Article Text

Abstract
Purpose Evaluate patient-reported knee function after arthroscopic partial meniscectomy (APM) and meniscus suture repair in two different age cohorts compared with a normal population.
Method Arthroscopic meniscus surgery was performed on 421 patients at Skåne University Hospital from 2010 to 2014, with a mean (SD) follow-up of 4.2 (1.4) years. Patients and controls were divided into two age cohorts; 18–34 years (younger) and 35–54 years (middle-aged) as well as according to surgery performed; either solely meniscus surgery or with concurrent anterior cruciate ligament reconstruction (ACLR). The outcome is measured with the five subscales of the Knee and Osteoarthritis Outcome Score (KOOS).
Results No significant difference in outcome after all studied types of meniscus surgeries between younger-aged and middle-aged patients.
Younger patients with APM or meniscus suture repair, with or without, ACLR score lower than the normal population in all subscales of KOOS (p<0.001), except in Activities of Daily Living (ADL) for meniscus suture patients.
Middle-aged patients with APM score lower in all subscales than the normal population (p≤0.009). Those with meniscus suture repair score lower than the normal population only for the subscales Sport/Rec and quality of life (p<0.001).
Both younger-aged and middle-aged patients achieve better KOOS values after meniscus suture repair and ACLR than after all other combinations of surgery.
Conclusion Patients with meniscus injuries do not reach the same KOOS score as the normal population, irrespective of age or type of meniscus surgery performed. However, combined with ACLR in younger-aged and middle-aged patients, meniscus suture gives a better subjective outcome than isolated meniscus surgery.
- Knee injuries
- Arthroscopy
- Knee surgery
Data availability statement
Data are available on reasonable request. Data files exist but include personal identification number of all participants, which is why it is not made public.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Arthroscopic partial meniscectomy for most degenerative meniscus tears is no better than physical therapy.
There is a lack of good level 1 studies for the surgical treatment of traumatic meniscus injuries.
WHAT THIS STUDY ADDS
No significant difference in Knee and Osteoarthritis Outcome Score after meniscus surgery between younger-aged and middle-aged patients.
Worse reported knee function, compared with a normal population after arthroscopic meniscus surgery regardless of age and type of surgery with or without anterior cruciate ligament reconstruction.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Inform patients before surgery that their knee will not be fully restored and thereby set realistic expectations before surgery.
Introduction
An arthroscopic partial meniscectomy (APM) for both traumatic and degenerative meniscus tears is the most common type of knee surgery.1 2 Degenerative tears are more common in a middle-aged population, >40 years old, with or without a traumatic event. Englund et al3 demonstrated that degenerative meniscus tears are commonly found in patients >50 years of age, and the incidence increases with age. Younger patients, <40 years of age, on the other hand, mostly have traumatic tears due to a traumatic event and an acute onset of symptoms.4 Degenerative meniscus tears are commonly associated with osteoarthritis (OA), while traumatic tears are associated with anterior cruciate ligament (ACL) injury.5
An increasing number of studies, with several randomised clinical trials (RCTs) and meta-analyses, have been published. These report that APM for degenerative meniscus tears is no better than sham surgery or physical therapy.5–10 There is only one RCT, from 2022, that investigate the difference between physical therapy and surgery in younger patients, which suggests that early surgery is not superior to physical therapy.11
A few studies examine the subjective outcome based on the type of surgery performed, that is, APM or meniscus suture repair.12–15 However, these studies do not examine the outcome compared with a normal population. To our knowledge, no study investigates the patient-reported outcome (PRO) after meniscus surgery compared with a normal population.
The current study aimed to compare the subjective knee function in a large cohort of patients, divided into two different age cohorts, having had either APM or meniscus suture repair, with each other and a corresponding normal population. This knowledge can be used in the clinical setting to provide correct information to patients before surgery and set realistic expectations for the surgery.
Our main hypothesis was that younger patients, who mainly suffer from traumatic lesions, will, after meniscus surgery, have a subjective knee function that is more on par with the normal population and better than middle-aged patients.
Material and methods
Register resources
This is a retrospective cohort study performed using prospectively ascertained healthcare data from the southernmost region in Sweden, Skåne (population 1.3 million). Electronic surgical journals (OrtReg), where all surgeries in Skåne are registered, were used. The data entries in OrtReg include information on the date of surgery, healthcare provider, diagnostic codes according to the International Classification of Diseases (ICD) 10 system and codes for surgical procedures according to the Nordic Medico-Statistical Committee classification. Data were collected on the type of meniscus surgery (APM or meniscus suture repair). In the case of concurrent meniscus suture repair and APM, the surgery was considered a meniscus suture repair.
