Article Text

Abstract
Objectives Foot and ankle injuries are commonly seen in dancers, yet limited studies exist on the injury prevalence of performers of Chinese classical dance. This study aims to determine and assess the prevalence of chronic ankle instability (CAI) in Chinese dancers and correlate the impact of CAI with foot function.
Methods This is a cross-sectional study of 105 Chinese dancers. CAI was assessed using the Cumberland Ankle Instability Tool and foot function via the Foot and Ankle Outcome Score (FAOS). Both self-reported assessment tools were distributed online between January and February 2021. Subjects were divided into CAI and healthy groups to observe any correlations in demographics, training hours and foot function.
Results CAI was seen in 28% of Chinese dancers, with most being unilateral instability. The number of training hours, level of expertise, occupation, gender and age showed no statistical significance with CAI. The FAOS showed that subjects with CAI had significantly greater pain and poorer quality of life.
Discussion and conclusion CAI is a problem affecting 28% of performers of Chinese dance. Future research should investigate the ankle biomechanics in Chinese dance and specific risk factors for CAI to formulate strategies to prevent ankle injuries in Chinese dancers.
- Ankle
- Foot
- Exercise
- Injury
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on the topic
Many dancers accumulate foot and ankle injuries due to increased demand and stress on the ankle, forefoot and plantar flexors. Early identification of chronic ankle instability (CAI) allows for timely treatment and rehabilitation.
There is a knowledge gap in the prevalence of foot and ankle-related injuries in Chinese classical dance.
What this study adds
Highlights the prevalence of CAI in Chinese classical dancers and correlates this with components of foot function such as pain, other symptoms, activities of daily living, sports and recreational function, and quality of life.
Compares the prevalence of CAI in Chinese classical dancers to that of other sports.
How this study might affect research, practice, or policy
Implications for education on injury prevention, proper medical advice, and ankle strength and conditioning to reduce the prevalence of CAI.
Introduction
Many dancers accumulate injuries throughout their careers, including foot and ankle injuries.1 With repeated conditioning and specific techniques unique to dance, increased demand and stress are placed on the ankle, forefoot and plantar flexors. In the Asia Pacific region, limited studies exist on the injury prevalence of dancers of the Chinese dance genre, including Chinese classical dance (Zhongguo gudian wu) and Chinese folk dance (Zhongguo minzu minjian wu).2 Ankle injuries significantly affect a dancer’s performance and subsequent career development. Early detection of ankle instability and injury in Chinese dancers can enable timely treatment and rehabilitation.
This study focuses on Chinese classical dance only. The term ‘Chinese dance’ and ‘Chinese dancers’ will be used to refer to this genre and its dancers hereafter.
Chinese classical dance
Chinese classical dance was created in the 1950s after the founding of the People’s Republic of China. It was based largely on historical Chinese dance forms from different dynasties and regions. The resulting style integrates elements from traditional Chinese martial arts, acrobatics, opera and Western Ballet training.3 This new discipline enabled the unification of dance styles and training across the country. It is widely regarded as a classic Chinese dance style with strong national connotations.
Chinese dance performances usually involve multiple leaps, jumps, turns and tumbling, many of which have a single-foot take-off and landing.4 Jumps are typically continuous, such that dancers perform a series of different jumps one after another without stopping. Turns in Chinese dance are performed in multiple planes and vary in posture, whereas those performed in ballet are often vertical and perpendicular to the ground (figure 1).5 In terms of foot placement and position, Chinese dancers often perform on their toe-tips and forefoot, similar to the demi-pointe position in ballet. Chinese dancers alternate between dancing barefoot, in soft shoes or heels, depending on the performance style and moves required.

