Article Text

Abstract
Objectives To investigate the association and utility of blood plasma markers of neurodegeneration in a population of retired athletes self-reporting multiple concussions throughout a sporting career. It is hypothesised that this type of athletic history would cause an increased prevalence of neurodegenerative disease, as detected by biomarkers for neurodegenerative disease processes.
Methods One hundred and fifty-nine participants were recruited (90 males, 69 females, mean age 61.3±9.13 years), including 121 participants who had retired from playing professional or semiprofessional sports and self-reported ≥1 concussion during their careers (range 1–74; mean concussions=10.7). The control group included 38 age-matched and sex-matched controls, with no history of concussion. We measured neurofilament light (NfL) and tau (neurodegeneration markers), glial fibrillar acidic protein (GFAP) (astrocytic activation marker) and 40 and 42 amino acid-long amyloid beta (Aβ40 and Aβ42) (Alzheimer-associated amyloid pathology markers) concentrations using ultrasensitive single molecule array technology.
Results We found retired athletes reporting one or more concussions throughout an athletic career showed no significant changes in NfL, tau, GFAP and Aβ40 and Aβ42 concentrations in comparison to a control group. No correlations were found between biomarkers and number of concussions (mean=10.7). A moderate correlation was found between NfL concentration and age.
Conclusion No difference in blood concentrations of neurodegeneration markers NfL, tau, GFAP and Aβ40 and Aβ42 was found in retired athletes with a history of concussion compared with controls. An increased prevalence of neurodegenerative diseases is not detected by biomarkers in a population self-reporting multiple concussions.
Trial registration number ISRCTN 11312093
- Concussion
- Athlete
- Brain
- Horse racing
Data availability statement
Data are available upon reasonable request. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Little is known about neurofilament light, tau, glial fibrillar acidic protein and Aβ40 and Aβ42 blood plasma concentrations many years after competing in sports that carry a risk of concussion/mild traumatic brain injury. This study was done to assess whether experiencing repetitive concussions throughout an athlete’s lifetime leads to any changes in various biomarker concentrations that may indicate an increased risk of long-term neurodegenerative disease.
WHAT THIS STUDY ADDS
This study found no significant differences in any of the biomarker concentrations between retired athletes with concussion and a control group without a history of concussion.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our study does not refute that lifetime concussions may induce neurodegeneration and/or reduce resilience to neurodegenerative disease, but the usefulness of fluid biomarkers alone as a predictor of long-term neurodegenerative disease risk may be limited.
Introduction
Multiple concussions/mild traumatic brain injury (mTBI) or repetitive subconcussive head impact in athletes is a growing concern due to an association with impaired mental health, cognitive impairment and increased risk of neurodegenerative disease.1–3 There is evidence of a link between moderate-severe TBI in young adults and Alzheimer’s disease and other dementias later in life.4 Gavett et al5 suggest the possibility that repetitive mTBI resulting in axonal injury can result in Alzheimer’s disease, frontotemporal dementia or chronic traumatic encephalopathy in later life.
To protect the brain health of athletes at risk of mTBI, it is important that the risks of concussion are carefully considered and that danger to the athlete should be reduced whenever possible.6 7 Demands to ban sports with a risk of concussion remain controversial due to the gaps in our knowledge surrounding the potential negative effects of concussion and the proven advantages of sports participation.6 Furthermore, many athletes never acquire neurodegenerative disorders throughout their careers.8
This study uses single molecule array (Simoa) technology, which is a supersensitive immunoassay technology that allows us to measure proteins that give information about neuronal health using serum or plasma as the biofluid. We measured neurofilament light (NfL), a biomarker of large-calibre myelinated axon damage, glial fibrillar acidic protein (GFAP), which is a biomarker of astroglia cell damage, and tau, which is a biomarker of thin non-myelinated axon damage.9 Amyloid beta 1-40 (Aβ40) and amyloid beta 1-42 (Aβ42) are markers of amyloidogenic amyloid precursor protein processing, which is upregulated on axonal injury and can result in the formation of diffuse amyloid plaques that may be related to onset of amyloid aggregation typical of Alzheimer’s disease.9
Most studies investigating blood biomarkers after concussion collect samples within a short time period (days to months) after injury.10–15 No study to our knowledge has looked at this combination of blood plasma biomarkers after a period of years in retired athletes participating in various sports with a risk of concussion. However, Di Battista et al16 used a similar approach by grouping athletes who competed in collision sports, but only assessed tau concentrations. It is hypothesised that this type of athletic history used in this study would cause an increased prevalence of neurodegenerative disease, as detected by biomarkers for neurodegenerative disease processes, compared with a control group.
