Article Text

Abstract
Objectives To describe the perceived importance of suggested hamstring injury risk factors according to chief medical officers (CMOs) of European male professional football clubs. A secondary objective was to compare if these perceptions differed between teams with a lower-than-average hamstring injury burden and teams with a higher than average hamstring injury burden.
Methods First, CMOs of 15 European professional male football clubs were asked to suggest risk factors for hamstring injury in their club. The perceived importance of the suggested risk factors was then rated by all participants on a 5-graded Likert scale. Participating teams were divided in two groups depending on their hamstring injury burden during the 2019/2020 and 2020/2021 seasons. The LOW group consisted of seven teams that had a lower than average hamstring injury burden. The HIGH group consisted of eight teams that had a higher-than-average hamstring injury burden.
Results Twenty-one risk factors were suggested. The majority were extrinsic in nature, associated with coaching staff, team or club rather than players themselves. ‘Lack of communication between medical staff and coaching staff’ had the highest average importance (weighted average=3.7) followed by ‘Lack of regular exposure to high-speed football during training sessions’ (weighted average=3.6). The HIGH group perceived the player factors fatigue and wellness as more important than the LOW group.
Conclusion According to CMOs recruited in this study, most risk factors for hamstring injuries are extrinsic and associated with the club and coaching staff, and not the players themselves.
- football
- injury
- hamstring
- muscle damage/injuries
- soccer
Data availability statement
No data are available. The dataset from this study is held securely in coded form and data are not available to the public.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Hamstring injury is the most common injury diagnosis in professional football.
While programmes to prevent hamstring injuries have been shown to be effective, no reduction in the rate of hamstring injuries has been observed in male professional football.
WHAT THIS STUDY ADDS
Several risk factors may contribute to hamstring injuries
According to the chief medical officer’s, the majority of these are extrinsic (ie, associated with the club and coaching staff) rather than intrinsic (associated with the players themselves).
Most of the risk factors proposed are associated with factors controlled by coaches such as excessive training, too many matches and overloading with subsequent increases in fatigue or poor training leading to undertraining and muscular dysfunction.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study highlights the responsibility of the club and coaching staff in reducing the risk for hamstring injury in professional football. A better understanding of the importance of communication between medical and coaching staff, as well as improvement in load management and training content during the football season could potentially lead to a fall in the rate of hamstring injuries among professional players.
Introduction
In 1999, the Union of European Football Associations initiated a research project aimed at reducing injuries and increasing player safety in male professional football—the Elite Club Injury Study (ECIS).1–5 We have previously reported that hamstring injuries constitute 19% of all time-loss injuries, that is, about eight hamstring injuries each season in a typical 25-player squad.6 Further, hamstring injury is reported to be the most common recurrent injury in football.7
Between seasons 2001/2002 and 2013/2014, the rate of match-related hamstring injuries was stable whereas the rate of training-related hamstring injuries increased by an average of 4% each year.8 During the recent eight seasons (2014/2015–2021/2022), the incidence and burden of hamstring injuries during training and match play have increased significantly,6 and the proportion of injuries diagnosed as hamstring injuries increased from 12% in 2001/2002 to 24% in 2021/2022.6
Various risk factors for hamstring injuries have been proposed,9–14 and clubs have embraced systematic hamstring prevention programmes to greater or lesser degrees.15
The aim of this study was to assess the educated opinions and current knowledge on preventable risk factors for hamstring injuries based on information from 15 chief medical officers (CMOs) at European male elite clubs. A second aim was to compare the opinion of risk factors between teams that had lower than average hamstring injury rates with teams that had higher than average hamstring injury rates during seasons 2019/2020 and 2020/2021.
Material and methods
Study design
This was an observational cohort study with prospectively collected injury data and retrospectively collected questionnaire in clubs participating in the ECIS.
Study participants
A total of 17 clubs participated in ECIS and qualified for the initial stage of either the UCL or Europa League in both 2019/2020 and 2019/2020 seasons. These 17 teams delivered complete injury data for both seasons. Two of the invited teams did not answer the questionnaires and were excluded. The remaining 15 teams came from 9 countries (3 teams from England, 3 from Germany, 2 from the Netherlands, 2 from Spain and 1 each from Portugal, Russia, Belgium, Italy and Hungary).
