Article Text

Abstract
Objectives To identify how primary care physicians (PCPs) prescribe physical activity for patients with chronic disease, and to determine characteristics of physical activity interventions with improved clinical outcomes of chronic disease.
Design A scoping review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews 2018 was completed.
Data sources Four bibliographic databases (Medline, EMBASE, SPORTDiscus, CINAHL) and four grey literature/unpublished databases (Proquest, National Institute for Health and Care Excellence, Canadian Health Research Collections, Clinical Trials) were searched from inception to 7 March 2022.
Eligibility criteria for selecting studies Studies involving PCP-delivered physical activity prescriptions or counselling for participants with a chronic disease or mental health condition, which reported clinical outcomes were included. Opinion papers, news and magazine articles and case reports were excluded, as were studies in which a physical activity intervention was provided for primary prevention of chronic disease, prescribed by healthcare providers or researchers other than PCPs, or for healthy participants without chronic disease.
Results An initial search identified 4992 records. Fifteen studies met inclusion criteria. Characteristics of physical activity prescriptions that improved clinical outcomes included: personalised advice; brief intervention; behavioural supports (handouts and/or referrals) and physician follow-up. Reported adverse events were rare. Research gaps include optimal timing and length of follow-up, and the long-term and cost-effectiveness of interventions.
Summary/Conclusion Several characteristics of physical activity counselling by PCPs for patients with chronic disease may improve clinical outcomes, although research gaps remain. Studies exploring the effectiveness of physical activity prescription for individuals with chronic conditions are urgently needed.
- physical activity
- exercise
- physical activity promotion in primary care
- non-communicable disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Physical activity can improve prevention and treatment of a myriad of chronic diseases.
Physician counselling to increase physical activity is effective, but underused due to lack of time, training or belief that patients will engage.
Many patients see their primary care physician on an annual basis and would welcome tailored advice on physical activity.
WHAT THIS STUDY ADDS
Characteristics of physical activity prescriptions to improve clinical outcomes of chronic disease include: personalised and brief advice according to patient factors and goals; use of behavioural supports including handouts and/or referrals and physician follow-up.
For the two studies in which no change in clinical outcomes was observed, it was postulated that limited interactions with PCPs and/or generic advice contributed.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Given the frequency of contact with large segments of the population living with chronic disease, studies exploring the effectiveness of physician-led physical activity prescription for individuals with chronic conditions are urgently needed.
Future trials should address research gaps including optimal timing and length of follow-up, and the long-term effectiveness and cost-effectiveness of interventions relative to specific chronic conditions.
Introduction
According to WHO, physical inactivity is the fourth leading risk factor for death worldwide.1 Inactivity exposes an individual to a similar health risk as smoking and obesity.2 Strong evidence for the therapeutic use of physical activity in several chronic diseases continues to emerge; including but not limited to, metabolic syndrome-related disorders, heart and pulmonary disease, rheumatoid and osteoarthritis, cancer and mental health disorders such as depression.3–7 For this reason, physical activity has been called ‘the miracle cure’.8
Primary care physicians (PCPs) have an important role to play,9 as approximately 80% of individuals visit their doctors every year10–12 and prefer to get health information directly from their PCP.13 Physician counselling to increase physical activity levels in otherwise healthy, sedentary individuals is effective but underused due to lack of time, training or belief that patients will engage.14–16 What is less well known is how PCPs currently prescribe physical activity for patients with chronic conditions, and which key characteristics are associated with an improvement in clinical outcomes.
The objective of this scoping review was to identify key characteristics of physical activity prescriptions by PCPs, which result in improved clinical outcomes of chronic disease. A secondary objective was to identify research gaps in the area. The primary outcomes of interest were the key characteristics of interventions that included physical activity prescriptions by PCPs and improvement in clinical outcomes. Secondary outcomes included the role of the PCPs in each aspect of the intervention, the clinical outcomes themselves and the presence of any serious adverse events.
Methods
This scoping review was completed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR).17 18 We followed the frameworks of Arksey and O’Malley19 and Levac et al20 to systematically identify relevant literature and extract themes pertaining to the research objectives and identification of evidence gaps.
Eligibility criteria
We included studies involving PCP-delivered physical activity prescriptions or counselling for participants with a chronic disease or mental health condition, which reported clinical outcomes. The search was not restricted by year, geographical location, study setting or design, participant age, gender or sex or language; however, only articles in English were included in the review. Systematic reviews and meta-analyses, scoping reviews, guidelines and grey literature were eligible for inclusion. Opinion papers, news and magazine articles and case reports were not included. Studies in which a physical activity intervention was provided for primary prevention of chronic disease, prescribed by healthcare providers or researchers other than PCPs, or for healthy participants without chronic disease were excluded.
