Article Text

Abstract
The objective was to increase understanding of how knee-injured people make sense of using the Motor Imagery to Facilitate Sensorimotor Re-Learning (MOTIFS) training intervention. This model integrates structured psychological skills training into existing care-as-usual (CaU) rehabilitation protocols. To better understand patients’ lived experiences of MOTIFS, it was necessary to understand those of CaU training. Interviews were conducted with five people undergoing knee-injury rehabilitation according to the MOTIFS model, as well as seven receiving treatment according to CaU. Interpretive phenomenological analysis was used to explore patients’ lived experiences. Results indicate that patients in the MOTIFS group perceive individualised meaning and sport relevance in their rehabilitation training. Imagery is perceived to be a concrete strategy that can be difficult, but encourages a biopsychosocial interaction to improve confidence, motivation, enjoyment and sport-relevant context, thereby aiding in physically and psychologically preparing patients for return to activity. CaU training is discussed in terms of physical factors, though patients identify psychological factors as important, perceiving a lack of focus on this, resulting in inadequate psychological readiness to return to activity. In conclusion, the MOTIFS model is perceived as focusing more on psychological factors in rehabilitation, helping to develop coping strategies and physically and psychologically prepare for return to activity. Patients in the CaU group perceive rehabilitation training as restoring strength and function, but lack structured psychological strategies to aid in return to activity preparation. This study is part of the MOTIFS randomised controlled trial (clinicaltrials.gov registration: NCT03473821).
- Knee injuries
- Rehabilitation
- Sport and exercise psychology
- Qualitative
Data availability statement
Data are available upon reasonable request. The data used in this study contains sensitive information about the study participants and they did not provide consent for public data sharing. The current approval by the Swedish Ethical Review Authority (DNR 2016/413; 2018/927) does not include data sharing. A minimal data set could be shared by request from a qualified academic investigator for the sole purpose of replicating the present study, provided the data transfer is in agreement with EU legislation on the general data protection regulation, GDPR and approval by the Swedish Ethical Review Authority.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Approximately half of all knee-injured athletes are unable to return to their preinjury level of competition, and one-third are unable to return to their preinjury level of activity.
The role of physical factors for return to sport and physical activity has been explored in detail, but recently, psychological factors such as motivation, self-confidence and fear of reinjury have been shown to be important for preparing for return to activity.
Psychological readiness to return to activity is low, with few interventions specifically designed to target these factors by clinicians in a real-world clinical setting, despite recommendations to consider psychological factors in rehabilitation training.
The novel Motor Imagery to Facilitate Sensorimotor Re-Learning (MOTIFS) training model has been developed as a method of integrating psychological training into physical training to influence patient-reported outcomes.
WHAT THIS STUDY ADDS
This interview study examines patient perspectives of rehabilitation, highlighting the need for individualised and patient-centered treatment that is relevant and meaningful to prepare for return to activity.
Patients receiving MOTIFS rehabilitation describe using structured psychological training methods in order to directly target psychological aspects with which they struggle throughout the rehabilitation process.
Patients receiving care-as-usual rehabilitation perceive a low degree of psychological training and report not receiving any tools to cope with what is described as a very important factor in rehabilitation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Results of this study indicate that patient readiness to return to activity can benefit from an intervention which integrates structured psychological skills training into rehabilitation exercises. This represents a plausible method of providing physical therapists (PTs) with the necessary skills to provide patients with coping strategies. The significance of the PT as a source of support is important, as it highlights the necessity of effective communication skills, and building trusting relationships through patient involvement in rehabilitation planning.
Introduction
Traumatic knee injury is common in both competitive and recreational physical activities. Rehabilitation typically includes physical training to restore function to injured and surrounding structures using neuromuscular and strength training.1 2 Despite best-evidence treatment, approximately 45% of injured athletes are unable to return to their preinjury level of competition3 and roughly half display persisting impairments in function.4 5
Best-practice guidelines recommend also addressing psychological factors.2 Higher motivation, optimism, self-confidence and lower fear of reinjury have been suggested to increase the likelihood of successful rehabilitation outcomes, such as return to activity.6–8 There are, however, few structured interventions aiming to improve psychological aspects of rehabilitation,9 though the literature has called for a more thorough exploration of potential strategies.10
We have proposed and are currently evaluating the Motor Imagery to Facilitate Sensorimotor Re-Learning (MOTIFS) model, a novel approach to rehabilitation in which psychological training principles are integrated into physical training exercises.11 12 Dynamic motor imagery (DMI) is a form of psychological skills training in which one simultaneously mentally and physically simulates an individualised, activity-specific situation.13 MOTIFS integrates DMI into care-as-usual (CaU) exercises using a set of principles in which the physical therapist (PT) and patient (1) discuss and (2) design an exercise integrating physical and psychological situation-based realism, then (3) execute a meaningful rehabilitation movement and finally (4) evaluate and modify to ensure realism and relevance.11 Compared with CaU training, this model has been shown to increase enjoyment and feelings of control in uninjured athletes.12 An ongoing randomised controlled trial (RCT) hypothesizes that a 12-week MOTIFS intervention will increase psychological readiness to return to activity and improve muscle function to a greater degree than CaU rehabilitation for traumatic knee injury.11
Few studies have explored lived experiences of patients undergoing rehabilitation for knee injury,14 so a qualitative study may provide valuable information to inform current rehabilitation practices. Interviews with knee-injured people can provide a deep and nuanced understanding of rehabilitation experiences and meaning making, providing important information on more holistic strategies.