Images of Chinese dancers performing on stage in traditional Chinese costumes, involving leaps, partner-work, lifts and prop use. Photo credits: Lam Lu Men (left), Liu Hai Dong (middle) and Tianqiao Theatre (right)
Chronic Ankle Instability
Chronic ankle instability (CAI) is the ‘giving way’ of the lateral ankle. Around 40% of ankle sprains develop into CAI, which may be due to inadequate healing, incomplete rehabilitation or repeated injuries.6 7 Patients with CAI often report persistent twisting of the ankle, swelling, pain and a feeling of instability while in motion.8
The Cumberland Ankle Instability Tool (CAIT) is one of the most common validated screening tools for measuring ankle instability. A Cantonese-Chinese version (CAIT-HK) was cross-culturally adapted and validated for the Cantonese-speaking population (online supplemental file 1).9
Supplemental material
According to the International Ankle Consortium, the inclusion criteria for patients with CAI include (1) a self-reported history of at least one significant ankle sprain, in which the initial sprain occurred more than 12 months ago and (2) a history of recurrent ‘feelings of instability’, which may be defined as a CAIT score of less than or equal to 24. Based on CAIT-HK, a lower cut-off of 20.5 was used for this study.9 10
Assessment tools
Self-reported questionnaires can be effective and accessible tools for screening.11 The CAIT is a self-reported, nine-item questionnaire that assesses CAI in the left and right foot separately. It is scored on a scale of 0 (severe instability) to 30 (no instability).12 The CAIT has been translated into Cantonese-Chinese (CAIT-HK) and validated in a previous study.9
The Foot and Ankle Outcome Score (FAOS) was developed from the Knee Injury and Osteoarthritis Outcome Score and is a self-reporting instrument for measuring foot function.13 The questionnaire is divided into five subscales, with each question scored on a Likert scale: pain, other symptoms, activities of daily living, function in sports and recreational activities, and foot and ankle-related quality of life (QoL). Participants answer based on symptoms in the past 1 week. Each subscale receives a score between 0 (severe symptoms) and 100 (no symptoms). Unlike the CAIT, the FAOS does not specify the left or right side. The FAOS has been translated into Chinese and validated in a previous study (online supplemental file 2).14
Supplemental material
Aim
This study aims to assess the prevalence of CAI among Chinese dancers and correlate the impact of CAI with foot function.
Methodology
Participants
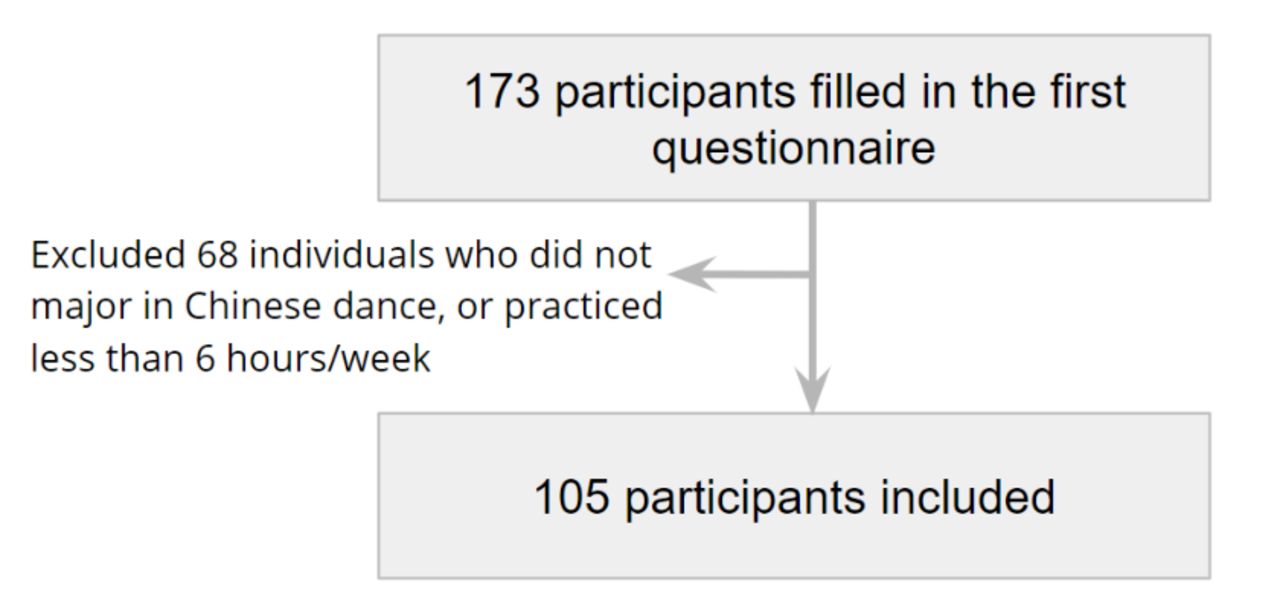
Questionnaire data were collected online using Qualtrics XM software. A total of 173 responses were collected from dancers recruited via dance institutions and companies in Hong Kong and other regions of China between January and February 2021. The questionnaire included basic demographic information of participants, including their gender, age, occupation, training and injury history, as well as the CAIT-HK and Chinese FAOS. The inclusion criteria included dancers that were (1) 16 years old or above, (2) primarily practised and performed Chinese dance and (3) trained 6 hours or above per week in the past 12 months. The exclusion criteria included (1) a history of previous surgeries to the musculoskeletal structures of either lower extremity, (2) any fracture of the lower extremities requiring realignment and (3) acute injury to musculoskeletal structures of other joints of either lower extremity in the past 3 months.