Exposure and injury data collection
Exposure and injury data collection for seasons 2019/2020 and 2020/2021 was completed in September 2021. Definitions and method of data collection have been described in detail previously.16–18
The 15 teams were divided into two groups; one group with 7 teams having lower than the mean of all teams for hamstring injury burden (group LOW) and one group with 8 teams (group HIGH) with higher than the mean of hamstring injuries during the two seasons.
Table 1 shows the hamstring injury data for all the 15 clubs as well as the teams in the two groups.
Hamstring injury data of clubs with lower-than-average hamstring injury (HI) rate (group LOW, n=7), clubs with average or higher than average hamstring injury rates (group HIGH, n=8), and the average for the total group (n=15)
Injury was defined as ‘Any physical complaint sustained by a player resulting from a football match or football training, that leads to the player being unable to fully take part in football training or match play thereafter’. A hamstring injury was defined as ‘A traumatic distraction or gradual onset injury to the hamstring muscle group’. Injury burden was defined as ‘number of lay-off days per 1000 player hours ((Σ lay-off days/Σ exposure hours) × 1000)’. Injury incidence was defined as ‘number of injuries per 1 000 player hours ((Σ injuries/Σ exposure hours) × 1000)’.
The survey questionnaire
The CMOs were informed that the aim of the questionnaire was to assemble and evaluate their expert opinions and conclusions on preventable risk factors for hamstring injury in male elite football. The medical officers were asked to base their responses on their practice and experience during the two preceding seasons 2019/2020 and 2020/2021. After agreeing to participate in the study, they were provided access to the questionnaire using the online survey software SurveyMonkey (SurveyMonkey, California, USA). The survey was conducted in two stages. The first stage consisted of an open question asking the medical officers to share their opinions on what they believed could be preventable risk factors for hamstring injury. Their answers revealed 21 potentially preventable risk factors (table 2). In the second stage, the officers were asked to evaluate perceived importance of each of these 21 risk factors using a 5-graded Likert scale (very important, important, moderate importance, minor importance, no importance).
Perceived modifiable risk factors for hamstring injuries, divided between intrinsic factors (players) and extrinsic factors (coaching, team, club)
Survey analysis
Scores were as follows: very important was weighted 4; important=3; moderate importance=2; minor importance=1 and no importance=0. A ‘no opinion’ alternative was also available. Scores were then averaged and risk factors ranked in order of averages.19 20 For each risk factor, a weighted average was calculated (sum of variables x weight)/(sum of all weights).
Patient and public involvement
This research was carried out without patient (player) involvement, that is, players were not invited to comment on the study design or to contribute to the drafting of this document.
Results
Fifteen CMOs replied to the survey. Perceived risk factors, their importance and their weighted average are shown in table 2.
Among the 21 perceived modifiable risk factors, 12 were considered extrinsic factors (relating to coaching, team and club) and 9 suggested being intrinsic or player factors. Further, the importance of the factors, as expressed as the mean of the weighted averages, was 3.1 for the extrinsic factors compared with 2.9 for the intrinsic factors. A lack of communication between the medical staff and the coaching staff was perceived as the most important or second most important risk factor in both subgroups.
The greatest difference between the two groups was the perception of style of coach leadership as risk factor, the group with higher hamstring injury rates (the HIGH group) perceived this factor as 57% more important compared with the teams with less hamstring injuries (LOW group). The HIGH group also perceived the player factors fatigue and wellness as more important compared with the LOW group. The LOW group, on the other hand, perceived a technical issue, the lack of regular exposure to high-speed football during training as considerably more important compared with the HIGH group (weighted average 3.8 vs 3.5).
Discussion
This study on modifiable risk factors for hamstring injury among professional football players revealed that CMOs from elite football clubs that had lower than average hamstring injury rates during two seasons, differed in their opinions on which risk factors are important and preventable compared with CMOs from clubs that had higher than average hamstring injury rates. The 15 CMOs included in the study felt that extrinsic (coaching, team, club) rather than intrinsic (players) factors were the most important preventable risk factors.
Lack of communication between medical staff and coaching staff
A lack of communication between the medical staff and the coaching staff was perceived as the most important or second most important risk factor in both groups.
We have previously reported an association between overall injury rates (not specifically hamstrings injuries) and the quality of internal communication at the club.21
Elite football clubs with good internal communication had fewer injuries and better player availability than clubs with poor communication.21
Communication between the head coach/manager and the medical team was vital for keeping players on the field.21 It is essential to communicate and discuss medical, performance and technical status to optimise individual training and match frequency.3 20 Mistakes happen when communication on prevention, regeneration, load management and rehabilitation breaks down. Management of minor injuries avoids larger injuries, and it is essential to have good communication and to have respect for minor injuries.21 22 Poor internal communication in a club lead to the coaching staff not receiving the necessary feedback they need to create an optimal football schema, and too tight a schema results in accumulation of fatigue.