The aim of this phenomenological interview study was therefore to explore and gain insight into the lived experiences of knee-injured people undergoing rehabilitation following traumatic knee injury using the MOTIFS training model. In order to do this, it was necessary to also gain insight into the experiences of patients who have undergone CaU rehabilitation, so that the context in which MOTIFS training is perceived can be better understood.
Methods
Study design
This phenomenological interview study is part of the MOTIFS RCT (clinicaltrials.gov registration: NCT03473821),11 reported according to Consolidated Requirements for Qualitative Research15 (online supplemental appendix 1) and Standards for Reporting Qualitative Research.16
Supplemental material
Participants
Eligible participants were men and women 16 years or older undergoing or having recently completed PT-supervised rehabilitation for traumatic knee injury and with a goal of returning to physical activity. Participants were purposively sampled from those that had completed participation in the MOTIFS RCT in southern Sweden11 and recruited by telephone. Interviews were conducted with n=5 patients from the MOTIFS group and n=8 from the CaU group (table 1; online supplemental appendix 1). Analysis was performed on n=5 MOTIFS and n=7 CaU interviews, as the research team had reached consensus regarding data saturation, defined as two new interviews not significantly altering the conceptual model.17 18
Demographic information of interviewed patients from the MOTIFS and care-as-usual conditions
Participant and public involvement
Clinically active PTs and patients were involved in providing input and feedback on MOTIFS exercises during the planning phase until the model was finalised; PTs aided in development of eligibility criteria and outcomes. This interview study provides an opportunity for end-user (ie, patient) feedback on and evaluation of CaU and MOTIFS rehabilitation. End users were not involved in recruitment to, nor dissemination of, results of this study nor the RCT.
Data collection and analysis
Patients received verbal and written information and provided demographic information and informed consent, both written and verbally. Digital interviews conducted by the first author (NC, male doctoral student with interview training and experience and expertise in sport psychology) between February 2021 and February 2022 were recorded and stored on a secure server. No non-participants were present, no interviews were repeated and participant transcript or conceptual model review was not deemed necessary. Pilot-tested questions included one to prompt recall of rehabilitation (ie, ‘who was your PT?’)19 and one open-ended question, asking patients to ‘describe in as much detail as possible how you experienced the rehabilitation process.’ Follow-up questions, based on interview notes, ensured thorough responses (ie, ‘can you elaborate on…’ or ‘what do you mean by…’).
Coding was done according to coding reliability thematic analysis approach20 grounded in interpretive phenomenological analysis (IPA), which decodes, interprets and identifies unique individual aspects of a phenomenon.19 The primary coder (NC) transcribed anonymised interviews verbatim and inductively coded according to IPA using QSR International’s NVivo qualitative data analysis software (released March 2020).21 Coding comparison was done following deductive coding by coder 2 (SG, expertise in psychology), then coder 3 (EA, expertise in physical therapy) when intercoder agreement was acceptable. Rigour was thereby established with thorough reading of the material, interdisciplinary expert opinion and subsequent agreement and reliability analyses.22 A detailed description of data processing is available in online supplemental appendix 1.
Results
Two separate conceptual models are presented, one each for patients in the MOTIFS and CaU groups in order to clarify the context in which MOTIFS training is perceived, and not to compare differences. Themes are presented in descending order of prevalence, from most to fewest references, and are marked in accordance with the corresponding figure, which shows major and more detailed subordinate themes. Selected participant quotations are presented in text as (P#) in order to illustrate the complex reality of participant experiences in the context of the generated conceptual models. Themes with fewer than three references are specified to indicate that they may not represent a distinct pattern.
Motor Imagery to Facilitate Sensorimotor Re-Learning
Three major themes were identified from patients in the MOTIFS group (figure 1):
‘Rehabilitation training is strongly influenced by psychological factors’: patients described psychological responses to injury and/or rehabilitation, including both positive and negative factors, and perceived concrete strategies to influence these.
‘Interaction between biopsychosocial aspects of injury and rehabilitation training’: physical and psychological factors were perceived to interact, in which physical, psychological and social aspects influenced one another during rehabilitation.
‘Physical rehabilitation aims to prepare patients for return to activity’: patients described perspectives on physical aspects of rehabilitation, including readiness to return to activity, and treatment and/or interventional strategies.
