Article Text

Abstract
Objectives To systematically review studies evaluating one or more components of physical fitness (PF) in pregnant women, to answer two research questions: (1) What tests have been employed to assess PF in pregnant women? and (2) What is the validity and reliability of these tests and their relationship with maternal and neonatal health?
Design A systematic review.
Data sources PubMed and Web of Science.
Eligibility criteria Original English or Spanish full-text articles in a group of healthy pregnant women which at least one component of PF was assessed (field based or laboratory tests).
Results A total of 149 articles containing a sum of 191 fitness tests were included. Among the 191 fitness tests, 99 (ie, 52%) assessed cardiorespiratory fitness through 75 different protocols, 28 (15%) assessed muscular fitness through 16 different protocols, 14 (7%) assessed flexibility through 13 different protocols, 45 (24%) assessed balance through 40 different protocols, 2 assessed speed with the same protocol and 3 were multidimensional tests using one protocol. A total of 19 articles with 23 tests (13%) assessed either validity (n=4), reliability (n=6) or the relationship of PF with maternal and neonatal health (n=16).
Conclusion Physical fitness has been assessed through a wide variety of protocols, mostly lacking validity and reliability data, and no consensus exists on the most suitable fitness tests to be performed during pregnancy.
PROSPERO registration number CRD42018117554.
- Gestation
- Physical activity
- Fitness testing
- Women
- Pregnancy outcomes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already knownWHAT IS ALREADY KNOWN ON THIS TOPIC
The assessment of physical fitness during pregnancy requires special considerations to preserve fetal and maternal health.
Although physical fitness during pregnancy has been assessed inconsistently across studies, these tests have not been systematically compiled to date.
The validity and reliability of the variety of tests used to assess physical fitness during pregnancy has not been comprehensively reviewed.
WHAT THIS STUDY ADDS
During pregnancy, physical fitness including cardiorespiratory fitness, muscular strength, flexibility and balance have been assessed inconsistently, using a wide variety of protocols.
Most of the tests used to assess physical fitness during pregnancy lack validity and reliability data.
Higher physical fitness might be associated with better maternal and neonatal health, although further research is needed.
HOW THIS STUDY MAY AFFECT RESEARCH, PRACTICE AND POLICY
The extent to which the data derived from current physical fitness tests during pregnancy is valid and reliable is still unclear and, therefore, should be interpreted with caution.
Developing a battery of fitness tests to assess the different fitness components during pregnancy must be set as a priority for relevant institutions.
An expert consensus to develop a battery of physical fitness tests is recommended.
Background
Physical fitness (PF) has been defined as the ability to carry out daily tasks with vigour and alertness, without undue fatigue and with ample energy to enjoy leisure-time pursuits and meet unforeseen emergencies.1 2 PF is considered a powerful marker of health that is associated with a lower risk of cardiovascular events, cancer and all-cause mortality in all ages.3–7 In pregnant individuals, some studies have recently highlighted the potential impact of PF on maternal and fetal health.8–15 Low PF levels are associated with low infant birth weight,8 increased risk of gestational diabetes mellitus,9 10 poor postpartum recovery11 and worse delivery outcomes.12 13 Moreover, the anatomical, biomechanical, physiological and psychological changes during the pregnancy might compromise PF levels.16–18 Consequently, it is of clinical and public health interest to assess PF during the pregnancy, and to understand which available tests are best to assess PF during this critical period of life.
Two categories of PF components have been defined as follows: (1) health-related components (cardiorespiratory fitness (CRF), muscular fitness, muscular endurance and flexibility) and (2) skill-related components (ability, coordination, balance, power, reaction time and speed).1 2 These PF components can be assessed subjectively through questionnaires,15 objectively and accurately through laboratory tests and efficiently, economically and easily through field-based tests. During the pregnancy, a wide variety of fitness tests have been used to assess PF, although a compilation of these tests has not been published to date. Compiling all fitness tests performed in pregnant women would help practitioners to select the most useful test according to their purpose. It is also important to note that, although laboratory tests are generally the gold standard for assessing PF, these tests are not accessible to everyone because they need sophisticated and expensive equipment, and it is not possible to evaluate a relatively large sample in a short period of time. As an alternative, a number of field tests exist that provide an opportunity to assess PF in a more accessible way.2 However, there is no consensus on which fitness tests should be used to assess PF in pregnant individuals, and the validity and reliability of many of the tests used to assess PF during the pregnancy are unknown.19
Since the assessment of PF in pregnancy requires special consideration to preserve fetal and maternal health,18 20 21 understanding which fitness tests are valid, reliable, and associated with maternal and neonatal health outcomes, would provide a framework for improving PF assessment during pregnancy and also for improving exercise prescription in this population.
The aims of this systematic review were to: (1) describe which fitness tests have been used to evaluate PF in pregnant individuals; and (2) to evaluate the validity and reliability of the fitness tests, and their relationship with maternal and neonatal health.
Methods
Registration and review guidelines and checklist
This systematic review was prospectively registered at PROSPERO (CRD42018117554; available at http://www.t.ly/fS6a). In addition, the review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines22 and the PRISMA checklist23 is included as online supplemental material 1, table S1. (1) .