Information sources
We conducted the search in four bibliographic databases (Medline; EMBASE; SPORTDiscus; CINAHL) and four grey literature/unpublished databases (Proquest Dissertations and Theses; National Institute for Health and Care Excellence; Canadian Health Research Collections; Clinical Trials) in August 2021 and updated on 7 March 2022.
Search
The search strategy was constructed to answer the research question: ‘What is known about how physical activity prescriptions are delivered by PCPs for patients with chronic disease and what are the key characteristics associated with improved clinical outcomes of chronic disease?’ We built the search architecture (online supplemental file 1) based on a preliminary search of published articles and in consultation with a research librarian.
Supplemental material
Selection of sources of evidence
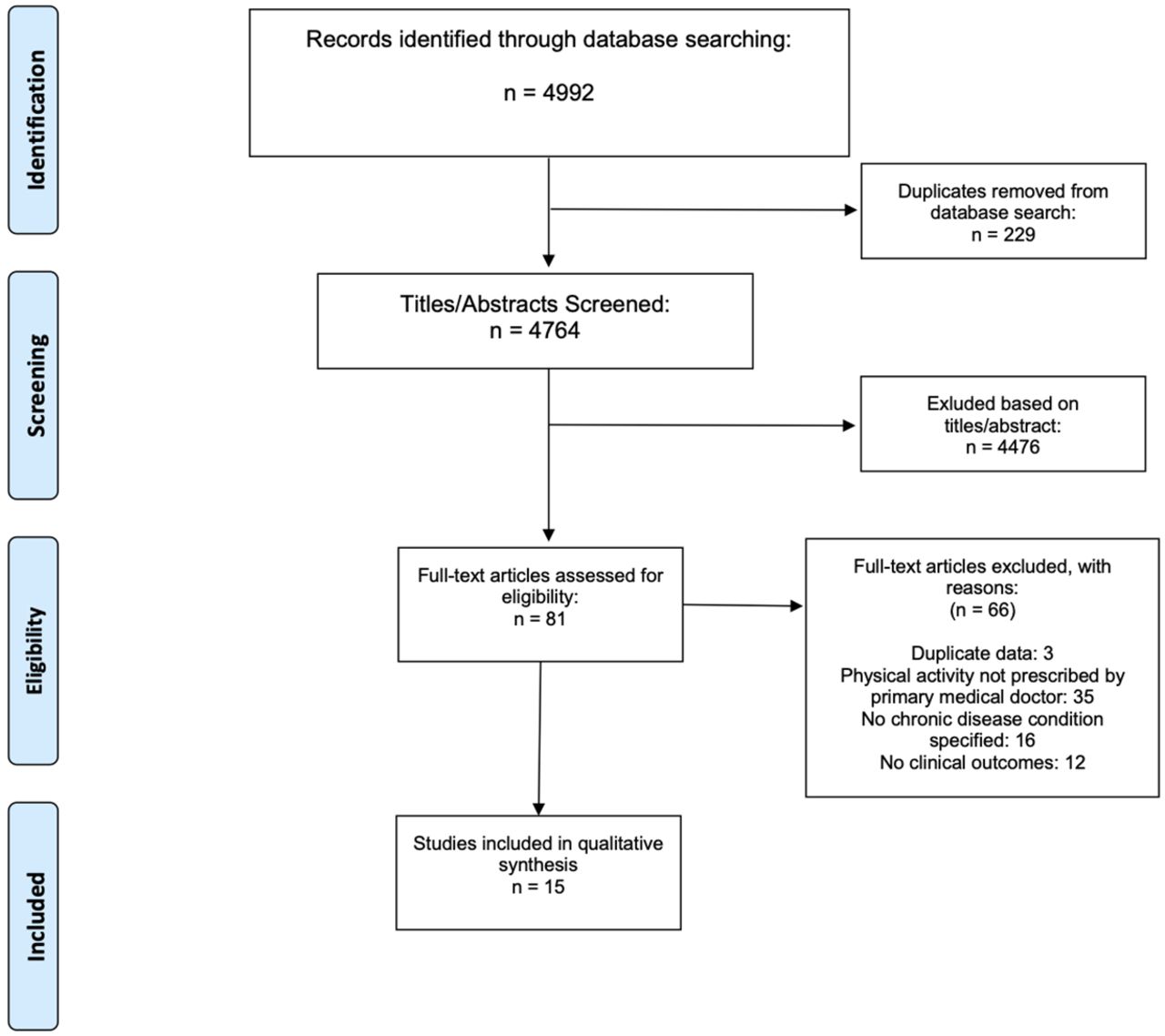
We collated all identified records into Endnote (X8) and removed duplicates using an automatic feature. Two reviewers evaluated all titles and abstracts (JT, TN). Selected articles were reviewed in full for further inclusion by two independent reviewers (JT, TN); in cases of disagreement, a third reviewer was involved (RP). Details of the search process are reported in a PRISMA-ScR flow diagram (figure 1).