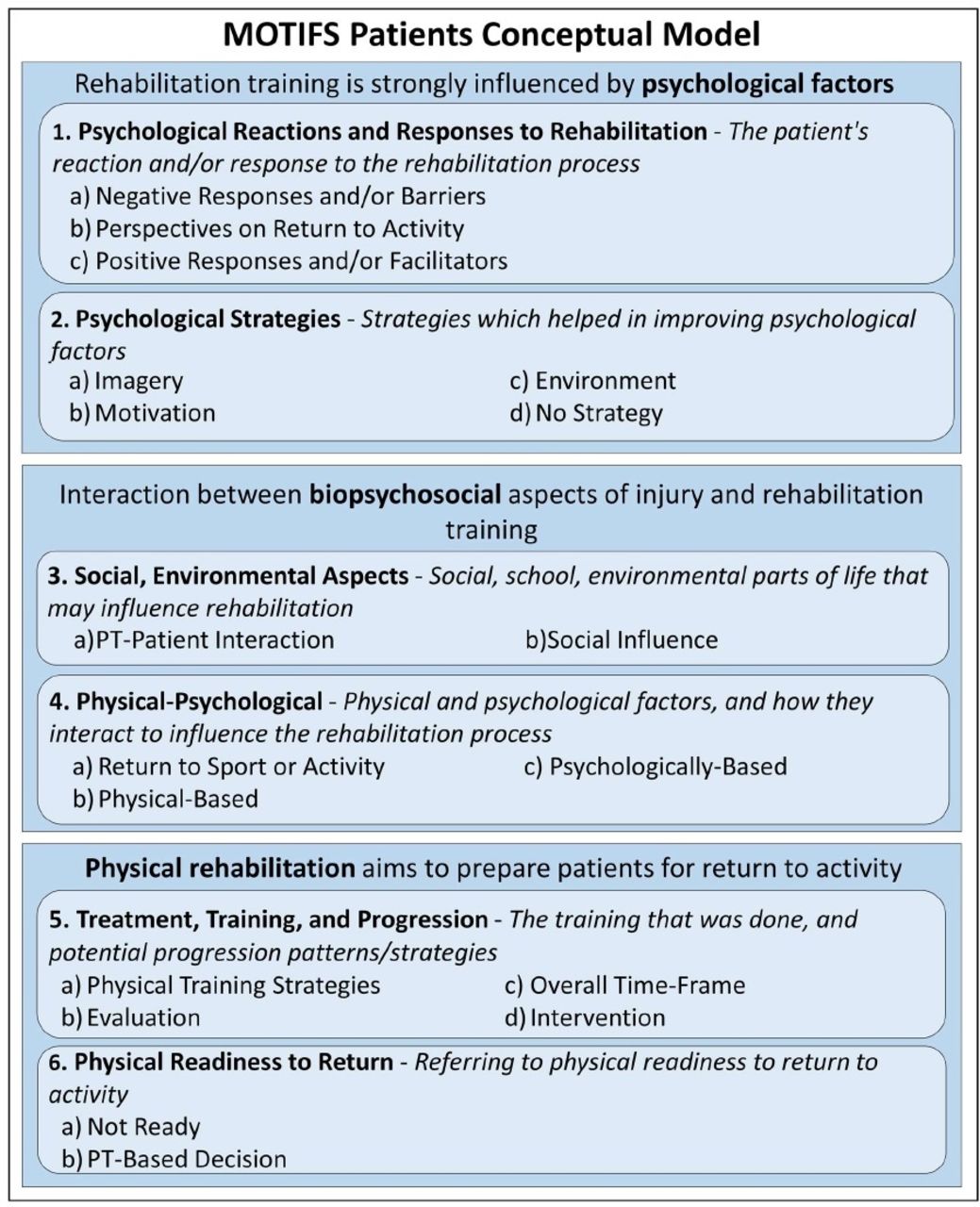
Conceptual model generated from interview responses of patients in the Motor Imagery to Facilitate Sensorimotor Re-Learning (MOTIFS) group including major and more detailed subordinate themes. PT, physical therapist.
Major theme: ‘Rehabilitation training is strongly influenced by psychological factors’
Patients described psychological aspects, providing unique perspectives on rehabilitation training, as those in this group were speaking from the experience of using MOTIFS training. Patients referred to psychological reactions and responses to rehabilitation, characterised by perceptions and feelings which arose as a result of training-related factors. Negative responses or barriers (figure 1—MOTIFS 1a) were described as the hardest part, resulting in a negative physical self-image, which may have resulted in feeling "totally handicapped" (P03). Absence from activity ("I’ve been away from floorball for so long, you almost forget how it can be" [P01]) and a lack of enjoyment and motivation ("certain times can feel hard and unmotivated and boring" [P04]) were perceived causes of this. Fear was also a perceived barrier to psychological readiness ("You were afraid for your knee, so it was hard to get into like, soccer-mindset. It was more, like, 'don’t step wrong-mindset’"[P10]). These results indicate that rehabilitation constitutes a negative change from patients’ usual lives.
Patients also discussed perspectives on return to activity (MOTIFS 1b), including feeling "scared for my knee. That the same thing will happen again" (P02). Desire to return may depend on perceived significance of the activity, as one participant described feeling "such freedom when I play soccer" (P02), and others perceived enjoyment and athletic identity as strengthening their desire to return to activity ("floorball has been such a big part of my life […] so I chose to fight my way back" [P01]). This implies that psychological aspects play a large role in determining how a knee-injured person views returning to activity following an injury.
Undergoing rehabilitation training also included positive responses and facilitators (MOTIFS 1c) to completing rehabilitation training. One participant perceived rehabilitation as a "kind of a social thing, too" (P04), possibly resulting from having a common focus on using MOTIFS to create sport-specific rehabilitation ("we were very focused on soccer, there were […] a couple others that were also soccer players" [P10]). Another believed self-confidence facilitated training and alleviated psychological barriers, because discussions with the PT in MOTIFS training provided evidence that "I’ve made it once, so I can do it twice, so [rehabilitation] is nothing scary" (P01). Positive motivation was psychologically important to rehabilitation compliance, as MOTIFS clearly connects to participant desires and interests ("I’ve always known I could […] go far in soccer. So I’ve never doubted- I know I have to give 100% [in rehabilitation]" [P10]). Patients indicated that, despite changes from normal preinjury physical and psychological states, rehabilitation included positive aspects which aid in encouraging effective rehabilitation training.