Supplemental material
Search strategy
Articles were searched by two independent reviewers from two major databases, MEDLINE (PubMed) and the Web of Science (WOS) from inception to January 2021. For the search strategy undertaken in PubMed Medical Subject Heading, (MeSH) terms were used. All terms were combined using the connector OR for similar criteria the connector ‘AND’ was used to combine population group (ie, pregnant women), to delimit date of publication (‘0001/01/01’(PDat): ‘2021/01/15’(PDat)), to include full text papers, and to include studies performed in humans.
A similar search strategy and term combination was undertaken in the WoS (online supplemental material 2, table S2), although MeSH terms and its appropriate terms connection were not used as they are exclusive for PubMed. The complete search strategy and further details are presented in online supplemental material 2, tables S1 and S2.
Inclusion criteria
The inclusion criteria were as follows: (1) healthy pregnant individuals (no restriction regarding gestational week); (2) at least one component of PF assessed either through field based or laboratory tests; (3) access to full text; (4) only one original article from the same study/project using the same test were included and (5) text in English or Spanish.
Quality assessment of the articles
To assess quality of the articles included in aim 2, three quality scores were applied. To assess validity and reliability, authors adapted two quality scores ad hoc previously used in two different systematic reviews following the same goal as the present review, however, undertaken in different populations.24 25 To assess the association of PF with health-related outcomes the Effective Public Health Practice Project was used.26 All procedures are comprehensively described in online supplemental material 3, tables S3–S5.
Process and data extraction
After checking title and abstract, only the studies meeting all inclusion criteria were introduced in a reference manager software (Mendeley). In the event of disagreement between the two independent reviewers concerning the inclusion/exclusion of an article, a consensus was reached (there was no need of a third person). The snowball strategy was also used. Information including reference, age, sample size and fitness test description are summarised in online supplemental material 5, table S6.
Results
A comprehensive PRISMA flow diagram is presented in figure 1.

Flow chart of the literature search and paper selection process.
Overall results, quality assessment and gestational week
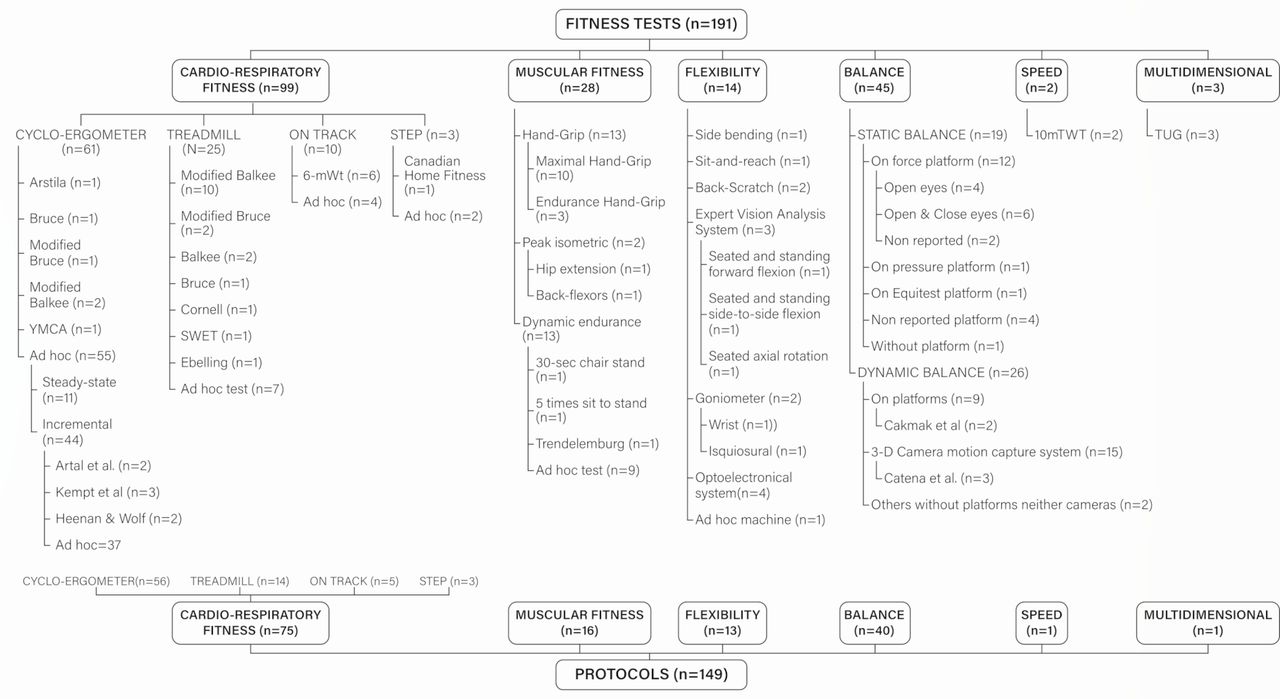
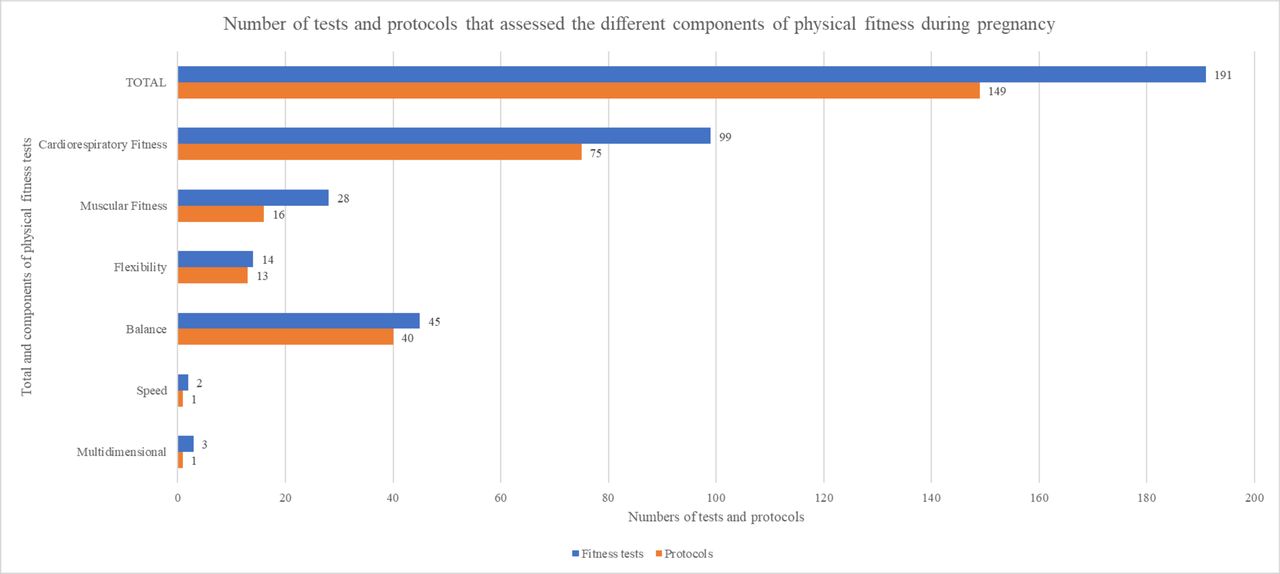