Fourteen responses were excluded as they did not predominantly perform or train in Chinese dance, and a further 54 were excluded due to their weekly training hours being less than 6 hours per week. A total of 105 subjects were included in the study (figure 2).

{kind=link}
{kind=link}
Eligibility criteria for data collection of the prevalence of CAI in performers of Chinese dance. CAI, chronic ankle instability.
Patient and public involvement
The public was involved in the conduct of this study during the recruitment process. Members of dance institutions and companies distributed questionnaires.
Statistical analysis
Statistical analysis was conducted using the IBM SPSS Statistics for Windows, V.26 (IBM SPSS Statistics for Windows, IBM). Participants were separated into groups with and without CAI. The inclusion criteria for CAI originate from the International Ankle Consortium.10 Significance between groups with and without CAI was determined by χ2 tests for age, gender, occupation, level of expertise and weekly training hours. An independent sample t-test assuming unequal variances was used to compare FAOS scores, and effect sizes and confidence intervals were calculated using Cohen’s d, where t-tests were significant.15 16 All statistical tests used p<0.05 to determine statistical significance.
It was conducted in accordance with the STROBE (Strengthening The Reporting of Observational Studies in Epidemiology Statement) guidelines.17
Results
Participant demographics and corresponding CAIT scores are shown in table 1. The mean age was 27, with 80% of participants being female. Full-time professional dancers training more than 18 hours per week made up the largest category for the level of expertise (34.3%). The mean CAIT score was 23.0 for the left ankle and 22.4 for the right ankle.
Patient demographics and CAIT scores
Of the 105 participants included in the study, 29 participants had CAI. Sixteen had unilateral CAI, and 13 had bilateral CAI (table 2). Table 3 shows the demographics of participants with and without CAI. χ2 test results showed no statistical significance between ankle stability and age, gender, occupation, level of expertise and training hours.
Prevalence of Chronic Ankle Instability (CAI), n (%)
Demographics of participants with and without CAI, n (%)
An independent sample t-test assuming unequal variances was conducted to compare the FAOS scores in the CAI and healthy groups (table 4). There was a significant difference in the scores between CAI and healthy groups for pain (p<0.05) and QoL (p<0.01) subscales. This suggests that participants with CAI experience significantly worse pain and QoL than their healthy counterparts. The effect size was also calculated where t-tests were significant. Effect sizes were moderate for both pain and QoL.
FAOS scores
Discussion
The primary aim of this study was to estimate the prevalence of CAI among Chinese dancers and its impact on foot function. To the best of our knowledge, this is the first study exploring the prevalence of CAI in performers of Chinese classical dance. Based on 105 participants, we found the prevalence of CAI to be 28%.
CAI in Chinese dancers
Chinese dance is a physically demanding sport. With repetitive multidirectional jumping and turning manoeuvres, dancers are expected to sustain foot and ankle injuries. Chinese dancers often land from jumps on the forefoot and perform on their toe-tips and metatarsal heads, similar to demi-pointe in ballet. Sustained weight-bearing in this maximum plantarflexion position increases the risk of inversion injuries due to minimal ligamentous support.6 18 19 Chinese dancers may compromise normal anatomical alignment for aesthetic purposes, for example, forcing ankle supination to keep the feet ‘in-turned’ or ‘sickled’, which puts added stress and elongates the lateral ankle ligaments.19
The prevalence of CAI in this study was lower compared with previous studies in different dance genres and sports. A study among student dancers of ballet and modern dance saw 53.2% of dancers with CAI.20 When compared with non-dance sports, a systematic review noted that a cohort of track and field athletes showed the highest percentage of perceived CAI (41%), with netball close behind (39%).21 In another study of student athletes, 23.4% had CAI, with rowing, aquatics and basketball having the highest percentages.22 There was a wide range of prevalence due to differences in participant characteristics and research methods, so study parameters should be considered when interpreting prevalence.
Factors contributing to CAI
Factors that may precipitate ankle injuries and subsequent CAI in dancers were considered in this study, including intrinsic factors such as age and gender, and extrinsic factors such as occupation, level of expertise and training hours. Our findings revealed no statistical significance between the abovementioned factors and the CAI prevalence. The relationship between age, training experience and CAI is unclear. Pourkazemi et al and Tanen et al found that younger age groups were at a higher risk of developing recurrent ankle sprains and CAI than older age groups.22 23 Nilsson et al also correlated the young age of ballet dancers with a higher risk of ankle sprains, which can subsequently develop into CAI.24 On the other hand, risk and incidence of overuse injuries in dancers were previously found to be positively associated with years of dance training and increased training time.25–27 However, our findings and two other studies found insignificant relationships between age and CAI.28 29 The inconsistent findings may be due to differences in injury history, activity or training load between studies, and varying study methodologies. Regarding gender, a higher prevalence of CAI was observed in young female athletes compared with males.22 30 However, the small sample of male participants in our study cohort made it difficult to observe any significant relationship.