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram.
Data items and charting process
Articles selected for inclusion underwent data extraction onto a standard Excel spreadsheet. One reviewer extracted the data (JT, TN) and a second reviewer (JT, TN) confirmed data for accuracy. The following data were extracted from included studies: publication details (year published, study location, study design, author details); primary health outcome evaluated; participant characteristics (sample size, sex/gender, age, chronic condition); intervention description; PCP role; main results for health outcomes and any reported adverse events.
Synthesis
We employed a narrative approach to synthesise findings.19 Extracted data were assessed descriptively and a thematic summary developed grouping the articles based on effect of the physical activity intervention on the clinical outcomes (eg, improvement, no change, etc). We identified characteristics pertaining to the PCP’s role in studies reporting improved clinical outcomes. We then identified evidence gaps and areas for future research.
Results
Our initial search yielded 4992 articles, and after removing duplicates, we screened 4764 titles and abstracts. We identified 81 full texts, and 15 studies were eligible for inclusion (figure 1). Of these, 5 were observational and 10 were randomised controlled trials. Seven studies were mixed interventions incorporating diet-related or general healthy lifestyle components in addition to physical activity.21–27 Chronic conditions reported in the studies included obesity,24 28–30 dyslipidaemia,23 25 hypertension,26 type 2 diabetes31 32 and metabolic syndrome.21 22 Clinical outcome measures included anthropometrics (waist circumference, body mass index),21 22 24 26 28 30 31 blood pressure,21 26 cholesterol,23 25 31 32 glycated haemoglobin,21 31 triglycerides,25 sodium,26 carotid artery distensibility,21 global cardiovascular risk23 and general and mental health scores.29 Study characteristics, role of the PCP and a summary of study findings are found in online supplemental table 1.
Supplemental material
Characteristics of PCP-led physical activity prescriptions for patients with chronic disease
Physical activity prescription interventions in the 15 studies included descriptions of the type of advice (personalised or generic), type of intervention (brief or in-depth counselling), the use (if any) of behavioural supports and follow-up (if any).
Type of advice
Personalised advice
In 12 of the 15 studies, the PCP provided a personalised physical activity prescription,21–26 28–33 by identifying participant barriers, goals and readiness for change; and establishing specific amounts, intensities and types of physical activity. In seven studies, PCPs also assessed baseline clinical outcomes relevant to cardiorespiratory fitness (eg, activity levels, cardiovascular risk assessment, anthropometric measurements, blood pressure and fasting glucose levels).21 23 26 28 30 32 34
Stage of/Readiness for change identification: in 9 of the 15 studies, the PCP considered patients’ readiness for change when tailoring the physical activity prescription.21 25 26 28–33 Stage of change assessment is a specific step within the Patient-centred Assessment and Counselling for Exercise (PACE) protocol for brief counselling delivered by the PCP, which was employed in four studies26 28 30 33 and involves assigning patients to one of three groups: precontemplation, contemplation/preparation or action/maintenance. Understanding a patient’s readiness for change and/or resolving their ambivalence towards change is also a core component of motivational interviewing (MI)-based interventions.25 29 31 32
Barrier and facilitator identification: identifying the existing and/or potential personal barriers to physical activity perceived by patients as well as developing strategies to overcome them was another component of personalisation in eight studies.25 26 28–33
Goal setting: individualised goal setting (ie, personal goals set by patients guided by the PCP) was included in eight studies as a component of an established protocol such as PACE or MI.25 26 28–33
Amount, intensity and type of physical activity: ten studies involved personalising the amount (ie, duration in number of minutes), frequency (ie, number of times per week), intensity (moderate, vigorous) and/or type of physical activity.21–23 26 28–33 In one case, patients were encouraged to achieve a preset (ie, not personalised) amount of physical activity, typically based on national guidelines.24 In seven studies, PCPs specified (moderate) intensity of physical activity.21 23 26 28–30 33 Finally, PCPs in four studies based the type of activity on the basis of patient preference.28 29 31 32 In one study, PCPs encouraged patients to take up specific, although not personalised activities (eg, walking, resistance/strength training, group exercise classes)24, while others did not incorporate individualised guidance on type.21 22 25 33
Generic advice
van Sluijs et al noted the lack of intervention effect in their study could be attributed to providers not tailoring their counselling to individual stages of change.33 In three studies the PCP provided generic advice,27 34 35 all of which resulted in no change or mixed outcomes.