The search identified 2617 studies, of which 149 were included (figure 1). These articles contained 191 fitness tests, using 149 different protocols that were included for Aim 1. A summary of the number of articles that assessed PF during the pregnancy and the protocols used for its assessment is presented in figure 2. This has been organised based on each of the different PF components assessed in those articles. Moreover, a comprehensive diagram of the fitness tests and the different protocols performed to date, organised by PF component, is presented in figure 3.

Number of tests and protocols that assessed the different components of physical fitness during pregnancy.
{kind=link}
{kind=link}
{kind=link}
Diagram of the fitness tests and the different protocols organised by PF component. PF, physical fitness.
Regarding aim 1, 99 tests (including 75 different protocols) were used to assess CRF,8 12 13 18 27–108 28 (including 16 different protocols) to assess muscular fitness,8 12 13 61 86 109–122 14 (including 13 different protocols) to assess flexibility,12 13 110 114 123–127 45 tests (including 40 different protocols) to assess balance,110 116 128–167 2 tests using the same protocol to assess speed168 169 and 3 tests using the same protocol were multidimensional.168–170 No results were found for other PF components such as agility or coordination.
Regarding aim 2, a total of 19 articles (13% of the total number of articles included) assessed at least validity (n=3) and reliability (n=4) of fitness tests. These articles are summarised in table 1. Of the three articles74 75 169 that assessed validity, two articles were classified as low quality74 169 and one as high quality.75 Of the four articles that assessed reliability criteria, three were considered high quality74 117 168 and one low quality.121 The relationship of PF with maternal and neonatal health outcomes (n=16 tests) are summarised in table 2. Of these 16 tests, 11 were classified as very low quality13 57 68 95 108 111 126 157 158 and 5 were classified as low quality.8 63 115 128 170
Overview of studies that assessed the validity and/or reliability of fitness tests during pregnancy
Summary of studies assessing PF and its relationship with maternal and neonatal health outcomes
The gestational week at PF assessment ranged from 8 to 41 across articles. Some articles assessed PF at different time points throughout pregnancy; therefore, we divided pregnancy into two stages. Early pregnancy (ie, from week 0 to week 20 of gestation) and late pregnancy (ie, from week 21 to week 40). Using this approach, 11 articles (7%) were performed in early pregnancy; 57 articles (38%) were performed in late pregnancy; 55 articles (37%) were performed several times (ie, range 2–5 times) throughout pregnancy; 7 (5%) articles specified a range of weeks that included early to late pregnancy; 14 articles (9%) reported only the trimester without specifying gestational week; 4 articles (3%) provided no information and 1 article (1%) assessed PF on the day of labour.
