Article Text

Abstract
Objective Report on long-term follow-up results in the apnoea hypopnea index (AHI) and self-reported daytime sleepiness in participants with moderate to severe obstructive sleep apnoea at 12 weeks after completion of a high-intensity exercise training or control intervention.
Methods Twenty-six participants with obstructive sleep apnoea (body mass index (BMI) 37 (36–39) kg/m, age 52 (49–55) years, apnoea-hypopnoea index 40.5 (31.3–50.2) events/hour), randomised to either 12 weeks of supervised high-intensity interval training (HIIT) (4×4 min of treadmill running or walking at 90%–95% of maximal heart rate) or no intervention (control), underwent a sleep evaluation follow-up 24 weeks after intervention initiation. Respiratory measures during sleep were registered at baseline, 12 weeks (postintervention) and 24 weeks (long-term follow-up).
Results At the 24-week follow-up, there were no statistically significant differences between the groups in the AHI (HIIT 30.7 (17.2–44.1) and control 38.7 (22.8–54.5) events/hour), Epworth score (HIIT 7.0 (4.7–9.3) and control 5.5 (3.9–7.0)), mean oxygen saturation (HIIT 93.2 (92.5–93.9) and control 92.0 (91.1–92.8)) or oxygen desaturation events (HIIT 32.9 (20.4–45.4) and control 44.3 (27.3–61.3) n/hour). BMI remained unchanged from the baseline in both groups. In the HIIT group, only two participants reported having continued with HIIT at 24 weeks.
Conclusion The effect of 12 weeks of supervised high-intensity exercise training on AHI and self-reported daytime sleepiness was lost at the 24-week follow-up.
- exercise
- sleep
- aerobic fitness
Data availability statement
No data are available. The ethical approval does not support sharing of data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Obstructive sleep apnoea is associated with physical inactivity.
Exercise interventions improve obstructive sleep apnoea.
Knowledge of the effects of long-term adherence to high-intensity exercise training on obstructive sleep apnoea is limited.
What this study adds
Few participants with obstructive sleep apnoea continued with high-intensity exercise training beyond the supervised intervention.
Adherence to long-term high-intensity exercise training is challenging for participants with obstructive sleep apnoea.
The small positive effect of 12 weeks of supervised exercise on the apnoea hypopnea index (AHI) and self-reported daytime sleepiness was most likely lost due to detraining in participants with moderate obstructive sleep apnoea.
How this might affect research, practice and policy
Future studies should examine the exercise intensity, mode and volume that is most likely to achieve long-term adherence to regular exercise in participants with obstructive sleep apnoea.
The effects of long-term high-intensity or moderate exercise training on obstructive sleep apnoea should be investigated further.
The underlying mechanisms connecting improvedAHI and daytime sleepiness with regular exercise training should be further investigated.
Introduction
Obstructive sleep apnoea (OSA),1 sleep deprivation and daytime sleepiness are associated with physical inactivity,2–4 and both OSA and physical inactivity are associated with obesity, hypertension, type 2 diabetes and cardiovascular disease.5 Modest improvements in the apnoea hypopnea index (AHI), self-reported sleepiness, maximal oxygen uptake (VO2max) and quality of life have been reported after relatively short exercise interventions.6–12 In general, adherence to exercise training after a structured rehabilitation programme is moderate to good, depending on the population studied and the programme investigated.13–16 Promising results have been reported in studies of long-term follow-ups in patient activity and home-based rehabilitation studies.13 15 In a study of the combination of weight reduction and increased physical activity, improvement in OSA was sustained 4 years after the active 1-year intervention.17 To our knowledge, little data exist on the effects of long-term adherence to high-intensity exercise training on AHI or daytime sleepiness in patients with OSA. In this study, we report long-term follow-up data on AHI and daytime sleepiness in participants with moderate to severe OSA: here, ‘long-term’ is 24 weeks after the initiation of the study and 12 weeks after the participants completed either a supervised high-intensity interval training (HIIT) intervention or a control intervention.7
Materials and methods
Study design
Twenty-eight participants with OSA completed a 12-week intervention. Participants were randomised to either a HIIT group or a control group that did not received supervised intervention (CON).7 Participants were investigated at the baseline, at 12 weeks and at 24 weeks. In the current paper, we report sleep data from the long-term postintervention follow-up, at the time point of 24 weeks after study initiation and 12 weeks after completion of the intervention. Twenty-six participants completed the 24-week follow-up sleep evaluation (HIIT n=12, CON n=14), and 16 participants underwent a VO2max test (figure 1). The inclusion criteria were a body mass index (BMI) ≥30 kg/m2 and an AHI ≥15, and the exclusion criteria were any disability precluding exercise intervention and known ischaemic cardiovascular disease. The primary study outcome was AHI at 12 weeks, measured using respiratory polygraphy. Secondary outcomes included the Epworth sleepiness questionnaire (Norwegian version)18 and the long-term postintervention follow-up.