Aim
To investigate NfL, tau, GFAP and Aβ40 and Aβ42 fluid biomarker concentrations in plasma of retired athletes who have competed in sports with a risk of concussion in comparison to a control group with no reported concussions.
Methodology
Participants
Participants were initially sought through a widely advertised study and invited to complete an online screening process. Participants responded to a detailed online questionnaire regarding self-reported concussion history, mood, sleep and physical and mental health status (online supplemental file 1) . From the database of completed questionnaires, participants with a history of concussion were matched to control participants with no history of concussion of the same age and sex. All the participants in the concussion group participated at a ‘professional or semi-professional’ level in their primary adult sport. The control group were active and played recreational sports with no self-reported history of concussion. Volunteers were all functioning normally in the community with no clinical evidence of neurodegenerative disease and were of a sound mind capable of leading an independent life. Participants with a history of concussion and their age-matched and sex-matched controls were then randomly selected for more detailed screening, including neuropsychological assessment and neuroimaging in London, UK. All the volunteers were interviewed to ensure their concussion history was recorded correctly.
Supplemental material
Recruitment was via publicity in sports-related media with 1200 volunteers enquiring to enrol into the study. Questionnaires were sent with 787 completed and included in the final cohort database. The physical screening on volunteers was initially focused on residents in England, Scotland or Wales and who were over the age of 55 (a total of 189 volunteers). To obtain statistical significance, it was estimated that a target total of 250 screened subjects was needed, so the invitation was extended to those aged 50–54 (an additional 129 volunteers). All 318 volunteers were invited to attend a screening day in London of which 32 declined. Of the remaining cohort, 166 were finally screened before COVID-19 prevented travel and screening. After this process, 159 samples were obtained for blood plasma biomarker concentration analysis.
Inclusion criteria: Participants were eligible to participate if they (1) participated but were then retired from their primary sport; (2) were able to complete the online screening assessment; (3) could understand and participate in the testing procedures; and (4) were able to provide informed consent for their participation.
Exclusion criteria: Participants were ineligible if they were aged <18 years; had a history of severe TBI; were currently taking sedative or psychotropic medication; or a pre-existing medically diagnosed neurological disorder (eg, Alzheimer’s dementia, Parkinson’s disease, multiple sclerosis, motor neuron disease).
Sample collection and measurements
Five millilitres of blood was collected from each participant in plasma EDTA tubes. Samples were centrifuged at 2000g and plasma aliquoted and stored at −80° until assay. NfL, tau, GFAP and Aβ40 and Aβ42 were measured on the Simoa HD-X platform (Quanterix, Billerica, Massachusetts) according to the manufacturer’s instructions. Briefly, plasma samples were diluted fourfold and then incubated with paramagnetic beads coated with anti-Aβ40, anti-Aβ42, anti-GFAP, anti-NfL or anti-tau antibodies and biotinylated detector antibodies. Beads were washed and combined with a conjugate of streptavidin-b-galactosidase. This enzyme binds to biotinylated antibodies; bound enzyme is hydrolysed by resorufin-b-D-galactopyranoside producing a fluorescent signal that is read by the analyser. Calibrators run on the same assay produce a standard curve, enabling quantification of samples. All samples were analysed on one occasion using one batch of reagents; intra-assay coefficients of variation were below 10%. The number of results for each biomarker differs as a number of measurements can be lost due to technical issues or sample quality. In the control group, the number of measurable samples was tau (n=37), GFAP (n=38), NfL (n=38), Aβ40 (n=38) and Aβ42 (n=37). In the concussion group: tau (n=121), GFAP (n=119), NfL (n=119), Aβ40 (n=119) and Aβ42 (n=117).