Aim 1: fitness tests used to evaluate PF in pregnant women
Cardiorespiratory fitness
We identified 99 tests assessing CRF, of which 61 (62%) were performed on a cycle ergometer, 25 (25%) on a treadmill, 10 (10%) on a track and 3 (3%) used step protocols (figure 3). Of the 99 tests, a total of 75 corresponded to different protocols. For instance, there were 56 different protocols using a cycle ergometer, distributed as follows: only one article used the Arstila test68; one used the Bruce Protocol at 75% HRmax27; one applied the Modified Bruce ramp protocol at anaerobic threshold104; two employed the Modified Balke protocol at 70% HRmax34 41; one used a YMCA protocol;106 The remaining of articles (n=55) used ad hoc tests (ie, specifically designed for the purpose of the investigation); 11 of which32 37 38 41 45 57 64 79 107 used steady-state tests and 4428–31 33 35 36 39–41 43 44 46–56 59–63 65–69 90 100–106 108 171–173 used incremental tests. When analysing the type of test based on intensity, we found that 13 tests were maximal tests,31 43 44 47–49 59 60 67 103–105 171 37 submaximal tests29 30 35–40 42 45 46 50–52 54–57 62–66 68 69 79 90 100–102 106 108 172 and 3 used mixed tests28 33 41 containing submaximal and maximal stages within the same protocol.
There were 25 treadmill tests that used 14 different protocols, distributed as follows: the Modified Balke protocol was used in 10 articles8 31 71 73 75–78 82 96; the Modified Bruce protocol in 2 articles13 97 and the traditional Balke protocol used twice in the same article70; the traditional Bruce protocol,98 the Cornell protocol,74 the SWET protocol and the Ebbelling single-stage protocol18 were each used in one article. There were seven ad hoc tests of which two were steady-state,38 81 and five were incremental tests.72 73 80 83 90 According to intensity, three were maximal tests73 80 81 and four submaximal tests.38 72 83 90
Of the 10 tests performed on a track, 6 articles used the 6 min walk test protocol,84 85 87–89 92 and 4 were ad hoc tests (ie, maximal and 4 were submaximal). With regard to the three step tests, one Canadian Home Fitness test93 was used and two ad hoc incremental submaximal tests were used.94 95
Muscular fitness
A total of 28 tests (ie, 14% of all included articles) that included 16 different protocols assessed muscular fitness, of which 10 performed maximal hand-grip strength tests,8 12 13 86 109–115 performed endurance hand-grip tests, 2 for 3 min118 120 and 1 for a 2 min period119 (figure 3). In two of the articles conducting an endurance hand-grip test,118 119 a hand-grip sphygmomanometer was used instead of dynamometry. On the other hand, one used a hand-held dynamometer fixed to a chair to assess quadriceps strength116 and one used a toe-grip dynamometer.116 Moreover, two ad hoc isometric tests were used to assess maximal voluntary hip extension and back flexors endurance in the same article.174 Finally, 13 dynamic endurance tests were found, 9 were listed as ad hoc tests12 112 122 and another 3 (30 s Chair Stand Test, 5 Times Sit to Stand test, Trendelenburg’s test) were classified as ‘other’ dynamic tests.13 112 117
Flexibility
Our search identified 14 (7%) tests that assessed flexibility using 13 different protocols, including the side bending test,125 the sit-and-reach test,12 the back-scratch test (twice),13 110 the motion analysis (ie, including three different tests such as the seated and standing forward flexion, seated and standing side to side flexion and seated axial rotation)123 and an optoelectrical system (ie, performing four different tests).127 Goniometry was used in two different articles to measure hamstring flexibility,114 wrist flexion-extension and medial lateral deviation.124 Only one article used an ad hoc machine to test passive abduction of the left fourth finger.126
Balance
We identified 45 (24%) articles assessing balance of which 19 analysed static balance and 26 used dynamic balance with 40 different protocols. With regard to static balance, 18 were laboratory tests of which 12 assessed balance through stabilometry tests on a force platform,129 131 132 138 149 158–160 162–164 167 one on a pressure platform163 and another on an Equitest platform.165 Four articles did not mention the type of platform used.117 132 133 175 Regarding protocols, all articles conducted the tests with participants standing with bipedal support. However, standing position varied between articles. Ten articles maintained a standing posture with feet separated,116 131 132 147 158 159 162 165–167 one with feet together,129 two used mixed protocols,128 160 one with medial malleoli separated130 and four did not mention the standing posture.138 149 163 164 Moreover, three articles used protocols with eyes open132 149 162 exclusively, eight articles used mixed protocols with eyes open and closed, one used visual target and visual tasks164 and six did not specify whether participants kept their eyes closed or opened. Only one article used a field test, the one-legged standing protocol.110 On the other hand, one test was a field-test without a platform.
In relation to the 26 articles measuring dynamic balance, 9 assessed balance using platforms. Each of these articles used a different testing tool such as a balance master platform.133 pressure platform,163 force platform,135 Equitest platform134 and a movable platform, which was used in two articles.136 137 Two of these articles were walking protocols,135 163 one with translational perturbations,157 one was standing with one knee flexed and arms across the chest.136 137 Another 15 articles used three-dimensional (3-D) camera motion capture systems using 13 different protocols. Twelve of the 15 articles were walking protocols139 140 142–144 148 150 152–156 161 and 2 used a stand to sit motion protocol.141 151 Moreover, one article used a triaxial accelerometer146; another article assessed balance through recording (without specification of camera type)145 and another using instrumented insoles.176 All three of these articles used walking protocols.