Psychological strategies were described that alleviated negative reactions and/or strengthened positive reactions. Using MOTIFS to integrate imagery was a psychological strategy (MOTIFS 2a), perceived as new and sometimes difficult, because imagery requires that one "really […] think about how you do things, like how I normally do it on the field’"(P03). One participant clarified that imagery gets easier over time and two "thought it was fun" (P10). Imagery was implemented using "a stick and a ball in the [clinical] environment […] to get into the mindset of ‘this can happen on the floorball court,’ and to see it in front of me" (P01) in order to "practice in my mind, […] so I get myself to the right place at the right time and play smart" (P10). Patients perceived that imaging sport-specific movements created training which was "specific to floorball […], so you could definitely say that [MOTIFS] is preparation to play for real again, with these exercises we’ve done with different directional changes" (P04).
Goal setting in connection with MOTIFS training was perceived to positively influence motivation (MOTIFS 2b) through goal-directed and activity-specific discussions ("in a month I’ll be able to run, in a month I can play floorball" [P01]; "I’m reminded all the time of why I am doing [rehabilitation]" [P01]). Two patients saw on-field MOTIFS training as an environmental psychological strategy (MOTIFS 2c), which provided a method of coping with difficulties. Having no strategy was a possibility (MOTIFS 2d), with one participant describing that "I didn’t really have any strategy not to think about it, because [the knee] was always reminding me" (P03) in the beginning of rehabilitation. However, MOTIFS exercises were "more similar to sport than the [CaU] exercises were. And then – you got to feel it – handball – in some way, even though it wasn’t for real" (P03), leading to a perception that MOTIFS "prepar[ed] me more than I think I normally would" (P03). Overall, MOTIFS training was perceived as a method of preparing for return to activity.
Major theme: ‘Interaction between biopsychosocial aspects of injury and rehabilitation training’
When discussing rehabilitation, patients clearly referred to the way in which physical, psychological and social factors are inter-related. This resulted in conceptually different perspectives than either physical or psychological reactions.
Patients indicated that both psychological and physical factors can be influenced by social and environmental aspects in their lives. PT-specific interactions (MOTIFS 3a) during MOTIFS training were important because PTs "were fun and they could joke around, and it wasn’t just like ’doctors’ […], it was fun" (P10). Support such as adapting communication and knowledge transfer strategies using "the simple names, so to speak, not those complicated names, […] like Greek names" (P02) influenced physical and psychological aspects of rehabilitation. This was perceived to help manage rehabilitation expectations, understanding that "this is what’s going to happen in a few months, next time we’ll do this" (P01) and connected them to the PT and exercise design ("because [PT] has also played handball, so we discussed, like, what are- what kind of situations can happen" [P03]). Participant responses highlighted the important impact the PT had on physical and psychological rehabilitation experiences.
Patients experienced other sources of social influence (MOTIFS 3b), perceived as coming from friends and family "that have said like ‘you’ve come so far, so you have no reason to give up’" (P01), which can impact training quality or frequency. However, negative support also occurred ("[my teacher] said if you want to continue with soccer and if something happens to your knee again, it’s not going to be like before. You might not even be able to work." [P02]). This shows that a person’s social network, including PT, sport and private life influences, can impact rehabilitation perspectives and behaviours.
Two patients felt that sport-specific MOTIFS training provided necessary physical and psychological return to sport or activity (MOTIFS 4a) preparation ("you don’t get the same feeling [in CaU], and then you maybe don’t do it in the same way." [P03]; ‘"[MOTIFS] helps more in the head, to get back in the mindset […], it’s helped both physically and mentally’"[P01]). MOTIFS integrates activity-specific rehabilitation training, which "helped me think back on it and actually get into those situations, and also prepares my knee" (P01). Patients suggested a need to rehabilitate sport skills by training "individual technique, and a little that you need to get back that you have lost during the injury period" (P01). Physical-based factors (MOTIFS 4b) including exercise difficulty ("some sessions were a little bad because it was hard to do them" [P02]; "I liked it because it was challenging" [P10]) and pain may have influenced rehabilitation perceptions ("I’ve been limping the whole time, so it has always been a reminder" [P02]). Psychologically based factors (MOTIFS 4c) were also perceived to influence rehabilitation, including frustration and reduced confidence because "you know that you can do things - I can walk, I can extend my leg, but then it, like, doesn’t work" (P03). However, progression increased trust in one’s knee ("after a while, I see that my knee is pretty good, it’s holding well" [P02]). This theme indicates that patients are aware of the interaction between psychological impacts on physical training and that they perceived that MOTIFS training addressed this.
Major theme: ‘Physical rehabilitation aims to prepare patients for return to activity’
Rehabilitation was described as including a significant physical aspect, and patients discussed their thoughts on this. Patients perceived treatment, training and progression as including physical training strategies (MOTIFS 5a) focusing on range of motion ("bending the leg and extending the leg" [P03]), strength ("a bench that you lay on and just try to lift up your hips" [P10]) and hop ability ("jumping sideways, jump for distance" [P04]). The chosen strategy was perceived to be determined by evaluations (MOTIFS 5b), including discussions of symptoms ("how was it with your knee while you were sleeping and stuff" [P02]), and one participant described evaluations of side-to-side differences "in my hamstrings that should be a certain percent of the other hamstrings" (P04). Progression was perceived as being unclear in terms of overall timeframe (MOTIFS 5c), but could include prehabilitation exercises ("strength training to build up the muscles before – since it was a little uncertain how long it would take to get the operation" [P04]). Other interventions that were perceived to help regain function were described, (MOTIFS 5d) including orthotics ("I got one of these, like, robot legs, a brace" [P03]), cortisone, and operation. One participant described a lack of physical readiness to return (MOTIFS 6a), citing lack of physical ability and symptoms ("sometimes I have a clicking sound in my knee" [P02]), which relied in part on the PT’s opinion (MOTIFS 6b).