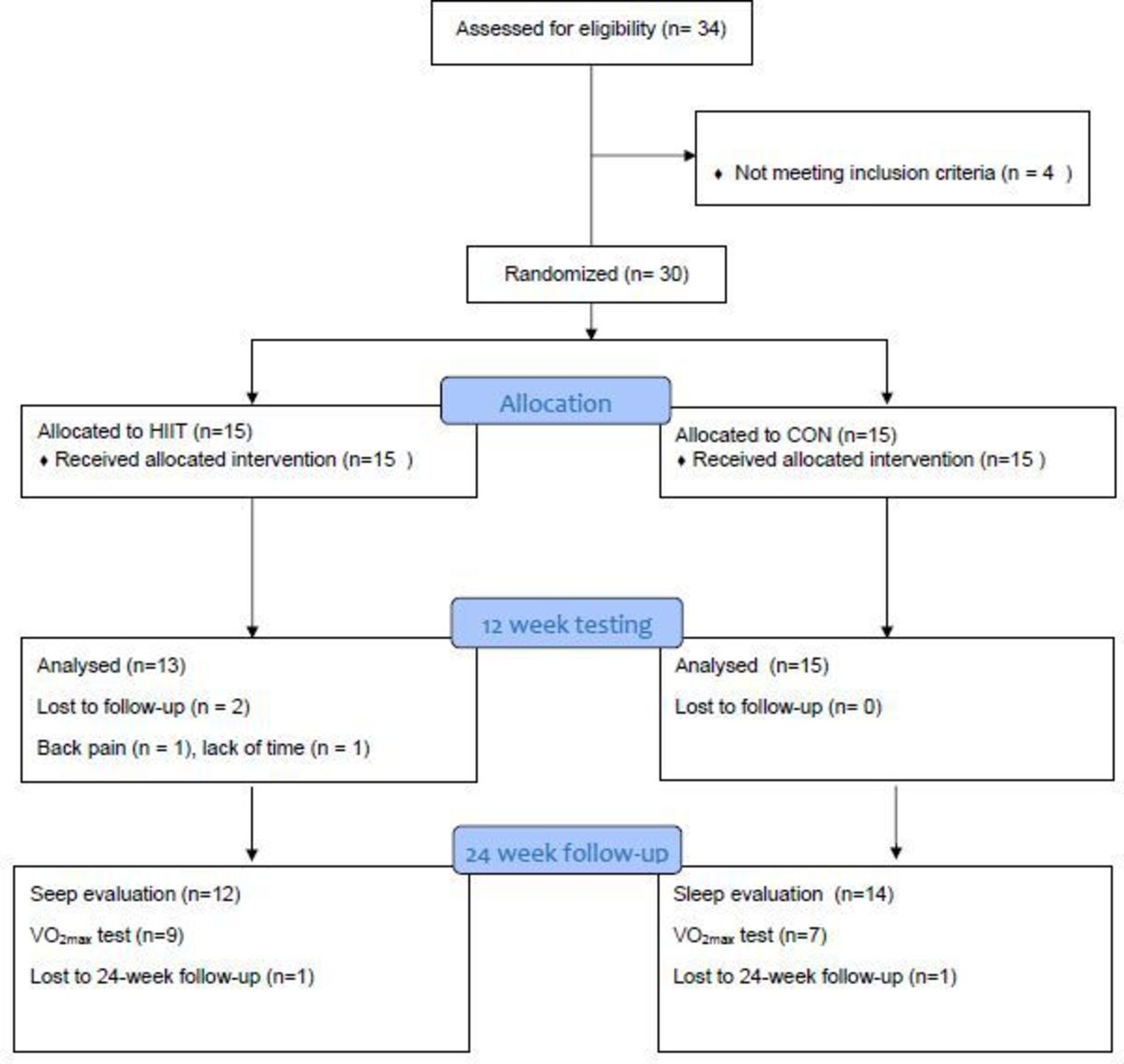{kind=link}
Study flowchart. CON, control group; HIIT, high intensity interval training group, VO2max, maximal oxygen uptake.