Data analysis
The data were uploaded to Microsoft Excel and GraphPad Prism V.9.0 (GraphPad) for analysis. A Shapiro-Wilk test was used to assess the normality of the data. Post hoc analysis using a Mann-Whitney U test was used to compare biomarker concentrations between the concussion group and the controls. An unpaired t-test was used for the comparisons of the demographics between groups. The Pearson correlation coefficient was used for analyses of correlation between various biomarker concentrations and variables (the number of concussions reported and age). An analysis of variance test was used to test the significance of correlations. Significance was set at p<0.05.
Patient and public involvement
Participants and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
From this process, one hundred and fifty-nine participants were recruited (90 males, 69 females). This included 121 retired athletes who had experienced at least one concussion (basketball, boxing, cricket, cycling, equestrian, football, horse racing, motor sports, martial arts, rugby league, rugby union, sailing, shooting, skiing, trapeze). Thirty-eight age-matched and sex-matched controls, who did not report having had any concussions, were also screened. All the controls came from the same online registry. See table 1.
Values are mean±SD
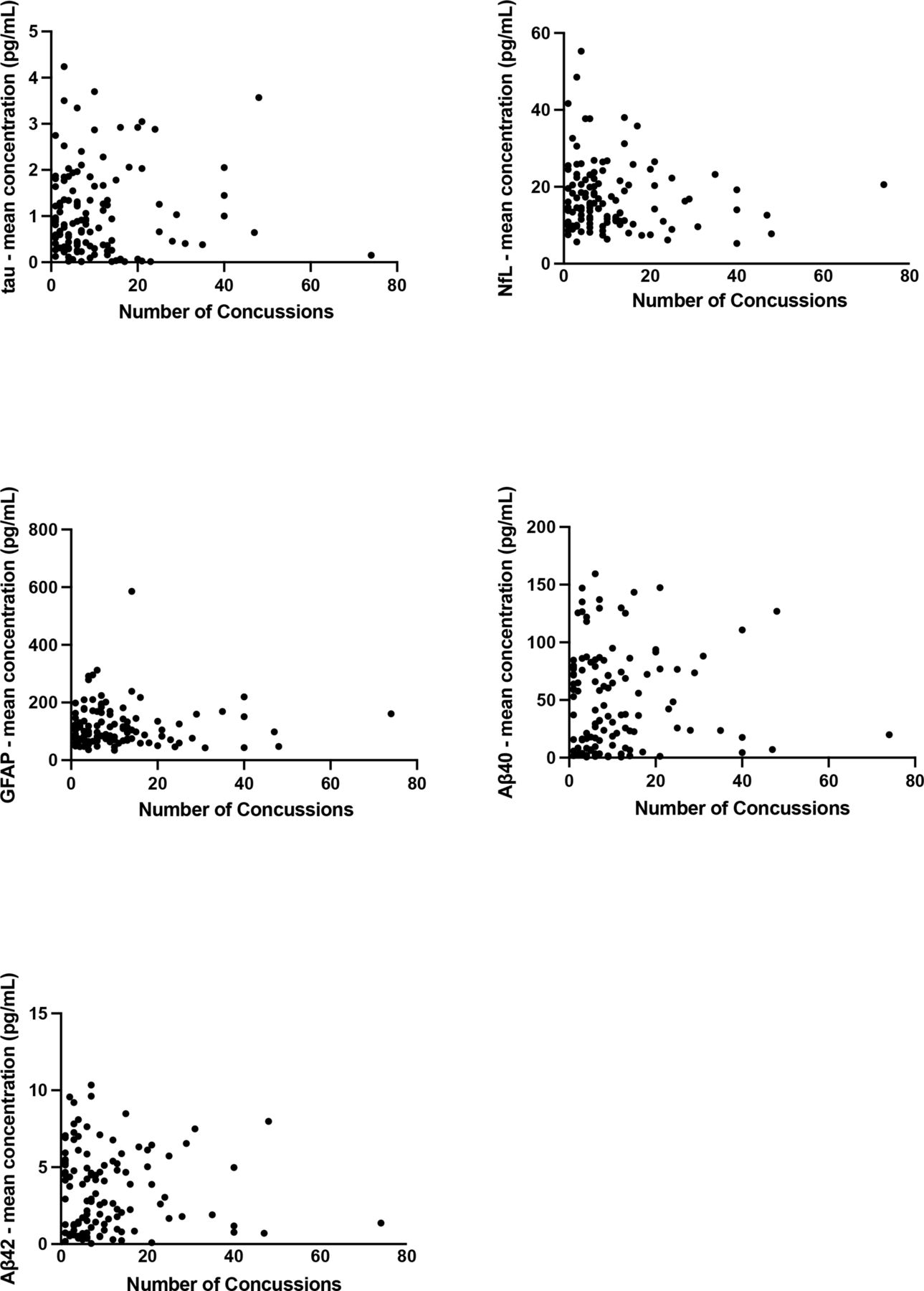