Care as usual
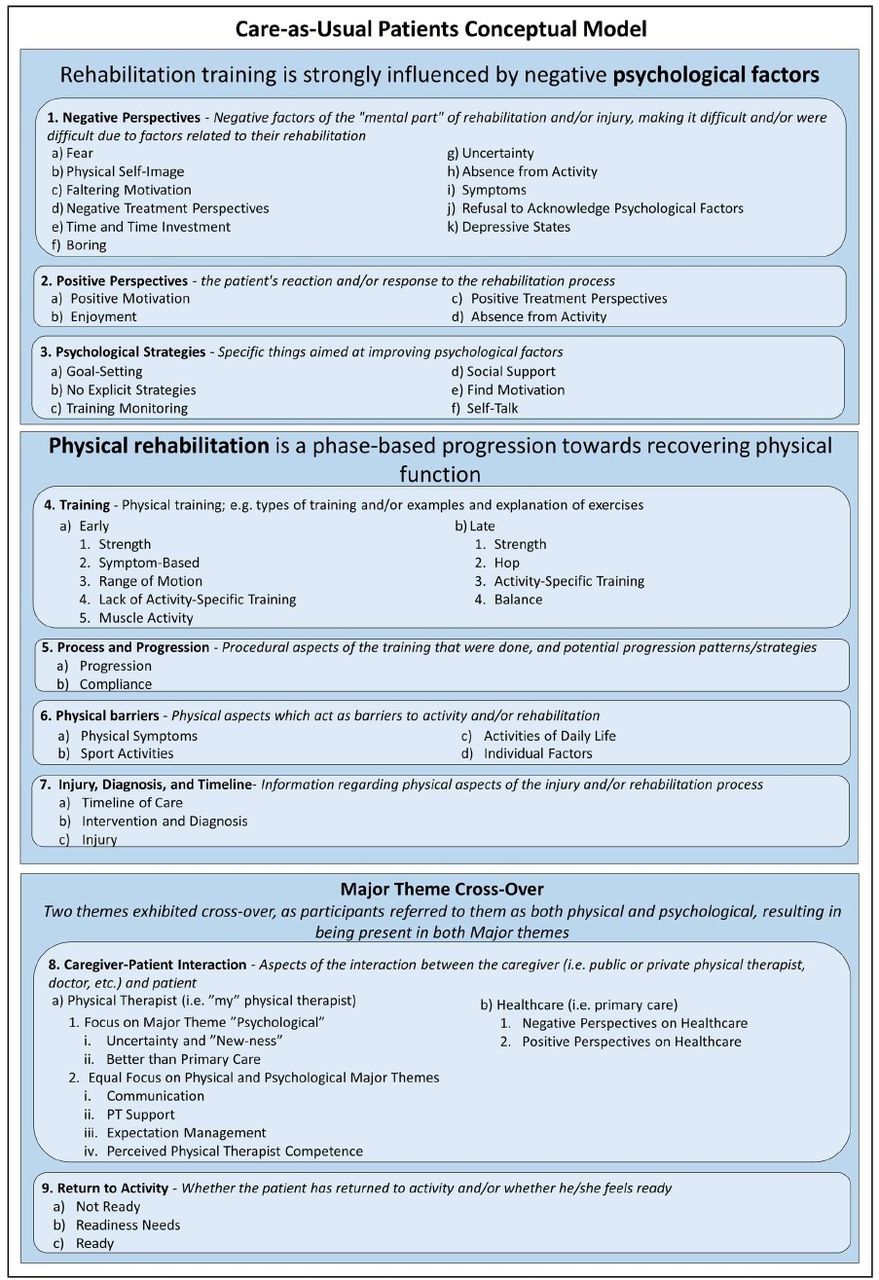
Two major themes were identified from patients in the CaU group (figure 2):
‘Rehabilitation training is strongly influenced by negative psychological factors’: patients perceived positive and negative psychological perspectives and described strategies used to address these.
‘Physical rehabilitation is a phase-based progression towards recovering physical function’: patients described their rehabilitation training and progression, as well as perspectives on physical barriers and the injury itself.
{kind=link}
{kind=link}
Conceptual model generated from interview responses of patients in the care-as-usual group including major and more detailed subordinate themes. PT, physical therapist.
Two themes (‘return to activity’ and ‘caregiver–patient interaction’) exhibited cross-over between both major themes, resulting in separate presentation of these themes. An interesting aspect of this conceptual model is the reflection of participants’ lived experiences of rehabilitation as being characterised by dualistic descriptors rather than articulating a holistic interaction between physical, psychological and social aspects.