Speed
The only protocol that was used to assess speed during pregnancy was the 10 m timed walk test (10mTWT). However, the same test was identified in two different articles.168 169 In the 10mTWT, the participants commenced standing at a chair. When told to start, subjects walked as fast as possible along 14 m marked with white tape placed at 0 m, 2 m, 12 m and 14 m. The time (100th of a second) required to walk between the 2 m and 12 m markers was recorded and converted into speed in metres per second (m/sec).
Agility and coordination
No articles of agility and coordination were identified.
Multidimensional
Our search identified a walking multidimensional test that was used in three studies.168–170 In the Timed Up and Go Test (TUG), the participant began seated in a chair with their arms on armrests and their toes against a start line. The purpose was to cross the front white line at 3 m away, turn around and walk back to the chair and sit down as fast as possible. The performance is measured in time (100th of a second).
Aim 2: evaluation of the validity and reliability of the fitness tests, and their relationship with maternal and neonatal health
Articles assessing validity and reliability are summarised in table 1. Articles assessing PF and its relationship with maternal and neonatal health outcomes are presented in table 2 and follows a similar format as Sallis et al.177
Cardiorespiratory fitness
We identified two articles examining validity.74 75 Yeo et al74 aimed to validate a portable metabolic testing system (VO2000) on healthy sedentary pregnant individuals. The VO2000 consistently overestimated VO2 measurements, compared with the same manufacturer’s reference system, by 4.4±3.6 SD mL/kg/min although the Pearson correlation was significant (r=0.48; p=0.01). When the VO2000 was used twice, the mean difference was statistically significant (1.0±1.8 mL/kg/min; t(45)=3.9, p<0.001). Mottola et al75 provided a prediction equation for VO2peak in pregnant individuals between 16 and 22 weeks of gestation, using a modified Balke protocol. The results of this equation revealed an adjusted R2 of 0.71 and differences between actual and predicted VO2 of 2.7 mL/kg/min. When the authors used this equation to predict VO2peak in a cross-validation group (n=39), they found a predicted value of 23.38±4.03 mL/kg/min, while the actual value was 23.54±5.9 mL/kg/min (p=0.78).
A total of six articles analysed the association of CRF with maternal and neonatal health outcomes. Pomerance et al57 observed that VO2max was inversely associated with the length of labour in multiparas (r=−0.65; p=0.001) and prepregnancy weight (r=−0.63; p=0.001). However, VO2max was not correlated with newborn weight, length or head circumference, or with the 1 min Apgar scores (all p>0.05). In the same line, Wong and McKenzie108 observed that fit mothers showed lower HR at submaximal exercise intensity (p<0.05) and the second stage of labour was shorter (no statistics reported) compared with unfit pregnant mothers. However, there was no difference between fit and unfit in the length of gestation or weight gained (no statistics reported). In the same article, the authors showed neither positive nor negative effects of maternal fitness on newborn weight or Apgar scores.
In addition, Erkkola and Rauramo68 found that newborns from fit pregnant individuals had higher pH than fetuses of less physically fit women (p<0.01). In this article, participants with low physical performance were more likely to have asphyxiated neonates than neonates of physically fit women (p<0.05). In the same line, Baena-García et al13 observed that maternal CRF at the 16th gestational week was related to higher arterial umbilical cord PO2 (r=0.267, p<0.05), and those who had caesarean sections had significantly lower CRF compared with those who had vaginal births (p<0.001).
Moreover, Bisson et al8 studied the association of CRF in early pregnancy with physical activity before and during early pregnancy. The authors found that a higher VO2 peak in early pregnancy was positively associated with physical activity spent at sports and exercise before and during early pregnancy (p<0.001).
Muscular fitness
Only two muscular fitness tests assessed reliability.117 121 Yenişehir et al117 analysed reliability and validity of Five Times Sit-to-Stand. Inter-rater reliability was excellent for subjects with and without pelvic girdle pain (PGP) (intraclass correlation coefficient, ICC=0.999, 95% CI 0.999 to 1.000: ICC=0.999, 95% CI 0.999 to 0.999, respectively). Test–retest reliability was also very high for subjects with and without PGP (ICC=0.986, 95% CI 0.959 to 0.995: ICC=0.828, 95% CI 0.632 to 0.920, respectively).
Gutke et al121 analysed the reliability for an ad hoc test. This test consisted of a maximal voluntary isometric hip extension with a fixed sensor holding a sling around the thigh and pulling for 5 s during 3 reps with 5–10 s of rest (r=0.82 for the right leg and r=0.88 for the left leg; ICC=0.87 for the right leg and 0.85 for the left leg; with p value not reported).
Bisson et al8 observed that hand-grip strength was positively associated with infant birth weight (r=0.34, p=0.0068) even after adjustment for confounders (r=0.27, p=0.0480). Żelaźniewicz and Pawłowski et al115 observed that hand-grip strength was associated with offspring birth weight when controlled for the newborn sex and gestational age at delivery (F(2.182)=3.15; p=0.04). Baena-García et al13 found greater hand-grip strength weakly associated with greater neonatal birth weight (r=0.191, p<0.05). Wickboldt et al111 found that hand-grip strength was moderately correlated with pain scores, where the mean hand-grip strength during contractions had the highest correlation coefficient (r=0.67; p<0.001) compared with peak hand-grip strength (r=0.56; p<0.001) and the area under the curve of hand-grip force (r=0.55; p<0.001).