Inclusion criteria
The following inclusion criteria were used; (1) ICD-10 codes: NGD11 (partial meniscectomy) and/or NGD21 (meniscus suture repair). For the meniscus repair, the second generation of all-inside technique was used (Fast-Fix, or in a minority of cases, inside-out placed Maxon or outside-in placed PDS suture). For ACL reconstruction (ACLR) hamstring tendon was used in the majority of cases; (2) Place of surgery: Skåne University Hospital; (3) Year of surgery: 2010–2014. Patients below 18 years of age and older than 54 were excluded.
Study population
A total number of 1434 patients aged 18–54 were asked to participate. The request to participate in the study was sent out 2–7 years after surgery.
Patients were divided into two age cohorts; 18–34 years (younger) and 35–54 years (middle-aged). We further compared the two age cohorts’ outcomes in four different groups based on the surgery performed; APM or meniscus suture repair with and without concurrent ACLR.
All patients had undergone physical therapy before surgery, except those with acute traumatic bucket-handle tears with a locked knee. After surgery, regardless of type, all patients were referred to a physiotherapist for rehabilitation.
Non-responders
Approximately one-third of the eligible participants answered the survey. The overall mean age of participants was higher than for non-responders, 39 and 33 years, respectively. Among non-responders, 77% underwent APM, and 23% had their meniscus repaired. The percentage of the participants were similar; 73% APM and 27% meniscus suture repair.
Data capture methods
A letter containing informed consent and an explanation of the study was sent to all eligible patients. The signed informed consent and email addresses of the participants were collected. Using the tool REDCap (Research Electronic Data Capture, V.6.10.11), hosted at Lund University, participants were invited to take the web-based survey. Two reminders were sent, by email, to those who did not answer the survey. REDCap is a secure, web-based application for data capture in research studies, providing intuitive data entry, audit trails for tracking data, automated export procedures and importing data from external sources.16 The survey included two different assessment instruments listed below.
PRO measures
The outcome was the five subscales of the Knee and Osteoarthritis Outcome Score (KOOS). KOOS is a self-administered questionnaire that covers five patient-relevant subscales. A score of 100 indicates no knee symptoms, and a score of 0 indicates extreme symptoms.17 18 It is validated for patients with developing OA and ACL and meniscus injury.19 ACL injured knees often have meniscus tears suitable for meniscus suture repair. ACL injury and surgery have a major impact on KOOS, especially in the quality of life (QOL) subscale.20 21
The division into the cohorts is based on the higher probability of having a traumatic meniscus injury versus a degenerative in the younger versus the middle-aged. This coincides with the age intervals in the normal population we compare to.22 A meniscus lesion in patients >35 years of age, without significant trauma, should initially be treated as a degenerative tear.23 KOOS also changes with age, and one can see a decrease in the scores of sport and recreation with increasing age.22
Participants used the Tegner Activity Score (Tegner) to grade their activity level from 0 to 10 (a high score indicates a higher activity level).24
Symptomatic knee
According to Englund et al,25 a symptomatic knee was defined based on the patient’s self-reporting from the KOOS questionnaire. They defined a knee as symptomatic if the score of the KOOS subscale QOL and two other subscales, out of four, were lower than a calculated cut-off value. This operational definition aims to identify individuals symptomatic enough to seek medical care. Another way to define a symptomatic knee is by using a patient’s acceptable symptom state (PASS). PASS thresholds are specific to the patient cohort, and different cohorts will have different PASS values. The PASS value used was by Pedersen et al,26 and the percentage of patients above the PASS value was calculated.
Normal population
We used data from Paradowski et al for the corresponding normal population from the same region.22 From their article, we used the mean KOOS score for men and women, respectively, in age groups 18–34 and 35–54. Since the difference between men and women are less than 10 points in KOOS (which is defined as clinically significant27), we choose not to analyse them separately.
Statistical analysis
IBM SPSS Statistics, V.24, was used for the statistical analysis. The Mann-Whitney U test was used to compare the two different age cohorts. The KOOS population data for men and women were pooled as one group and compared with the calculated values for KOOS of the study population with the help of the one-sample z-test. A p<0.05 was set as statistically significant. A 95% CI was calculated for the difference in mean value between population data and study data.
Patient and public involvement
Patients and the public were not involved in the study design, data analysis, writing and editing. Still, all participants were asked to fill in an informed consent before being included in the study.
Results
Study population
A total of 421 patients answered the survey. Figure 1 illustrates a flow chart detailing the number of participants in the study, as well as the number of surgeries performed. The mean follow-up time range between 3.7 and 5.0 years for the different groups with a mean (SD) of 4.2 years (1.4). Body mass index (BMI) for younger-aged and middle-aged patients was similar. A total of 62 patients (mean age 40.4) had a known instability in their knee and/or a distortion/rupture to the cruciate ligaments and/or collateral ligaments treated non-surgically.