Coaches are key persons
The greatest difference between the HIGH and LOW groups was the opinion on the leadership style of coaches. This is a prospective epidemiological survey, and this study design does not allow us to evaluate the reasons behind the data. However, based on 21 years of monthly contacts with these elite-level teams, we do have some hypotheses.
Our basic hypothesis is that the coaches are the most important persons for the injury situation in an elite club, medical staff can only realise suggestions for preventative training implementation across the whole team if the coach and coaching staffs are positive about the suggestions.6 23 24
We have previously reported an association between overall injury rate (not specifically hamstring injuries) and the leadership style of the main coach.25 Clubs with coaches that used a transformational or democratic leadership style had lower hamstring injury rates.25
One might speculate whether the teams with high injury rates in this study (the HIGH group) had the perception that the coaching style and communication between the coaches and the medical team was less good. Since the coaches at elite level also decide about load on players, this might explain the higher rating of load on players, fatigue and wellness among players as risk factors for injuries in the HIGH group.
Training/exercise surveillance by coaching staff
Surveillance with correction of conduction of training/exercise execution was included as one of seven preventative measures in the study by Ekstrand et al; the first RCT showing that it is possible to prevent sports injuries.26 Since then, the topic has hardly been investigated.
The CMOs in this study commented that training/exercises performed in an incorrect manner can be counterproductive, especially strength exercises. Diligent surveillance results in players performing exercises optimally, and coaches can change things when necessary. Engagement and surveillance by the coaching staff have more impact than surveillance by the medical staff. Disciplinary measures can be taken by coaching staff when players do not comply.
Is fatigue the underlying problem behind the perceived risk factors?
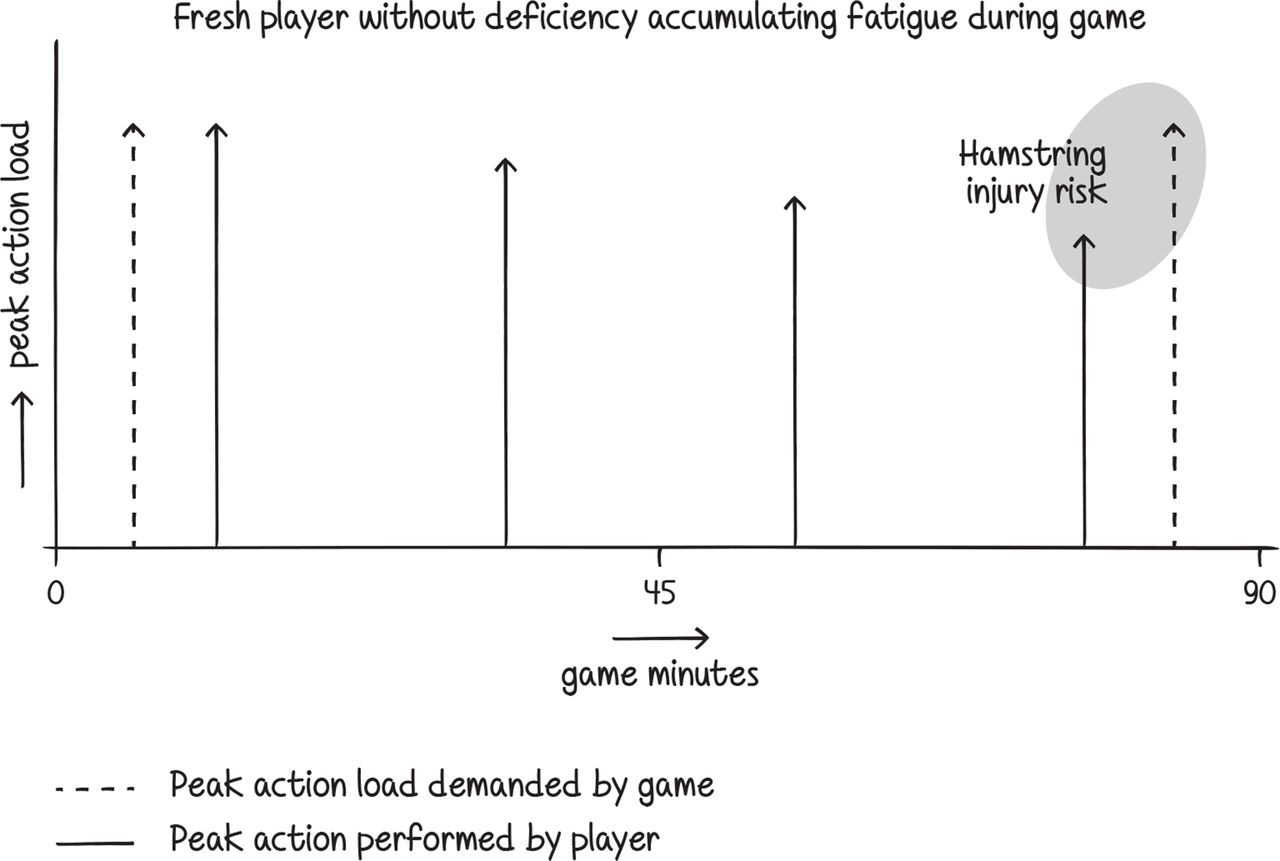