Exercise training intervention
The full exercise intervention is described in Karlsen et al.7 Briefly, HIIT involved 4×4 min of treadmill walking or running at 90%–95% of maximal heart rate (HRmax), two times a week, for 12 weeks.19 The target exercise intensity was achieved using heart rate monitors. Treadmill speed or grade was increased throughout the training period to maintain the target exercise intensity. The control group was encouraged to continue their normal lifestyle during the intervention period. After the intervention, the participants in the HIIT group were asked to continue the exercise training programme at home, while participants in the control group were given the opportunity to perform one HIIT session in the laboratory in order to sustain their motivation to continue the study and meet for the 24-week follow-up.
At the 24-week follow-up, participants in the HIIT group were asked whether they had continued HIIT beyond the supervised intervention. In addition, the participants were asked to fill out the International Physical Activity Questionnaire (IPAQ) short form for the last 7 days.20 21 The data were analysed and categorised according to the questionnaire’s user manual (www.ipaq.ki.se/scoring.htm). The levels of physical activity were classified based on weekly metabolic euqvivalent per minutes (MET-minutes) (the sum of the metabolic energy requirements of specific activities or tasks performed in 1 week. One metabolic equivalent, one MET=3.5 mL of oxygen consumption·kg-1min-1), with the categories of low (<600), moderate (600–3000) or high (≥3000) physical activity.22
Demographics
Body weight and body composition were measured using a bioimpedance scale (Omrun BF500, Omron Healthcare, Japan). Systolic and diastolic blood pressures were measured using a polygraph (SunTech Medical, Tango+) in line with standard procedure. Fasting venous plasma and serum samples were collected for standard haematology, and biomarkers were analysed at the Department of Clinical Chemistry at St. Olav’s University Hospital.
Sleep evaluation
The participants underwent one full night of data collection using respiratory polygraphy with ambulatory equipment (Embletta, Embla, Ontario, Canada) at home, without the use of CPAP, at baseline, 12 weeks and 24 weeks. The morning after, participants reported their sleeping patterns and answered the Epworth sleepiness questionnaire. A specialist in clinical neurophysiology analysed the registrations blinded for information of intervention using Somnologica studio V.5.1 (Micromed S.p.A. Mogliano Veneto (TV), Italy) and standardised guideline criteria.23–26 Further details of the sleep evaluation methodology are found in Karlsen et al.7
Cardiopulmonary exercise testing
VO2max was measured during treadmill running/walking at baseline, 12 weeks and 24 weeks using indirect breath-by-breath calometry (MMX-II, CORTEX Biophysik GmbH, Germany). Specifically, the participants warmed up for 15 min at ~70% of HRmax before being fitted with the test equipment, and the workload gradually increased until the participants reached exhaustion. VO2max was defined as the mean of the three highest consecutive 10 s measurements where the VO2 levelled off despite an increase in intensity, with a respiratory exchange ratio value above 1.10.