Major theme: ‘Rehabilitation training is strongly influenced by negative psychological factors’
When discussing negative perspectives on rehabilitation, negative factors and rehabilitation barriers were described. Fear (figure 2—CaU 1a) and reinjury anxiety ("I know I have arthritis in my knee. I know that the more times I injure myself, the closer I get to getting a knee replacement" [P08]) were perceived to negatively influence return to activity:
it will of course be scary to start playing soccer again. I’m not going to sit here and say anything else… because it is the psychological part that will mostly… put a stop to going into a duel
(P06)
Negative physical self-image (CaU 1b) and faltering motivation (CaU 1c) were perceived to be a result of lack of progress ("I had to get to know [my knee] again. Both how it looked, because it was so thin [laughing] but mostly how it worked" [P11]; "it’s pretty hard to see a light at the end of the tunnel" [P12]). Negative treatment perspectives (CaU 1d), such as boring exercises (CaU 1f) resulted from being "extremely basic when you just- when you like extend and lift a leg, it feels like ‘this is nonsense’" [P08]). The subsequent frustration and lowered motivation may be due to uncertainty (CaU 1g) resulting from inadequate guidance, because "it’s pretty much my feeling. And who knows if my feeling is right" (P08). It may also be due to absence from activity (CaU 1h), because "I found other sports that I thought were really fun. (…), but that I couldn’t participate in fully because I was like waiting for my knee to be good enough" (P11), suggesting symptoms (CaU 1i) were barriers ("I still feel it now when I work, too, […] I feel a bit of cartilage and stuff" [P12]). One participant described refusing to address psychological factors (CaU 1j), feeling that negative psychological reactions "didn’t exist for me, I thought 'that’s for other people, but it won’t get me'" (P07). Others perceived feeling "super depressed" (P05; CaU 1k). The overall negative perceptions suggest that this is a dominating factor which influences rehabilitation experiences.
Positive perspectives on rehabilitation included motivation (CaU 2 a) and self-confidence, perceived as helpful because “you know that, if I just keep training well enough like this- it will work out” (P06). Positive perspectives can also include enjoyment (CaU 2b) and overall positive treatment perspectives (CaU 2c) including that it "felt good" (P05). One participant believed "it was also kind of nice to get away from [sport] a little bit" (P07; CaU 2d). These results indicate that patients recognise the importance of psychological factors in influencing perspectives on rehabilitation.
Patients perceived using self-initiated psychological strategies including goal setting (CaU 3a), while others had no strategy (CaU 3b), claiming that "you never get any tools for the mental bit" (P08). Training monitoring (CaU 3c) and social support (CaU 3d) were described as strategies to find motivation (CaU 3e) and set training goals ("jogging, that’s been [the goal] – when you look at where I need strength and stability" [P08]; "it was more and more fun, and you felt that you got the leg going and you got stronger" [P12]). However, one participant "didn’t think [monitoring] gave so much" (P05), resulting in giving up that strategy. One patient also described using self-talk "to convince myself that [my knee] will hold […] you try to- I don’t know… push it in your head that you can do these things" (P08). Patients perceived the importance of being able to influence psychological factors, but the strategies are vague and vary in their efficacy.
Major theme: ‘Physical rehabilitation is a phase-based progression towards recovering physical function’
Patients described a perspective that training followed a phase-based progression. Early phases (CaU 4a) included muscle activation, range of motion and strength training, in order to "feel that the leg could do something, […] that there was some connection between my head and the knee" (P11) and includes "a lot […] leg exercises, like in machines and stuff" (P07). Later phases (CaU 4b) included hop and strength training ("(h)exbar was one, Bulgarian split squats was one" [P06]), with two patients doing balance training. Training intensity and movement type became "more intensive, finally full running […] a lot of rushes forwards and fast braking" (P12), seen as increased activity–specificity.
The rehabilitation process and progression (CaU 5a) was perceived to be determined by evaluations, including strength or cutting movements to "test things more towards soccer" (P07). Compliance (CaU 5b) to PT-supervised training was thought to ensure proper execution ("the stuff that was challenging we did in the clinic" [P06]), but may lack sport specificity and variation ("When we were going to adjust something ([…)], then we just increased weight, or that I hopped a bit further. But the exercises didn’t change very often" [P09]). These results may indicate an understanding of the physical requirements and goals of rehabilitation training.
Physical barriers to rehabilitation were perceived to include physical symptoms (CaU 6a) such as swelling, fatigue and pain ("when I get winded […] I feel that I have pretty bad control of my knee" [P07]), and two patients perceived limitations in sport and daily life activities (CaU 6b and c), feeling that "I haven’t been able to do anything, until the end when you can start passing a little" (P06). One participant felt limited by pre-existing individual factors (CaU 6d). Patients referred to the injury, diagnosis and timeline of rehabilitation ("I waited almost 6 months for my operation" [P12]; CaU 7a–c). These physical barriers indicated a focus on negative factors of rehabilitation over which patients may feel little control, possibly resulting in feeling helpless regarding these.
Major theme cross-over
Two themes were determined to exhibit cross-over between psychological and physical themes. This resulted from discussions of both physical and psychological concepts without explicitly distinguishing between them.
A positive caregiver–patient interaction was perceived as important, showing whether the PT (CaU 8a) cared and communicated well ("[PT] has had other patients at the same time, so I’ve trained mostly alone. […] I feel like I’ve been there and done what I was supposed to, but I didn’t get the right follow-up on it" [P08]; "they did a really good job and tried to give me as much information and stuff as possible" [P12]). This helped return to sport expectation management, which "is nothing we have discussed in depth, it’s just 'when can I start playing?’" (P06) and increased perceived PT competence and feeling "safe because I felt in some way like he knew his stuff" (P09), leading to positive perceptions. One participant perceived primary care (CaU 8b) as disappointing ("I met a newly graduated physical therapist and the first thing he says to me is ‘oh, you’re my first knee patient, how exciting!’ How trust inspiring [sarcastically]" [P05]). The importance of this interaction was seen as physically and psychologically important, but patients did not express a distinction between these aspects, possibly indicating they did not consciously make this connection.