Fatigue is regarded as a major risk factor behind most hamstring injuries.6 10 12 27–30 Most of the risk factors perceived by CMOs (table 2) can be divided into two categories both of which lead to fatigue and consequently an increased risk for hamstring injury: (1) Excessive training/too many matches/overloading with subsequent accumulation of fatigue and (2) Too little specific training leading to muscle underloading. Dysfunction such as lack of eccentric strength, implies that load tolerance of the hamstrings is not good enough, and this may lead to either fatigue (injuries often appearing late in a match) or muscles not being prepared for match activity (injuries appear early in a match). Figures 1–4 illustrate a theoretical framework for the correlation between fatigue and muscle dysfunction, and risk for hamstring injury.

For a fresh player who begins a game with peak action performance and normal muscle function that corresponds to the loads demanded by the game, the risk for hamstring injury is minimal. However, as the game proceeds the player’s performance may not match loads demanded by the game due to fatigue and the risk for hamstring injury increases.

A player with fatigue accumulation due to excessive training/too many matches/overloading but still has normal muscle function begins a game with peak action performance that does not match the loads demanded by the game, and the risk for hamstring injury is already increased at the beginning of the game. As the game proceeds, the mismatch between loads demanded by the game and the player’s performance increases due to increasing fatigue, and the risk for hamstring injury increases even more.

A fresh player with muscle dysfunction such as lack of eccentric strength, will begin a game with peak action performance that does not match the load demand of the game and thus has an increased risk for hamstring injury already at the beginning of the game. However, due to increasing fatigue as the game proceeds, the mismatch between loads demanded by the game and player performance increases with consequent increase in the risk for hamstring injury.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
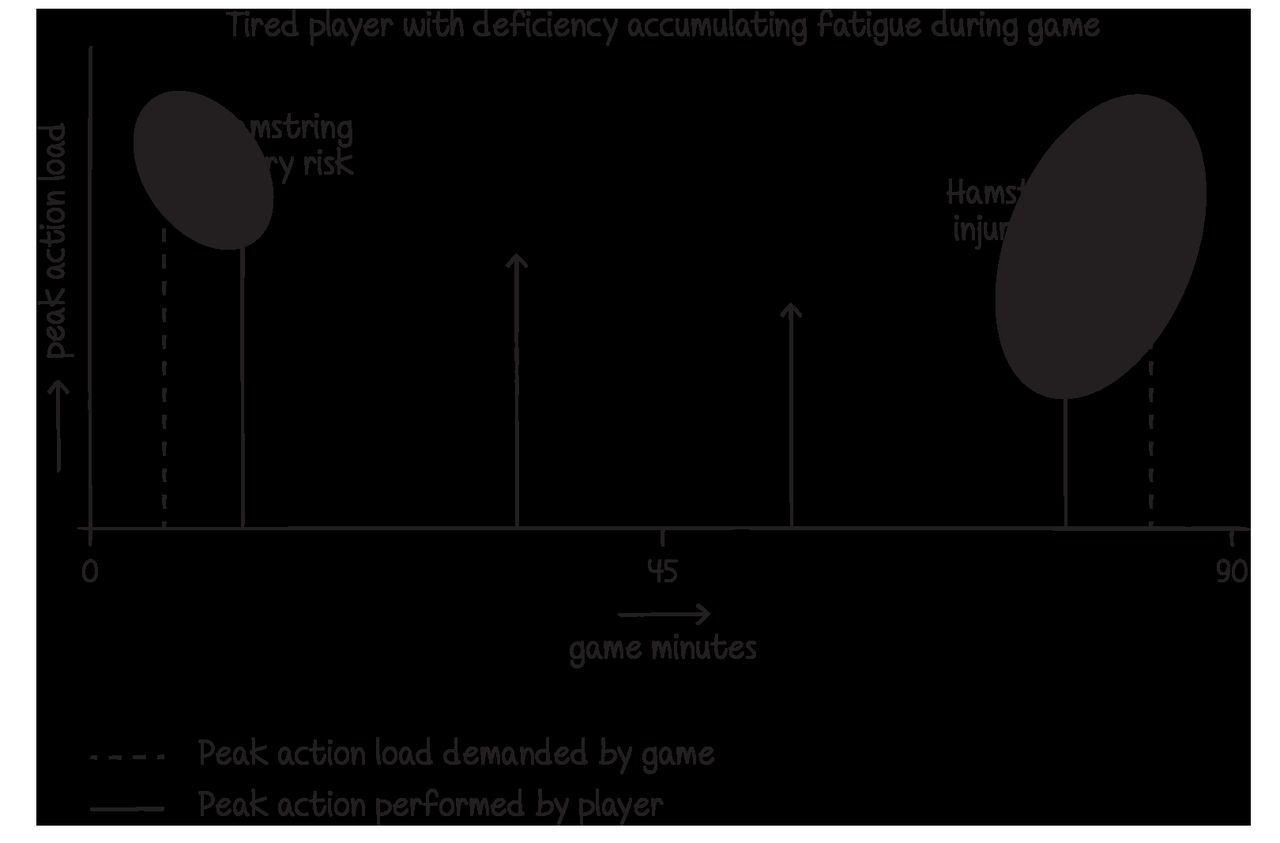
A player with fatigue accumulation and muscle dysfunction such as poor eccentric strength, will begin a game with a great mismatch between the performance and the loads demanded by the game, and the risk for hamstring injury is already high at the beginning of the game. As the game proceeds fatigue increases with an even greater mismatch between load demanded by the game and the player’s performance, and the risk for hamstring injury increases rapidly.