No significant differences were found in fluid biomarker concentrations between the control group and the retired athletes with a history of self-reported concussion (table 2). No association was found between each of the biomarkers and the number of concussions in the concussion group, tau r (0.04), GFAP r (−0.01), NfL r (−0.11), Aβ40 r (0.01) and Aβ42 r (−0.03) (figure 1). However, we found a moderate correlation between age and NfL concentration (r=0.44, p<0.001) and a weak correlation for GFAP (r=0.36, p<0.001) (figure 2). No associations were found between age and tau, Aβ40 or Aβ42 concentrations (p>0.05). The sex differences were also analysed between the controls and the participants with one or more self-reported concussion. No significant differences were found in males or females (table 3).
Values are median and IQR
Values are median and IQR
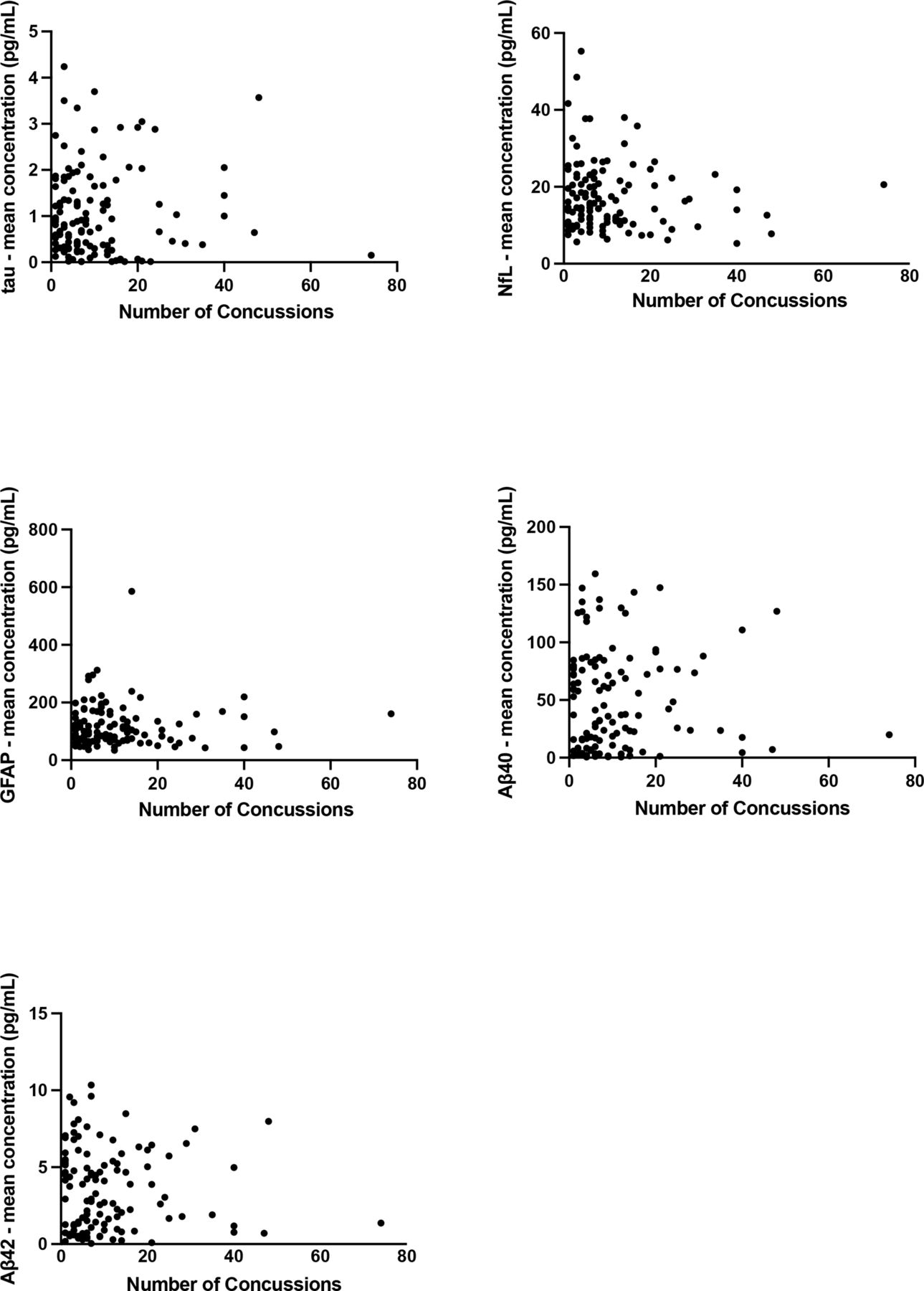
Correlation of plasma biomarker concentration versus the number of concussions the participant self-reported. No significance was found. GFAP, glial fibrillar acidic protein; NfL, neurofilament light.

{kind=link}
{kind=link}
Correlation of plasma biomarker concentration versus the age of the participant at the time of testing. An analysis of variance (ANOVA) test showed a significant positive correlation between glial fibrillar acidic protein (GFAP) and neurofilament light (NfL) against age.
Discussion
Main findings
This study found that retired athletes with a history of self-reported concussion (mean±SD 10.7±11.5) did not have a significant increase in biomarkers for neurodegeneration (NfL and tau), astrocytic activation (GFAP) or amyloid aggregation (plasma Aβ42/Aβ40) compared with a control group without reported concussions. The participants were retired from sport but functioning normally in the community without clinical evidence of neurodegenerative disease.
Neurofilament light
Several previous studies have shown that NfL can be regarded as a global marker of neurodegeneration due to elevated concentrations being present in frontotemporal dementia,17 Alzheimer’s disease,18 Huntington’s disease19 and other neurodegenerative disease.20 It has also been reported that serum NfL was elevated in amateur boxers 3 months after a bout of boxing in comparison to the control group.12 Similarly, NfL blood concentration has been shown to increase during the season in American football players.13 This implies that NfL could potentially be used as a marker of ongoing neuroaxonal injury secondary to repeated concussion.21 In our study, we did not find any difference in plasma NfL concentration between the two study groups. This may suggest that retired athletes with a history of concussions did not have a higher prevalence of neurodegenerative disease, as measured by plasma NfL or that increases in NfL related to acute brain injury may not be persistent in plasma over time.