Type of intervention
Six of the 11 studies which reported improvements in clinical outcomes included brief physical activity counselling.23 24 26 28 30 Brief intervention in these cases involved physical activity counselling from 2 to 10 min via the PACE protocol.26 28 30 33 One study, using the Swedish Physical Activity on Prescription (PAP) protocol, involved brief counselling by the PCP with other healthcare professionals delivering longer counselling sessions.29 In three studies, PCPs delivered longer interventions including MI or general lifestyle counselling.25 31 32
Use of behavioural supports
In 7 of the 15 studies, patients were provided printed educational tools and resources by their PCP.24 29 31 34 Four interventions included a printed physical activity prescription.26–29 Two studies included providing referrals for personal trainers30 or fitness programmes.35 Four studies incorporated self-monitoring, or the recording of physical activity behaviours (eg, time, place, duration, etc) in a log or journal.24 28 29 31 Patients were instructed to keep a general activity record,24 notes detailing type, duration and obstacles that arose,28 or daily step counts.29 31
Follow-up
In 8 of the 15 studies, the PCP provided follow-up assessments, reminders or information sessions.22–24 26 29–31 33 Some interventions included a combination of in-person and phone call follow-up19 25 or a ‘booster session’.33 In two studies, PCPs mailed a letter to reinforce physical activity advice.28 29
Characteristics of interventions in studies with improved clinical outcomes
Among the 11 studies reporting improvements (table 1), all included a personalised physical activity prescription, and 7 included a PCP-delivered brief intervention.23 26 28–30 32 33 Seven provided behavioural support21 24 26 28–31 and eight included in-person follow-up.21–26 31 32
Physical activity prescription characteristics in studies with improved outcomes (n=11) and no change or unclear change in outcomes (n=4)
Characteristics of interventions in studies with no or unclear change in clinical outcomes
The two studies reporting no change in outcomes involved limited interaction with the PCP and/or generic advice (eg, general letter from PCP about physical activity, one follow-up at 4 weeks33 34). Of the four studies with no or unclear change in outcomes, only one included personalisation of any kind by a PCP, and none included self-monitoring.
Adverse events
Two of the 15 studies reported adverse events associated with physical activity. One fitness assessment that included a maximal exercise test was stopped because a participant felt unwell.32 In another study, a participant was hospitalised, however it was unclear whether this was a result of the intervention.26 Although not reported as adverse events, one study reported a lack of adherence to the physical activity prescription at 10 weeks due to ‘interruptions to the established routine’, which included illness and injury (sometimes attributed to exercise sessions).35
Discussion
PCPs prescribe physical activity for patients with chronic conditions involving a number of characteristics which may improve physical and mental health outcomes. Findings from this review are in line with literature outlining the essential role that PCPs play in identification of patients at risk of chronic disease (eg, cardiovascular disease) and providing long-term follow-up.36 When PCPs are engaged in physical activity prescription and follow-up this may also have considerable influence on patients’ health-related behaviours.37 PCPs providing physical activity advice can also play an important societal and public health role due to frequent contact with large segments of the population, especially those with poorer health, lower socioeconomic status and/or who are older.38
Characteristics of physical activity prescriptions by PCPs in studies with improved clinical outcomes
Based on the findings of this review, four characteristics of PCP-led physical activity prescriptions or counselling in the subset of studies with improved clinical outcomes include: personalised advice; brief intervention; behavioural supports and follow-up (box 1). By contrast, when an intervention did not produce its expected improvement, study authors attributed this to low PCP involvement (eg, recruitment only) or lack of personalised advice.33
List of gaps in knowledge for primary care physician (PCP)-led physical activity prescription in chronic disease
Many chronic conditions have not been investigated to date.
The role of the PCP needs to be further elucidated in counselling and follow-up.
Long-term effectiveness of interventions is not known.
Cost-effectiveness of clinical interventions involving patients with chronic conditions is not known.