We have previously reported from the ECIS that muscle injuries occur more frequently toward the end of a match,2 6 or during/after a congested match period with little time for recovery.31 It has also been shown in simulated football studies that eccentric hamstring strength decreases with time, particularly during the second half of a match.17 30
These findings indirectly suggest an association between fatigue and risk for injury.12
It is suggested that fatigue leads to poorer neuromuscular coordination which potentially increases the risk for injury.12 26 When running fast, the primary role of the hamstring muscle group is active deceleration of the forward moving thigh and lower leg during the terminal swing phase.24 27 The terminal swing phase is considered the time when most hamstring injuries occur, due to high eccentric force contraction in the extended hamstrings when decelerating the leg.30 32
Fatigue is a combination of central (brain) and peripheral (muscle) fatigue mechanisms.12 33 It is believed that physical performance is largely affected by peripheral (muscle) fatigue whereas technical performance more by central (brain and neural) factors.33
Muscle fatigue can lead to injury situations due to poor control of muscles and joints or overloading/overstretching of muscles. Poor recovery from a previous load may increase the vulnerability of the hamstring muscle fibres to subsequent high intensity loads. Neural fatigue may reduce the player’s quality of play.30 Accuracy is reduced and ‘clumsy’ play can lead to the player injuring himself or an opponent.12 27 28 Reactions and speed of play are affected, the player is slower in controlling the ball enabling opponents to get closer leading to contact situations that increase the risk for injury.
However, despite common belief and studies indirectly suggesting that fatigue is associated with injury, scientific evidence supporting this theory is weak.19
In this study, the teams with high hamstring injury rates (the HIGH group) ranked fatigues as a considerably more important risk factor compared with the LOW group with less hamstring injury rates (ranking of importance 3.6 vs 2.6, see table 2).
The finding might be the consequence of the HIGH group teams having a lot of accumulated fatigue which in turn could be due to leadership leading to unbalanced training load, whereas in the LOW group teams there might be less accumulated fatigue, maybe because of a more balanced training load.
Accumulated fatigue is a consequence of unbalanced training which in turn might partly be due to the leadership style of the coach but also due to lack of knowledge in coaches about periodisation of load.