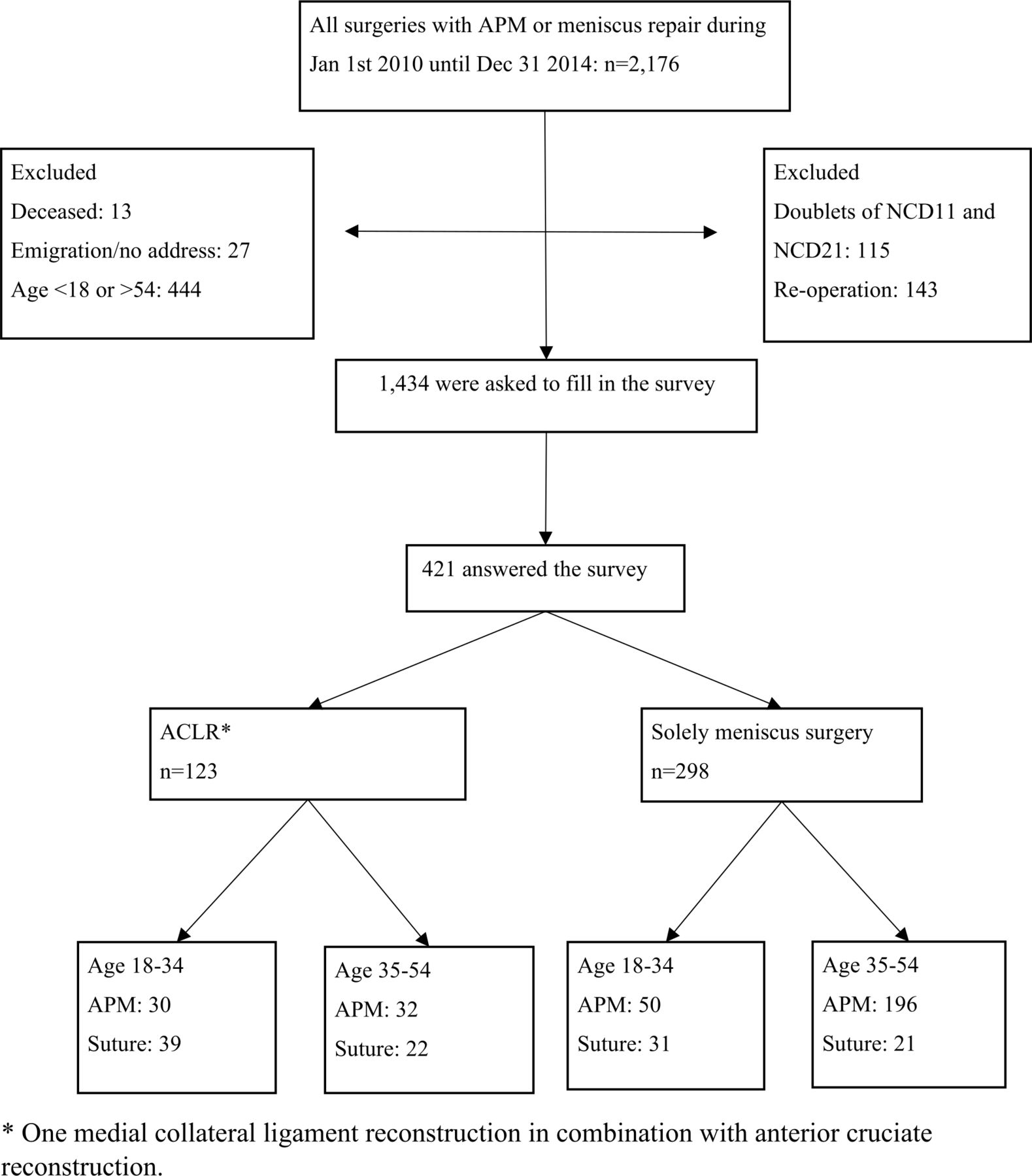
Flow chart detailing the study cohort. Detailing the inclusion process and the number of excluded patients. ACLR, anterior cruciate ligament reconstruction; APM, arthroscopic partial meniscectomy; NCD11, partial meniscectomy; NCD21, meniscus suture repair.
All group characteristics are displayed in table 1, as well as the percentage of patients with a score over their PASS as defined by Pedersen et al.26
Group characteristics for the subgroups
Younger-aged versus middle-aged patients
There is no significant difference in any of the subscales of KOOS between the two age cohorts, regardless of the type of surgery (see figures 2 and 3 and online supplemental appendix 1).