Flexibility
Lindgren and Kristiansson126 designed an ad hoc machine to test passive abduction of the left fourth finger and its relationship with low-back pain during pregnancy and early postpartum. Abduction angle was measured at three different times throughout the pregnancy and once in the postnatal period. Reliability of the abduction angle was analysed by the intraindividual coefficient of variance. The coefficients of variance between the first and second measurement was 0.077, between the second and third 0.070 and between the third and fourth 0.071.
Only two flexibility tests evaluated associations with maternal and neonatal health outcomes. Lindgren and Kristiansson126 found that women with greater passive abduction angle of the left fourth finger was associated with the highest back pain incidence (OR 1.09; 95% CI 1.01 to 1.17; p=0.022) and the highest number of previous pregnancies (OR 3.24; 95% CI 1.57 to 6.68; p=0.002). Baena-Garcia et al13 found increased flexibility associated with a more alkaline arterial pH (r=0.220, p<0.05), higher arterial PO2 (r=0.237, p<0.05) and lower arterial PCO2 (r=−0.331, p<0.01) in the umbilical cord blood.
Balance
No validity or reliability assessments were performed regarding balance tests.
Three articles associated balance with neonatal and maternal health-related outcomes. Öztürk et al128 observed that static balance decreased and fall risk increased in pregnant individuals with lower back pain (49.90±24.47 vs 28.47±19.60; p<0.0001). In relation to exercise, McCrory et al157 showed that exercise may play a role in fall prevention in pregnancy (p=0.005) and they also found that dynamic balance is altered in pregnant individuals who have fallen compared with non-fallers and non-pregnant individuals (p<0.001). Nagai et al158 studied the relationship between anxiety and balance. They concluded that when anxiety increases during pregnancy, the standing posture is destabilised (r=0.559, p=0.020), which may increase the chance of falling.
Speed
Validity and reliability for 10mTWT was studied by Evensen et al in two different articles.168 169 In 2015, Evensen et al168 analysed the test–retest reliability of 10mTWT showing an ICC of (0.74). Intertester reliability was determined in the first 13 participants with strong correlation (ICC=0.94). In 2016,169 the same authors analysed the convergent validity of 10mTWT by comparing performances with scores achieved on the Active Straight Leg Raise (ASLR) test and observed moderate positive correlations between 10mTWT and ASLR (r=0.65, p=0.003).
This systematic review did not find any articles that analysed the association of speed with maternal and neonatal health outcomes.
Agility and coordination
No articles were identified.
Multidimensional
Validity and reliability for TUG was analysed by Evensen et al in two different studies.168 169 The TUG showed good test–retest reliability (ICC=0.88) and intertester reliability (ICC=0.95). Regarding reliability, strong correlations were found between the TUG and ASLR (r=0.73, p=0.001).
The time on TUG among pregnant individuals with PGP was significantly higher (mean (95% CI) 6.9 (6.5 to 7.3) seconds) than for asymptomatic pregnant (5.8 (5.5 to 6.0), p<0.001) and non-pregnant (5.5 (5.4 to 5.6), p<0.001) individuals.
Discussion
Summary of the evidence
This systematic review revealed that PF has been assessed through a wide variety of tests during pregnancy. However, little is known on the validity and reliability of the tests performed, and the large variety of tests makes it challenging to compare results from different studies. Until a battery of specific fitness tests for pregnant women is developed and validated, the confidence of PF data obtained during pregnancy is limited and should be interpreted with caution. Consequently, the appropriateness of using this PF data to prescribe exercise during pregnancy could be questioned and is a matter that requires special attention. In this context, it is also difficult to evaluate the association of PF with maternal and neonatal health which, in fact, is of wide clinical and public health interest. However, some studies observed associations of PF with maternal and neonatal health outcomes, which needs to be replicated once a PF test battery is released. We strongly suggest that extensive research must be performed to validate such battery of PF tests.