Off-season load/recovery
The off-season is a crucial period for physical and mental recovery,34 and detrimental changes in fitness may occur during this period.35 If players refrain from training during the off-season or take longer breaks in training, football fitness and muscle strength will decline increasing the risk for hamstring injury.34 So besides the necessary days off for recovery, it would be wise to also do some training in this period to remain football fitness and continue load on muscles and tendons. This especially counts for players who had less load in the previous season (for example due to injuries).
Furthermore, many top European clubs also devote part of the preseason to ‘‘promotional travel’’ which also reduces the number of days available for training especially when travelling through time zones, which causes more fatigue and therefore requires different training load in this period.36
Lack of regular speed training (high-velocity football)
The CMOs in the LOW team group (teams having less hamstring injuries) perceived lack of regular speed training as the most important risk factor for hamstring injury at the professional level. Hamstring injuries most frequently occur during sprinting and other high-velocity moves.14 Regular consistent exposure to high-speed play prepares the hamstrings for similar moves during games.20 34 Lack of sufficient high-speed play during training increases the risk for hamstring injury during games. Training should mimic match play in order to adapt the muscles to loads at matches.14 37 Training sessions should not only include basic action such as running or sprinting but should also include match-like situations where play depends on the football actions of opponents and the player’s response to those actions.14 28
Residual weakness after a previous hamstring injury
Previous injury is reported to be the most important risk factor for hamstring injury, but unfortunately this is a non-modifiable factor.6 10 11 13 38 However, residual weakness after a previous injury is modifiable. Both groups reported residual weakness after a previous hamstring injury to be the most important or second most important risk factor in individual players.
Insufficient rehabilitation (both strength and speed) results in lower load capacity of the muscle and puts it at higher injury risk during high-speed play.13 Furthermore, residual weakness after a previous injury may lead to muscle imbalance, increasing the risk of fatigue in the weak muscle.12 Studies suggest a change in neuromuscular control after a hamstring injury with lengthening of the muscle leading to falls in strength and EMG activation.39 40
Lack of regular strength training (eccentric/isometric/concentric)
Based on the assumption that hamstring injuries occur due to insufficient muscle strength,41 the CMOs stressed the importance of strength training to avoid muscle injury. Hamstring injury prevention should not only focus on eccentric strength training, but also isometric and concentric training, including combinations of knee and hip dominant exercises. There is some evidence that eccentric exercise can prevent hamstring injury,42 43 but there are few studies showing how other types of strength training can prevent hamstring injuries.19 41
What does this mean in practice?
If fatigue is the main risk factor and the reason for fatigue is either excessive training/loading or poor training, then focus should be on coaching team players at an optimal level. Cooperation and communication between the coaching staff and the medical staff are vital. It is the coach that decides on and leads football activities and the degree of loading of players, and they must be aware of the possible connection between hamstring injuries and fatigue, overloading and poor training. However, to optimise match/training and thus avoid fatigue, the coaches must be informed by the medical team and listen to the players.
Methodological considerations
A main strength of this study is that its design follows the international consensus statements and reporting guidelines for epidemiological research in sport.16–18
The study has limitations. First, hamstring injury, according to our inclusion criteria, comprises a heterogeneous group including structural (partial or total muscle fibre ruptures) and functional (no macroscopic muscle fibre disruption) injuries, with different foci and severity. Second, there may be different causes for acute or gradual onset hamstring injuries. This was not considered in the present study. The study is also limited by a relatively small sample size and a short observation period. The generalisability of the results from these 15 clubs to other high-level or semiprofessional clubs is unclear. Finally, as this is a descriptive study, we cannot infer any causality between expert opinions on risk factors and injury rates since the clubs may have differed regarding other risk factors for hamstring injury or confounding factors unknown to us.
Data availability statement
No data are available. The dataset from this study is held securely in coded form and data are not available to the public.
Ethics statements
Patient consent for publication
Ethics approval
Written informed consent was collected from all participating clubs. The study plan underwent an ethical review and was approved by UEFA.
Acknowledgments
The authors thank the participating clubs for their participation in the study. A special thanks to Dr Steve McNally, Manchester United and Dr Nelson Puga, Porto FC. Mrs Mirjam Kuipers is gratefully acknowledged for the design of the figures.
References
Footnotes
Twitter @wartvanzoest
Contributors JE was responsible for the conception of the study. JE and HB were involved in the data collection. HB conducted the analyses. JE drafted the manuscript, which was critically revised by the coauthors. JE is the study guarantor.
Funding This study was funded by grants from the Union of European Football Associations.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.