Tau
Elevated blood plasma tau concentrations have been previously shown to be linked with neurological conditions including Alzheimer’s disease.22 23 Furthermore, exosomal tau has shown the potential to be a chronic traumatic encephalopathy biomarker in retired NFL players.24 When tau concentrations are raised, it suggests that axonal injury has occurred and can be seen in peripheral blood of professional boxers and ice hockey players within a short period after the event.10 11 However, the half life of tau in blood is short (around 10 hours), and Neselius et al10 did find that after 14 days plasma tau concentrations were no longer significantly different from the controls. Nevertheless, in a study involving retired American football athletes it has been shown that greater exposure to repetitive head impacts correlated with elevated later life plasma total tau concentrations.25 Similarly, Di Battista et al16 found in male university-level athletes that plasma tau concentrations were significantly higher in collision sport athletes in comparison to non-collision sport athletes with samples collected at the start of the competitive season, although this was not seen in females. Also, when plasma tau concentrations were evaluated in combination with collision sport involvement, biomarker variability was not impacted by the athletes’ concussion history and found to be a non-significant influence.16 Therefore, Di Battista et al16 suggested that a larger biological response may be evoked from frequent subconcussive hits due to collision sport involvement than reported concussion. Kenney et al26 found higher plasma tau concentration in military personnel with a history of TBI. This was shown particularly in military personnel who have reported more than three TBIs throughout their deployment or with a medical diagnosis of TBI.26 Kenney et al’s26 study was also similar to our study, limited due to the self-reporting of the TBIs. Olivera et al14 also conducted a study testing retired military personnel many years after injury. Furthermore, it was found that total tau concentration was found to be elevated in the military personnel which reported multiple TBIs. Similarly, Olivera et al14 and our present study are both limited due to the highly variable time from testing to the occurrence of the last TBI/mTBI. Although, this present study disagrees with these findings, this could be due to mTBI/concussions experienced in our study which are not as damaging as TBIs used in Kenney et al26 and Olivera et al’s14 studies of military personnel.
Glial fibrillar acidic protein
Blood GFAP concentrations have been shown to be greater in participants with Alzheimer’s disease, Parkinson’s disease dementia and dementia with Lewy bodies in comparison to controls.27 Only a few studies have researched GFAP concentrations in blood plasma in regard to assessing neurodegenerative diseases; therefore, more investigation is needed for complete clarity.28 29 Bogoslovsky et al15 found that in a cohort predominately with mTBI, they were able to differentiate plasma GFAP levels from uninjured controls. Furthermore, it was found that although GFAP levels declined over the first few weeks following injury, they stayed increased for up to 3 months in a subgroup of patients when compared with undamaged controls.15 However, little research has been done long term. No studies, to our knowledge, have assessed blood plasma concentration of GFAP many years after injury, which this study accomplishes.
Amyloid markers: Aβ40 and Aβ42
Elevated blood plasma Aβ42 concentrations have been linked to long-term neurodegenerative conditions, including Alzheimer’s disease.30 Kenney et al26 compared participants with ≥3 mTBIs to participants with one to two mTBIs and the TBI-negative controls and found no significant differences between groups for Aβ40 and Aβ42. This is reflected in the present study, the results of which speak against a higher prevalence of Aβ pathology in the brains of the exposed subjects.
Strengths and limitations
The major strength of this study is that a large range of participants was used from many sporting backgrounds, including many female participants. Also, the concussion group included a high mean total of concussions in comparison to similar studies assessing sport concussion/mTBI.