Personalised advice
In settings with patients with chronic disease, physical activity interventions should be tailored to individual needs and preferences, consistent with other studies examining patient preferences on physical activity counselling.39 This personalisation includes identifying stage of and readiness to change, barriers and facilitators, goal setting and determining amount, type and intensity of physical activity. These findings are consistent with the broader literature, where personalisation can also include individualised framing of prescriptions to achieve the patient’s immediate health and functional goals (eg, avoiding surgery, reducing pain symptoms, managing health conditions without medication, improving balance to reduce fall risk, improving mental health).40 41 Patients with depression and female patients may specifically benefit from personalised physical activity prescriptions.27 28 42 43
Intervention type
In this review, we found that PCPs generally employed one of two intervention types: brief intervention or MI. Brief intervention involves less time than traditional MI and is an effective way of addressing one of the main barriers of PCPs delivering physical activity interventions: time constraints.13 44 45 Several existing protocols for physical activity prescription use brief interventions—including the PACE and Swedish PAP programmes. The PACE model may have a dual advantage as it minimises the duration of the intervention and improves the PCP’s knowledge and abilities at the same time.28 Individual counselling appeared to outperform group counselling for improvements in clinical outcomes—attributed to the patient-provider rapport.31
Behavioural supports
Behavioural supports include printed physical activity prescriptions, patient education handouts, activity logs and referrals to allied health. Patient handouts are low-cost educational tools that are effective in improving patient care and outcomes.46 47 They may also provide benefit for physicians who experience time constraints. Others have emphasised the need for readability and accessibility,48 49 particularly for physical activity resources. By referring patients to allied health professionals, PCPs may benefit from sharing the ‘workload’ of assessments and personalised consultations.32
Follow-up
Follow-up appeared to increase patients’ motivation and adherence. This is consistent with findings that patients expect their PCP to address physical activity regularly.39 Follow-up by a PCP may include reminders of the initial prescription, assessment of physical activity goals and health outcomes measurement. Optimal timing, type and length of follow-up is yet to be determined, although most studies included 3–6 months follow-up appointments.22 24 29 50
Knowledge gaps
We identified several knowledge gaps (box 1). In this review, studies investigated physical activity prescription involving four common chronic conditions, yet there are >25 chronic conditions in which physical activity can play a role in prevention and treatment.51 While physical activity interventions in primary care are cost-effective, knowledge gaps include effectiveness and comparative costs of interventions in chronic disease settings.34
It is possible that studies incorporated additional elements of personalisation, behavioural supports or follow-up within the intervention which were not described in sufficient detail. There was a large variation in intervention design (role of PCP, type, frequency of involvement, duration of the intervention and follow-up), for example, length of follow-up for the study outcome measurement varied from 24 weeks to 54 months. Long-term effectiveness is unknown.
Finally, information pertaining to the intervention agents and their involvement within the study was often lacking and, in some cases, made it challenging to draw conclusions regarding the role of PCPs. Guidelines such as the Template for Intervention Description and Replication checklist can improve the quality of reporting and increase potential replication.52
Strengths and limitations
A strength of this study is the use of an appropriate design for this topic; the scoping review design is suited to the multifaceted interventions and real-world implementation messages that we sought. A second strength is the focus on PCPs which restricts generalisability but increases applicability to a larger population of patients, as not all patients have access to allied health practitioners or research teams. A limitation of the studies reviewed may be their incompletely known quality; they may be prone to response bias (eg, those who are already fit being more likely to participate and have better outcomes) and lack of control groups. A limitation of scoping reviews in general is the inability to determine the effectiveness of the interventions and assessing the quality of studies is not possible. With multifactorial lifestyle interventions, it is impossible to directly attribute changes to physical activity components, and further research investigating physical activity as a standalone intervention is eagerly anticipated.
Conclusion
Physical activity counselling by PCPs for patients with chronic disease includes several characteristics which may improve clinical outcomes, although research gaps remain. These characteristics include personalised advice, brief intervention, behavioural supports and follow-up. The field is ripe for research into many more chronic conditions as well as research evaluating effectiveness of interventions. Positive results will enhance fidelity and confidence for patients and providers alike, and facilitate physician engagement, remuneration and training requirements. Given the frequency of contact with large segments of the population living with chronic disease, studies exploring the effectiveness of physician-led physical activity prescription for individuals with chronic conditions are urgently needed.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors thank Ms Jane Yuan, Ms Karen Simmavong and Mr John Costella for their administrative and technical assistance with this study. This work was supported by the Unnur Brown Award for Leadership in Health Policy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JaneSThornton
Contributors JT developed the idea and wrote the first draft. JT and TN conducted the search and evaluated the studies. RP acted as third reviewer when needed. KR and MS provided expertise in qualitative analysis. MS and RP provided study oversight. All authors were responsible in editing the manuscript and final approval of the submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JT is an Editor of the British Journal of Sports Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.