Not feeling ready to return to activity (CaU 9a) included acceptance of replacement activities due to changing perceived activity-specific abilities and need fulfilment ("I don’t need to play soccer. Partly because I don’t have time, and I don’t miss it as much because I’ve found another sport that fits me just as well" [P09]). Readiness needs (CaU 9b) included time, exposure or regaining skills and confidence ("[PT] tried to find situations that I thought were scary. And then challenged me quite a bit in those situations" [P11]). Two patients distinguished readiness to return to their specified activity from other activities, citing expertise as a factor:
we […] are beginners, so there’s not the same tempo in paddleball. […] And my knee can handle that. And soccer I’ve played long enough that, and I, I have always lived on my quickness, so it’s, it’s a lot more- a lot harder, quicker loading. […] If I were a good paddleball player, I don’t think that would work for me either.
(P07)
Patients perceived readiness to return to activity as both physical and psychological, with one referring to feeling ready (CaU 9c) "as soon as I get the OK" (P05), suggesting PT dependence. These results suggest that patients desired activity, but accepted an inability to return to their preinjury activity.
Discussion
Patients in the MOTIFS group experienced rehabilitation as having negative aspects due to the change from normal and subsequent limitations. However, integrating psychological training into rehabilitation was perceived to provide strategies to cope with both physical and psychological difficulties, and patients indicated feeling psychologically prepared to return to activity. The CaU group described rehabilitation as including physical training with a negative psychological component, for which they lacked explicit coping strategies.
MOTIFS group
Psychological
Best-practice guidelines suggest addressing psychological factors in rehabilitation by evaluating changes,23 providing support, setting goals and mental practice,2 with educational interventions being beneficial.24 The MOTIFS group addressed psychological factors using MOTIFS training, which uses motor imagery to integrate physical, environmental, task, timing, learning, emotions and perspective25 into rehabilitation exercises. Patients described the strategies of using equipment and imaging sport-specific situations in order to create individualised meaning, confidence and enjoyment, which is in line with previous research on motor imagery.12 26 In creating this imagery situation, one is also naturally simulating a connection to technical, tactical and social aspects of sport, which is reflected in the major theme biopsychosocial. This suggests motivation and goal-setting strategies based on autonomy, competence and relatedness, consistent with self-determined motivation.27 Patients see MOTIFS training as a method of preparation for return to activity in which they are able to get exposure to real-world situations in a safe environment prior to return, consistent with previous research indicating that trust in knee function28 and confidence in performance8 impact psychological readiness. This can include development of tactical or technique modifications to facilitate confidence and reduce risk-taking behaviour on return.29
Positive psychological aspects such as self-efficacy and motivation are perceived as being important, which has support in previous research.6 The fact that they were training sport-specific skills was described as being enjoyable, indicating that patients perceive meaning and fun to be important aspects of rehabilitation training. This may thereby improve motivation and confidence in sport-specific situations, in turn influencing both physical and psychological readiness to return.
Overall, patients indicated that negative psychological aspects of rehabilitation were more dominant. Given the desire to return to activity, not being able to participate at the same preinjury level or not being allowed to progress can lead to boredom and loss of motivation. This reduction in physical ability can result in a negative self-image which may explain fear of reinjury (eg, fear of the pain of injury) and reinjury anxiety (eg, fear of needing to undergo an operation or rehabilitation again) reported in this study and is supported in previous research.8 14 30 This can be due to uncertainty of safe levels of activity, which can increase likelihood of avoidance behaviours.31 Therefore, information from the PT which includes effective communication of risk factors in a manner adapted to the needs of the participant was perceived as beneficial.
Biopsychosocial
Rehabilitation includes significant overlap between physical and psychological factors, and current recommendations include a biopsychosocial approach to rehabilitation.32 Patients in the MOTIFS group seemed to understand, and expressed distinct opinions about, these nuanced facets of training. They describe goal-directed sport-specific training as a means of preparing both physically and psychologically for return to activity. This includes interactions with the coaches and team, as well as through sport-specific interactions with the PT. Other social interactions can include from friends and family, for example, encouraging them to continue with the rehabilitation. Interestingly, the MOTIFS group implied a need to rehabilitate sport skills in reference to having lost sport-specific experiences or ability, and not only restoring function to injured structures. The implication is that physical aspects need to be trained, but without meaningful psychological connection, the sport skill will still be behind on returning to sport, thereby hindering physical and psychological readiness to return to sport.
Physical
Patients described exercises and evaluative tests which correspond to those ACL injury treatment recommendations,2 23 33 indicating that PTs prescribed appropriate exercises, and that patients were able to understand their relevance and purpose. This lends support to the finding that the PT’s judgement and expertise are important in shaping perceptions of one’s own physical readiness.
CaU group
Psychological
Return to sport goals were discussed by the CaU group, although vaguely as an overall desire to return, as opposed to activity-specific goals.34 The lack of specific strategies may indicate inadequate psychological competence and relatedness, potentially resulting in lower motivation.35 A lack of competence may include being unaware or unable to use strategies, which could be a result of not thoroughly discussing with the PTs or coaches, for example, and therefore lower understanding of real-world (ie, sport- or activity-specific) applications. This may explain patients’ questioning of the efficacy of strategies such as self-monitoring or goal setting, and some stopping altogether. Other psychological strategies described by the CaU group include self-talk, pressuring oneself to ‘find’ motivation and setting goals in very broad terms. No specific information was provided on how these can be done effectively to positively influence rehabilitation training or resulting psychological states. Interestingly, taking a break from sport was discussed as a positive factor by one participant, potentially indicating a motivational shift away from return to activity, as motivation and goal setting were said to be related to rehabilitation progress, with return to sport a more abstract desire. Patients also perceive that self-efficacy and motivation are important aspects to rehabilitation, reflecting on the fact that the addition of more sport-specificity would be beneficial to increase enjoyment and overall rehabilitation experiences.