Cardiorespiratory fitness
This systematic review identified that a cycle ergometer has been the equipment most frequently used to assess CRF followed by treadmill and field tests, although step tests have also been conducted. There is a large disparity of protocols and wide variety of ad hoc tests used, which makes comparing results between studies difficult. However, the Modified Balke treadmill Protocol validated by Mottola et al75 for pregnant women has been the most frequently used test. There have been more incremental tests used for CRF tests during the pregnancy compared with steady-state tests and more submaximal compared with maximal tests. There is no consensus regarding test termination criteria for submaximal tests, which undoubtedly needs further research. Some articles used relative intensity using physiological variables such as %HRmax or %VO2max, and others used absolute intensity, such as specific HR (beats per minute). Among the studies that used %HRmax as a test termination criterion, there was a variety of percentages such as 70%,34 35 90 100 75%27 29 69 97 or 85%.13 54 74 Among the studies that used %VO2max, there were different percentages such as 40%,38 50%,37 101 60%32 38 or 70%.30 Among the studies that used absolute HR as a test termination criterion, the HR for finalising the tests were set either at 125,61 150,36 45 62 108 155,94 16065 or 17050 53 55 56 beats per minute. Some studies even used the rate of perceived exertion as complementary criteria46 50 106 or peak aerobic power.39 These complementary criteria have been recommended and studied in pregnant women by authors like Hesse et al98 since the physical and emotional changes during pregnancy limit performance. It must be noted that the same equation was not used to estimate HRmax. Some articles used the traditional 220-age formula29 35 54 69 97 while others used the Karvonen74 or Tanaka100 formulas. Some articles did not specify how HRmax was estimated.27 34 90 This heterogeneity could be due to the physiological complexity of pregnancy, in terms of cardiac changes and response to exercise and the lack of scientific information in this regard. Moreover, the gestational week could be a determinant for physiological responses since Bijl et al100 observed a slower haemodynamic recovery and an increased ventilatory response to exercise in early pregnancy compared with non-pregnant women. With regard to maximal tests, different terms have been used for maximal criteria such as volitional fatigue,30 33 43 44 47 48 98 103 105 exhaustion,31 anaerobic threshold73 80 104 171 and point of symptom limitation.59 60 102
This lack of consensus has many drawbacks that should be resolved in view of the need to accurately assess CRF during the pregnancy. We advocate for an expert consensus to be developed in the following years to achieve the goal of appropriate and effective CRF assessment during the pregnancy. In particular, it seems essential to develop a treadmill and a cycle ergometer submaximal test that reveals sufficient validity to confidently estimate VO2max throughout gestation.
Muscular fitness
Muscular fitness tests included muscular strength, endurance and power.2 The studies included in this systematic review show that muscular strength was the most frequently assessed component of muscular fitness, since only six studies12 13 112 117 122 178 179 assessed endurance and none of them assessed power in pregnancy. In most studies, muscular strength was evaluated through hand-grip maximal strength using a dynamometer. However, two studies used a hand-grip sphygmomanometer test.118 119 Some of the hand-grip tests were performed in a standing position,8 109 while others used a sitting position110 or supine position,113 and others did not reveal the position used for the assessment.86 112 114 115 Some tests were completed three times,112 others twice8 86 115 and others only once.110 113 114 This clearly reveals a large methodological variability that might influence the results and make comparing results between studies difficult. Another limitation is the fact that the main strength outcome was hand-grip strength. While hand-grip strength is a good marker of health,180 it is unclear whether hand-grip responds to changes following exercise interventions. Therefore, validating other muscular strength tests, including lower limb strength tests, is needed for researchers and practitioners to confidently assess muscular strength during the pregnancy.
There were no validity studies and the reliability was assessed only in one maximal isometric hip extension test.121 This test has limitations since the pregnant abdomen must be on a bed and, as acknowledged by the authors, it cannot be performed during the third trimester. It must be noted that higher hand-grip strength was associated with higher birth weight.8 115 Moreover, increased hand-grip strength was produced during uterine contraction.111 The advantage of using hand-grip is that it represents an inexpensive, rapid and easy-to-use assessment with minimal training needed to appropriately administer. However, assessing the performance of pregnant athletes with this test seems clearly insufficient. More quality in tests employed is necessary since the association of muscular strength with maternal and neonatal health outcomes is of clinical importance. Moreover, other studies are needed to understand the extent to which preserving strength throughout pregnancy and post partum relates to clinical outcomes.
Flexibility
Although there were seven studies assessing flexibility, none of them used the same protocol. Once again, this reflects a lack of agreement when assessing the same component of PF. Moreover, Lindgren and Kristiansson126 found that higher flexibility showed higher low back pain. Despite the limitation of a finger laxity test, we considered these findings an interesting association that warrants further investigation since passive stretching is one of the most common practical prescriptions for exercise professionals instead of mobility and breathing exercises. On the other hand, the results of Baena-García et al13 are very relevant to fetal health since flexibility was associated with a better pH, PO2 and PCO2 in umbilical cord blood. Hence, more research about flexibility tests, their outcomes and their prescription are needed.
Balance
We identified that balance was the second PF component most frequently evaluated during pregnancy, following CRF. This makes sense since the centre of gravity changes during pregnancy as a result of expansion of the uterus and the risk of falls increases. However, there is high heterogeneity between the protocols employed in different studies. For static balance, the protocol most frequently used was stabilometry on a force platform with bipedal support and eyes open and eyes closed within the same test. For dynamic balance, there was a greater heterogeneity across protocols both in the platform used and in the movements over the platforms. Regarding the assessment tool, the 3-D camera was the device most frequently used.139–142 144 165 Likewise, we observed differences between the number of platform pieces, trials and Hz used. Some protocols were performed on two piece platforms,130 131 149 others on one piece platforms129 132 138 158 160 166 167 and others did not specify the type of platform.163–165 Although the number of trials and the frequency of recording (ie, Hz) are important protocol parameters that should be carefully documented, only 5 (out of 13) articles described the number of trials131 138 166 167 175 and 1 described frequency of recording.149 The usefulness of these tests is restricted to the research area and all of them use expensive technological tools; therefore, it is difficult to extrapolate these tests to fitness centres or clinical settings. Falls during pregnancy could be prevented if balance was easily assessed. For this reason, it is necessary to develop an inexpensive and easy-to-use balance field test.