Statistics
We used IBM SPSS V.28 for the statistical analysis (IBM SPSS statistics, USA). Data are presented as means and 95% CI. We used a linear mixed-effect regression model with random intercepts to investigate changes between the groups over time from 12 weeks to 24 weeks. Data normality was investigated using QQ-plots and tests of between-group effects, and the homogeneity of variance was tested using Levene’s test. Trends within groups were investigated using analysis of variance (ANOVA) for repeated measurements. A two-sided p value ≤0.05 was used to establish the threshold of statistical significance.
Results
Demographics
The demographic variables were unchanged from baseline to the 24-week follow-up (table 1). BMI in the sixteen VO2max-tested participants at 24 weeks was 39.4 (33.3-45.7) and 39.0 (35.1-43.0) in the HIIT and the control group, respectively, and BMI remained unchanged throughout all study timepoints.
Demographics of the participants at baseline
Sleep data
There was no significant between-group difference in AHI, self-reported daytime sleepiness (Epworth score), mean oxygen saturation or oxygen desaturation events at 24 weeks (table 2). The number of CPAP users is reported in table 1. The rate of self-reported CPAP use remained constant throughout the study. In the control group, AHI was reduced by 8.7 events/h1 (p=0.046) from baseline to 24 weeks.
Sleep evaluation
Cardiopulmonary exercise testing
Sixteen participants underwent VO2max testing at the 24-week follow-up (HIIT n=9, CON n=7). Reasons given by those who dropped out of the testing were lack of motivation and lack of time. There was no significant difference in VO2max between the groups at 24 weeks (table 3). The ~2 mL/kg/min increase in VO2max from baseline to 12 weeks in the HIIT group was preserved at 24 weeks in the tested participants.7
Maximal oxygen uptake and self-reported physical activity
Self-reported physical activity
At the 24-week follow-up, two participants in the HIIT group reported having continued with regular HIIT after the supervised exercise intervention. The remaining participants in the HIIT group reported regular moderate-intensity exercise (n=5) or limited/no regular exercise (n=6). From the IPAQ data on self-reported physical activity, we found no statistical differences between-groups in self-reported weekly minutes of walking, moderate physical activity, vigorous physical activity or total activity in MET-min/week at 24 weeks (table 3). As not all the participants turned in the IPAQ data material at all study timepoints, these data serve as an indication of trends in participants’ physical activity, and they must be interpreted with some caution.
Discussion
The main finding of this study was that at the 24-week follow-up—12 weeks after the training intervention was completed—there were no differences between the HIIT group and the control group in AHI or in Epworth sleepiness score. We, therefore, conclude that the 12-week exercise training effect on measures of sleep apnoea was lost after 12 weeks without supervised HIIT.7 The 24-week results underscore previous findings in a long-term follow-up study demonstrating that greater lifestyle changes, or long-lasting interventions and follow-up, are needed in order to slow the progression of the burden of OSA through lifestyle changes.17 Some long-term follow-up studies of supervised laboratory-based or clinic-based HIIT in cardiovascular disease patients show low to moderate adherence to exercise training,14 16 27 others show that physical fitness and physical activity are maintained and that patients meet the recommended levels of moderate physical activity 1 year after a 12-week programme of either supervised HIIT or moderate continuous training.15 In addition, home-based HIIT cardiac rehabilitation shows the most promise for long-term adherence after the intervention period.13
Sustaining motivation beyond the intervention period is a challenge with exercise training interventions. Most of the participants in the HIIT group reported not continuing HIIT after the supervised exercise period, and based on the IPAQ questionnaire, there were no significant differences between the groups in physical activity from 12 weeks to 24 weeks. Future studies should examine the exercise intensity, mode and volume that is most likely to achieve long-term adherence to regular exercise in patients with OSA.28
In the HIIT group, AHI and nightly O2-desaturation events returned to baseline values at 24 weeks. As the majority of the HIIT participants reported less regular high-intensity exercise at the 24-week follow-up, the favourable effects of 12 weeks of HIIT on sleep apnoea were most likely lost during the follow-up period, due to less structured exercise training.7 However, given the small number of participants, we cannot rule out that other lifestyle changes, or random variations in the single night of respiratory polygraphy, might have influenced the results. There was also no change in BMI from baseline in the participants who underwent VO2max testing at 24 weeks; therefore, changes in body composition is unlikely to be explanatory factor behind the changes in respiratory measures during sleep.6 9 The improvement in self-reported daytime sleepiness in the HIIT group from baseline to 12 weeks7 persisted at 24 weeks. We speculate that this might be due to a carry-over effect from the supervised HIIT, as regular exercise is reported to have a moderate beneficial effect on sleep quality.28