The validity of the participants’ concussion history is limited due to it being self-reported. However, it was not possible to gather the participants’ clinically diagnosed concussion history due to fragmented documentation. Another limitation of the study was that although the control group was recreationally active, they were not retired athletes. Also, these concussions occurred prior to current concussion guidelines. This study is also limited due to the highly variable time between participants from the last concussion received and the time of sample collection. This data is not available to publish. It is also possible that the age range analysed may be a time window prior to any clinical deterioration; therefore, a follow-up study looking at this cohort at multiple time points in their life is critical.
Conclusion
This study found no difference in blood concentrations of the neurodegeneration markers NfL and tau, as well as the astrocytic activation GFAP and biomarkers for amyloid plaque formation (plasma Aβ42/Aβ40 ratio), in athletes with a history of multiple concussions in comparison to controls. No correlation was found between the number of concussions experienced and any of the measured biomarkers.
Data availability statement
Data are available upon reasonable request. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained from St Mary’s University, Twickenham, London, UK on 1 June 2015, SMEC_2015-16_53, SMEC_2016-17_115 and SMEC_2017-18_051.
Acknowledgments
The ICHIRF project is currently philanthropically funded by Godolphin Racing, the Injured Jockeys Fund (UK), the Irish Injured Jockeys Fund, the Professional Footballers Association (UK), the NFL (USA), the Concussion Foundation, the Racing Foundation, the British Association of Sport and Exercise Medicine as well as private donations. The ICHIRF-BRAIN Study would not be possible without the input of the ICHIRF project manager, Pippa Theo.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The conception and design of the project originated from MT and HZ. MT/International Concussion and Head Injury Research Foundation (ICHIRF) provided the demographic data and the blood samples. Acquisition, analysis and interpretation of data were completed by AH, OJS and HZ. OJS drafted the manuscript. HZ, MT, AH and OJS critically reviewed and revised the manuscript for intellectual content. HZ, MT, AH and OJS approved and agree to be accountable for the final version of the manuscript. HZ was the guarantor of this study.
Funding This study was funded by UK Dementia Research Institute (UKDRI-1003).
Competing interests MT is employed as CEO and Medical Director of the International Concussion and Head Injury Research Foundation (ICHIRF) and was formerly employed as the Chief Medical Adviser to the British Horseracing Authority (BHA) and the Lawn Tennis Association (LTA). He is Honorary Medical Adviser to the Professional Jockeys Insurance Scheme (PRIS) for which he receives a discretionary honorarium. ICHIRF is a not-for-profit organisation. He undertakes no clinical duties but has been reimbursed for travel and accommodation at conferences, symposia and scientific meetings by the organisers. He does not hold any shares in any company related to concussion or brain injury assessment or technology. HZ has served at scientific advisory boards and/or as a consultant for AbbVie, Alector, Annexon, Artery Therapeutics, AZTherapies, CogRx, Denali, Eisai, Nervgen, Pinteon Therapeutics, Red Abbey Labs, Passage Bio, Roche, Samumed, Siemens Healthineers, Triplet Therapeutics and Wave; has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure, Biogen and Roche; and is a co-founder of Brain Biomarker Solutions (BBS) in Gothenburg, which is a part of the GU Ventures Incubator Program (outside submitted work). HZ is a Wallenberg Scholar supported by grants from the Swedish Research Council (2018-02532), the European Research Council (681712), Swedish State Support for Clinical Research (ALFGBG-720931), the Alzheimer Drug Discovery Foundation (ADDF), USA (201809-2016862), the AD Strategic Fund and the Alzheimer’s Association (ADSF-21-831376-C, ADSF-21-831381-C and ADSF-21-831377-C), the Olav Thon Foundation, the Erling-Persson Family Foundation, Stiftelsen för Gamla Tjänarinnor, Hjärnfonden, Sweden (FO2019-0228), the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement number 860197 (MIRIADE), European Union Joint Program for Neurodegenerative Disorders (JPND2021-00694) and the UK Dementia Research Institute at UCL.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.