The prescription of low-moderate intensity aerobic exercise most commonly is also consistent with Australian guideline recommendations. However, it should be noted that these guidelines themselves may require updating considering the rapidly expanding body of evidence since their last revision in 2004. High-intensity aerobic exercise has demonstrated promising improvements in health and fitness compared with lower intensities of exercise in patients with CVD.36 Although the risk of CV events is greater during high intensity compared with moderate intensity aerobic exercise, the major CV event rates for patients with CVD remain very low at 1/11 333 patient-exercise hours.37 As a result, recent guidelines from Europe and North America have extended aerobic exercise intensity thresholds to include higher intensities,23 26 with some evidence of uptake in CR services in the Netherlands.20
Resistance exercise intensity
Australian guidelines do not currently include any specific resistance exercise intensity recommendations, thus, it is more difficult to assess the appropriateness of Australian CR service delivery in this regard. All but 13% of services reported low or moderate intensity resistance training. In contrast, major international guidelines from Europe and North America provide detailed recommendations for moderate-vigorous intensity resistance training,23 26 with uptake apparent within a national CR survey in the Netherlands.20 The benefits of moderate-intensity resistance exercise in CR are well established, however, despite some emerging evidence, more research is needed to properly evaluate the use of high-intensity resistance exercise in this setting,9 given its safety and efficacy for improving health and functional outcomes in other chronic disease cohorts.38
Limitations
A limitation of the current study was the lower response rate in comparison to previous Australian surveys12 13 which may, in part, be explained by this investigation’s significantly shorter enrolment period, broader inclusion criteria and survey distribution method independent of national governing bodies. Furthermore, identifying information was not collected in the survey, which limited the ability to identify and remove duplicate entries from the final analysis. The current survey also did not allow for the addition of any programme outcome information or open-ended qualitative responses, which is necessary to properly evaluate the operation and effectiveness of national CR programmes. The self-reported nature of this survey must be acknowledged as a limitation, which could be improved by using an audit-based research study, similar to the ongoing work in the UK.39
Conclusion
The main finding of this study is that only three Australian guideline recommendations were consistently reported in current CR programmes: (1) assessment of physical function prior to exercise, (2) review of referring physician results and (3) prescription of light-moderate exercise intensity. Key deficiencies include the lack of concurrent exercise prescription and the infrequent assessment of resting HR and ECG, which may be influenced by location, exercise supervisor and equipment availability. The scarcity of muscular strength and aerobic fitness assessments could have implications on the quality of tailored exercise prescription, where actual prescription is unable to be informed by individual capacity.
Implications for future research and practice
Future work should incorporate programme outcome data into the evaluation of programme effectiveness. In addition, assessment of patient-reported outcomes such as quality of life and satisfaction would be a vital addition to the staff-centred and facility-centred nature of all previous surveys, including this one. Future studies including the on-site auditing of protocols and outcomes in CR would provide evidence as to whether changing these elements does indeed improve adherence to guidelines, and more importantly, patient outcomes.
To address the issue of suboptimal pre-exercise assessment and prescription in Australian CR programmes described above, additional funding and resources may be required to overcome potential uptake and accessibility barriers, ensure the continued education of practitioners and encourage the concurrent prescription of both exercise modalities as recommended by current guidelines. Specifically, these may include (1) the employment or support of exercise physiologists to aid in the uptake of exercise-specific assessments, (2) the additional funding to ensure the appropriate equipment is available for all guideline-required assessment and prescription practices and (3) an update of the national guideline so there is a clear policy that services can use to justify equipment requests.
Finally, an update of the 2004 national guidelines to bring them closer to current international recommendations and existing evidence, followed by an educational initiative and review of service equipment and staffing policies may be warranted for the broad range of allied health disciplines involved in Australian CR, to facilitate the translation of clinical trials evidence into practice.
Supplemental material
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
All material and procedures were approved by the University of Sydney Human Research Ethics Committee (HREC approval number: 2016/971). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to acknowledge all CR service staff and managers who took the time to participate in this survey. We would also like to thank Professor Robyn Gallagher for her critical review of the manuscript prior to submission.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrExerciseNerd, @DrYorgiMavros, @Dr_Freezo, @mariafiatarone
Contributors Study design and conception: all authors. Survey tool design: all authors. Data collection: MH. Data analyses: MH, YM and MFS. Manuscript drafting and critical revisions: all authors. All authors approved the final version of this manuscript.
Funding The doctoral candidature of the first author, from which this work was produced, was supported by a Research Training Program scholarship funded by the Australian Government. A small portion of these funds were used to purchase prizes used in this investigation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.