With few studies investigating the relationship between physical fitness (ie, VO2max) and sleep, it is somewhat unclear how the former may mediate the relationship between regular exercise and sleep.28 Possible explanatory effects of exercise on sleep discussed in the literature include improved fitness levels, changes in body composition, and changes in night-time heart rate variability and metabolism.29 In addition, patients with OSA who exercise are less likely to complain about poor sleep quality than non-exercisers.30 The correlation between sleepiness and OSA severity is found to be poor,30 as demonstrated in a study on exercise and diet that found significant weight loss and improvement in daytime sleepiness without changes in AHI.31 As discussed in extant literature,7 night-time neck fluid accumulation may increase AHI; this could be reduced with physical activity, which leads to less retention of leg fluid that can shift to the neck during sleep.32 33
Despite randomised assignment to the study groups, AHI was higher in the control group than in the HIIT group at baseline, and the mean AHI was in the severe OSA category; therefore, we cannot rule out that the change over time in this group could be due to a regression towards the mean effect due to high baseline levels, or to a Hawthorn effect, with study participation stimulating increased focus on a healthy lifestyle and thereby potentially positively affecting AHI and nightly O2-desatutation events over time. This is supported by indications of increased self-reported physical activity from baseline to 12 weeks and 24 weeks in some control group participants (n=10), which might have improved AHI in the control group at 24 weeks. However, with so few participants and only partial data on physical activity throughout the study, the results should be interpreted with caution. A previous long-term follow-up study focusing on weight reduction reported no change in AHI in the control group at 3 months and 1 year. For the 32% of the patients in the control group who had improved AHI at 3 months, this was maintained at the 1-year follow-up. Furthermore, in the total study population, changes in AHI during the 12 months of follow-up were strongly associated with weight reduction.34
Strengths and limitations
The strength of the study is its randomised controlled design with a postintervention follow-up at 24 weeks—12 weeks after the intervention period—at which we measured both respiration during sleep and subjective daily sleepiness (Epworth scale). The study is limited by its few participants and possible low statistical power. The lack of stratification during randomisation allowed for a significantly higher baseline AHI in the CON group compared with the HIIT group. In addition, out of the 30 included participants, only 26 completed sleep quality testing at the 24-week follow-up and only 16 participants completed the VO2max testing. With partial dropout in various phases of the study, selection bias towards exercise testing cannot be ruled out, and the results should, thus, be interpreted with caution. Objectively measured physical activity throughout the study could have strengthened the study by limiting bias in self-report of physical activity. Also, the CPAP equipment used in the present study did not automatically record time in use: instead, this was self-reported by the participants and could allow for some bias.
Conclusion
The effect of 12 weeks of supervised high-intensity exercise training on the AHI and on self-reported daytime sleepiness was lost at the 24-week follow-up.
Data availability statement
No data are available. The ethical approval does not support sharing of data.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Regional Medical Research Ethic Committee Number: 2010/1539. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are deeply grateful to the unit for applied clinical research at the medical faculty at NTNU, for supplying the webCRF randomisation database; to the SINTEF-Unimed foundation, for partly funding this study; and to research nurses Marit Tjelle Setvik and Anne Stine Fossum, for assistance with data collection. In addition, we are deeply grateful to our research participants for giving their time to participate in the study.
References
Footnotes
Contributors TK is as the fort author responsible for the overall content of the publication. All authors meet the criteria for authorship defined by the International Committee of Medical Journal Editors.
Funding The study was funded by the SINTEF-Unimed foundation and the Norwegian University of Science and Technology (NTNU).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.