Validity and reliability of PF tests, and association with maternal and neonatal health
Unfortunately, studies that examine validity and reliability of PF tests are scarce. The PF component most frequently studied was CRF. However, we only found two studies that analysed the validity of the CRF tests, and no studies examined the reliability of these tests. On a treadmill platform, Mottola et al,75 validated a special equation for modified Balke protocol that has been used by numerous other authors. In contrast, Yeo et al74 aimed to validate a portable metabolic testing system (mod. VO2000) but it overestimated VO2 measurements for pregnant individuals compared with non-pregnant females and males.
Regarding muscular fitness, the hand-grip test was most commonly used; this test was used as the gold standard for muscular fitness during pregnancy. Only Gutke et al121 studied the reliability of a test for hip extension. However, the p value was not reported, and the position adopted in the test could be uncomfortable for pregnant participants. Finally, the studies evaluating validity and reliability of speed and multidimensional tests of PF have been researched by Evensen et al.168 169 They demonstrated that TUG and 10mTWT are reliable and valid tests for use during the pregnancy.
The validity and reliability of balance (without tests), agility and/or coordination tests has not been investigated to date.
We suggest that specific tests to be performed in pregnancy are needed and their validity and reliability must be assessed to understand the extent to which one might rely on such measures when prescribing exercise, or making clinical recommendations.
Regarding the association of PF with maternal and neonatal health outcomes, we conclude that more research is also necessary. Nevertheless, from this review we can highlight some interesting associations with different fitness components. A better CRF was associated with a shorter labour57 108 and a lower risk of caesarean section.13 However, no association was found regarding other fetal outcomes such as Apgar scores or the newborn anthropometrics.57 108 By contrast, muscular strength was associated with optimum infant birth weight.8 13 115 Other neonatal outcomes like fetal umbilical cord pH were positively associated with maternal CRF.68 On the other hand, better balance scores were associated with lower risk of falls,128 158 181 which is of particular interest for exercise professionals, who might include balance as a component of exercise programs for pregnant women. Finally, Evensen et al169 found that PGP could be a limiting factor to assess PF in pregnant individuals since the time of TUG was significantly higher in those with pain than in asymptomatic pregnant and non-pregnant individuals.
None of the studies reviewed in this article have described adverse events during PF assessment. Moreover, official bodies such as the American College of Obstetricians and Gynecologists, the Canadian Society of Exercise Physiology and the Society of Obstetricians and Gynaecologists of Canada have highlighted the benefits of an adequate PF assessment, and assert the need of consensus in PF assessment during the pregnancy.182 Consequently, the findings from this study have important research and clinical implications.
Limitations and strengths
A limitation of this article is that, although PubMed and WOS are among the most relevant databases in the medical literature, the possibility that a small number of studies have been overlooked cannot be discarded. Nevertheless, these two databases are the biggest databases in sports medicine and sports sciences and, therefore, include the vast majority of studies.
A strength of this systematic review is the fact that, to the best of our knowledge, this is the first article to comprehensively analyse PF assessments, the validity and reliability of fitness tests, and their relationship with maternal and neonatal health outcomes during the pregnancy. The results from this systematic review provide an overall picture of how PF is being assessed in this population, what type of tests are being performed, their specific characteristics, whether these tests have been tested for validity and/or reliability; and whether PF is associated with maternal and neonatal health outcomes. All this information is of wide and undoubted clinical interest.
Conclusions
The main finding of this systematic review is that PF has been assessed through a wide variety of protocols, mostly lacking validity and reliability data, and that no consensus exists on the most suitable fitness tests to be performed during pregnancy. In addition, the available evidence regarding the association of PF with maternal and neonatal health outcomes is scarce and is a matter of further investigation. Provided the need to assess PF during the pregnancy and the importance not only to understand the physical state of the pregnant individual but also to precisely prescribe exercise in this population, extensive research is needed to design and validate a battery of fitness tests to be used for the safe and effective assessment of PF during pregnancy. We advocate for an expert consensus panel to develop a battery of PF tests to assess the different PF components during pregnancy.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @lidiaromero_owa, @AlbertoSoriano_
ORR and JC-P contributed equally.
Contributors Conceptualisation: LR-G, VAA, JC-P and AS-M. Literature search and data analysis: LR-G and ORR. Methodology: LR-G, ORR, JC-P, MM, VAA and AS-M. Formal analysis and investigation: LR-G, ORR and AS-M. Writing-original draft preparation: LR-G. Writing-review and editing: LR-G, ORR, JC-P, LEM, OO, LM, MM, VAA and AS-M. Resources: VAA, JC-P and AS-M. Supervision: VAA, OO, JC-P and AS-M.
Funding This study has been partially funded by the University of Granada, Plan Propio de Investigación 2016, Excellence actions: Units of Excellence: Unit of Excellence on Exercise and Health (UCEES), and by the Junta de Andalucía, Consejería de Conocimiento, Investigación y Universidades and European Regional Development Fund (ERDF), ref. SOMM17/6107/UGR. This study is included in the thesis of LRG enrolled in the Doctoral Program in Biomedicine of the University of Granada.
Competing interests Yes.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note Please note that this work was posted as a pre-print prior to submission. The pre-print version can be accessed here https://doi.org/10.1101/2021.06.26.21259584.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.