Other determinants may also contribute to the high prevalence of CAI in Chinese dancers, such as incorrect technique, insufficient warm-up, fatigue, performing while in pain and returning to dance prematurely without adequate recovery.2 31–34 Similar to other genres of dance, Chinese dancers are also prone to delaying health-seeking behaviours to avoid losing time from training, as doing so may affect career prospects.35 Combining these behaviours may further precipitate injury recurrence for dancers with previous ankle sprains. Furthermore, psychosocial and environmental factors such as intensive dance training accompanied by varying coaching styles, performances and examination stress may also be risk factors for dance injuries.36
CAI and foot function
The difference in FAOS scores between the CAI and healthy group demonstrates that CAI can significantly impact some aspects of foot function. Compared with the healthy group, participants with CAI had greater pain and poorer foot and ankle-related QoL. A study by Lai et al found that Chinese dancers experienced more severe hindfoot and ankle pain than contemporary dancers. Still, interestingly, Chinese dancers were at a higher risk of developing midfoot or forefoot injuries than hindfoot injuries.37 Pain also appeared to be a major problem in people with CAI.38 39 However, it is unclear whether the pain is secondary to CAI or whether the pain is a risk factor for developing CAI.
The two groups had no significant differences in sport or daily function. This was unexpected as ankle pain would likely hinder routine training and day-to-day function. This may be due to the design of the FAOS questionnaire, where participants answered based on symptoms in the past week. Participants may report significant foot and ankle pain in the past week but no corresponding limitation in sporting function as they may have temporarily stopped training for rehabilitation.
Injury prevention
In one of the dance institutions studied, measures have been implemented to minimise their dancers’ injuries, such as self-tracking mobile applications to document injuries and risk factors. However, these measures are not widely used. Methods to reduce injury risk may be valuable, such as enforcing strengthening and conditioning programmes, enhancing access to specialist care at the time of injury, educating dancers on injury prevention through appropriate warm-ups and breaks during long rehearsals, and discouraging the culture of dancing through the pain.
Strengths and limitations
This study explores a genre of dance that has not yet been thoroughly researched. Identifying the prevalence of CAI in Chinese dancers forms a basis for future studies in this dance genre. The validated self-reported questionnaires are convenient and accessible tools for screening. In the design of this study, the CAIT and FAOS are complementary in nature, as each questionnaire focuses on different aspects of ankle function. While CAIT focuses on ankle instability, FAOS accounts for other foot conditions such as pain, inflammation or overuse injuries.
There were some limitations in this study. In determining the prevalence of CAI, the approach of using self-reported measures is subjective and risks recall bias.22 40 Limitations in questionnaire design were present—the FAOS was designed to measure foot function and symptoms in the past week, while the CAIT does not specify a time frame. Since this questionnaire was distributed during COVID-19, when public health interventions had led to the closure of dance facilities, the ‘normal’ training of dancers during the week of completing the questionnaire may have been affected. Also, while the sample size was moderate, the sample size was small during subgroup analysis.
Future directions
Only perceived ankle instability was measured in this study. Further studies on the biomechanics of Chinese dance can be done for more objective analyses with quantification of mechanical instability and accounting of differential diagnoses such as syndesmosis instability to be ruled out.41–45 In addition, a greater focus on the specific risk factors predisposing Chinese dancers to CAI should be explored.
Conclusion
Our results show that CAI is a major problem for Chinese dance performers, with 28% suffering from the condition. CAI is associated with greater pain and a poorer QoL. Education on injury prevention, proper medical advice and ankle strength and conditioning are crucial in reducing CAI in the future.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Survey and Behavioural Research Ethics Committee at the Chinese University of Hong Kong (30 April 2021/SBRE-20-531). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Thank you to Henry Lam of the Hong Kong Association of Dance Medicine and Science and David Tsui of the Hong Kong Dance Company for their support and recruitment of participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drsling
Contributors VWTC, AHKT and JYNH contributed to the design and implementation of the research, analysis of results and writing of the manuscript in consultation with HHTY, PSHY and SKKL. HHTY contributed to participant recruitment and data acquisition. SKKL is the guarantor and accepts full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.