Patients in the CaU group echoed the sentiment that negative psychological factors played a significant role in rehabilitation. These negative aspects were a large focus in the CaU group, as they expanded on these perspectives, referring to depressive states and an instinct of avoidance and denial regarding psychological factors. This could be a further indication of inadequate psychological preparation and understanding, which has previously been shown to be important for recovery.14 Patients describe the information from the PT regarding psychological factors as focusing largely on physical effects. This includes the fact that movement execution may be hindered due to psychological responses which result in maladaptive physiological responses (ie, stiff-legged landing mechanics), and re-establishing the connection between the brain and injured limb.
Physical
Patients in the CaU group also described exercises and evaluative tests in line with current recommendations.2 23 33 In this group, patients are able to understand exercises which are relevant to their injury. However, they specifically refer to early and late phases, and the sport specificity included in each phase. This may point to an overly physical focus on phase-based training, which may take away from the ability to reflect on sport relevance and ascribe more importance to the exercise themselves, rather than to the real-world application of these exercises.
Cross-over
The CaU group discussed physical and psychological factors, though the distinction was not clear, seeming to refer to both at once. This resulted in cross-over between physical and psychological major themes.
Communication of physical factors by the PT, but not psychological factors, seemed to be effective in the CaU group, which resulted in positive perceptions of PT confidence. A potential problem with this is the dependence on PT confirmation of physical readiness, as opposed to autonomy and competence in feeling this themselves. This may explain the patients’ feelings that expertise can play a role in readiness, which has been shown to be a risk factor.36 They express a desire for more sport-specific training to increase enjoyment, shown to influence physical activity behaviours in non-injured people.37 38 The PT- reliance and lack of activity-specific training limits opportunities to adapt to the constraints of the injury and evaluate one’s own ability to perform the chosen activity at a desired level. Therefore, testing a new sport in which they lack expertise is seen as a comfortable replacement. It has been theorised that movements which are based on previous experiences are easier to plan and therefore become automatic.39 40 This may explain patients’ perceptions of comfort in playing a sport in which they have less experience, as there may be lower likelihood of automatically executing an explosive movement and putting oneself in a situation deemed dangerous.
Strengths and Limitations
Strengths include the unique first-hand, end-user perspective afforded by qualitative interviews, as well as the fact that this study is evaluating a novel training model, which addresses a gap in the literature regarding psychological interventions integrated in physical rehabilitation training. The coding process was rigorous to ensure that the generated conceptual models are representative of participant responses from the perspective of coders with expertise in sport psychology (NC and SG) and physical therapy (EA). A further strength is the thorough analysis of patient experiences of rehabilitation, more clearly illustrating the complexity of rehabilitation in comparison to previous studies, especially as it relates to psychological factors.
Limitations include that patients were familiar with the interviewer and that he is a sport psychologist. However, during recruitment and interviews, information regarding psychological aspects was minimal, with all patients receiving the same written and verbal information regarding study aims (ie, to explore patient experiences of rehabilitation). There was a limited number of available patients in the MOTIFS group, though predetermined criteria for saturation were fulfilled, suggesting that the model is stable.
The fact that the groups were heterogeneous in terms of age, for example, may have an influence on the results in terms of sport-related goals, for example. However, as this is a qualitative study, direct comparison is impossible and future research may further explore this aspect. Likewise, the differences in time since intervention completion were different, which may introduce a degree of recall bias. A priming question was used to aid in recall of details, which was expressed by participants as having been effective, so we believe this to be a minimal risk.
Conclusions
Patients in the MOTIFS group perceived rehabilitation as both physical and psychological preparation for return to activity using structured and explicit strategies which aid in coping with negative psychological factors. CaU rehabilitation follows physical guidelines, but is reported as not being effective at influencing psychological factors due to inadequate psychological information potentially resulting in a lack of psychological coping skills. These results indicate that the MOTIFS model may be a plausible and pragmatic method of addressing psychological factors in knee-injury rehabilitation, and warrants further quantitative research to confirm the efficacy.
Data availability statement
Data are available upon reasonable request. The data used in this study contains sensitive information about the study participants and they did not provide consent for public data sharing. The current approval by the Swedish Ethical Review Authority (DNR 2016/413; 2018/927) does not include data sharing. A minimal data set could be shared by request from a qualified academic investigator for the sole purpose of replicating the present study, provided the data transfer is in agreement with EU legislation on the general data protection regulation, GDPR and approval by the Swedish Ethical Review Authority.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. Ethical approval provided by the regional ethical review board of southern Sweden (Etikprövningsnämnden): Dnr 2016/413, Dnr 2018/927. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the patients for their participation in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @EvaAgeberg
Contributors Study conception, design and planning done by all authors. Data collection by NC. Initial data analysis by NC with subsequent analyses performed by and in collaboration with SG and EA. Manuscript prepared by NC with feedback from EA and SG. EA is primary investigator for the MOTIFS project, and is guarantor for the current study.
Funding Funding for this research was mainly provided by the Folksam insurance company and the Swedish Research Council for Sport Science. Other funders include the Governmental funding of clinical research within the National Health Services (NHS), the Kock’s Foundation, the Swedish Rheumatism Association and the Faculty of Medicine, Lund University. Funding bodies and sponsors were not involved in design or execution of this study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.