Supplemental material
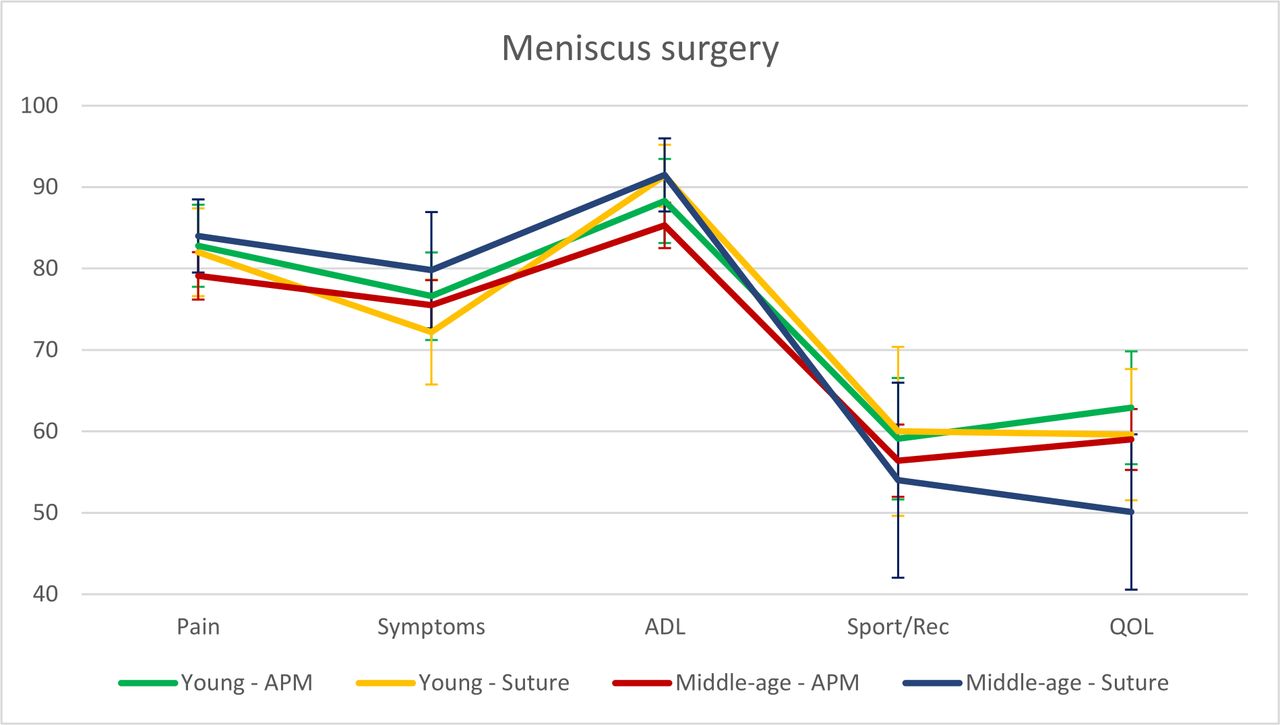
KOOS profile for solely meniscus surgery in the two age cohorts. KOOS profile for participants that underwent meniscus surgery solely, with mean value and 95% CI of the mean value of each subscale, set as error bars. ADL, activities of daily living; APM, arthroscopic partial meniscectomy; KOOS, Knee and Osteoarthritis Outcome Score; QOL, quality of life.

KOOS profile for meniscus surgery with ACLR in the two age cohorts. KOOS profile for participants that underwent meniscus surgery with concurrent ACLR, with mean value and 95% CI of the mean value of each subscale, set as error bars. ACLR, anterior cruciate ligament reconstruction; ADL, activities of daily living; APM, arthroscopic partial meniscectomy; KOOS, Knee and Osteoarthritis Outcome Score; QOL, quality of life.
Younger patients
Younger patients operated with APM scored significantly lower in all subscales of KOOS in comparison to the normal population. Meniscus suture repair also resulted in lower scores in all subscales of KOOS, except Activities of Daily Living (ADL). A clinically relevant difference for both APM and meniscus suture repair could be seen in the subscales Sport/Rec and QOL (see figure 4 and online supplemental appendix 2).

KOOS profile for younger patients. KOOS profile for participants aged 18–34 years old with mean value and 95% CI of the mean value of each subscale, set as error bars. *Population data calculated from Paradowski et al. Klicka eller tryck här för att ange text.22 ACLR, anterior cruciate ligament reconstruction; ADL, activities of daily living; APM, arthroscopic partial meniscectomy; KOOS, Knee and Osteoarthritis Outcome Score; QOL, quality of life.
Middle-aged patients
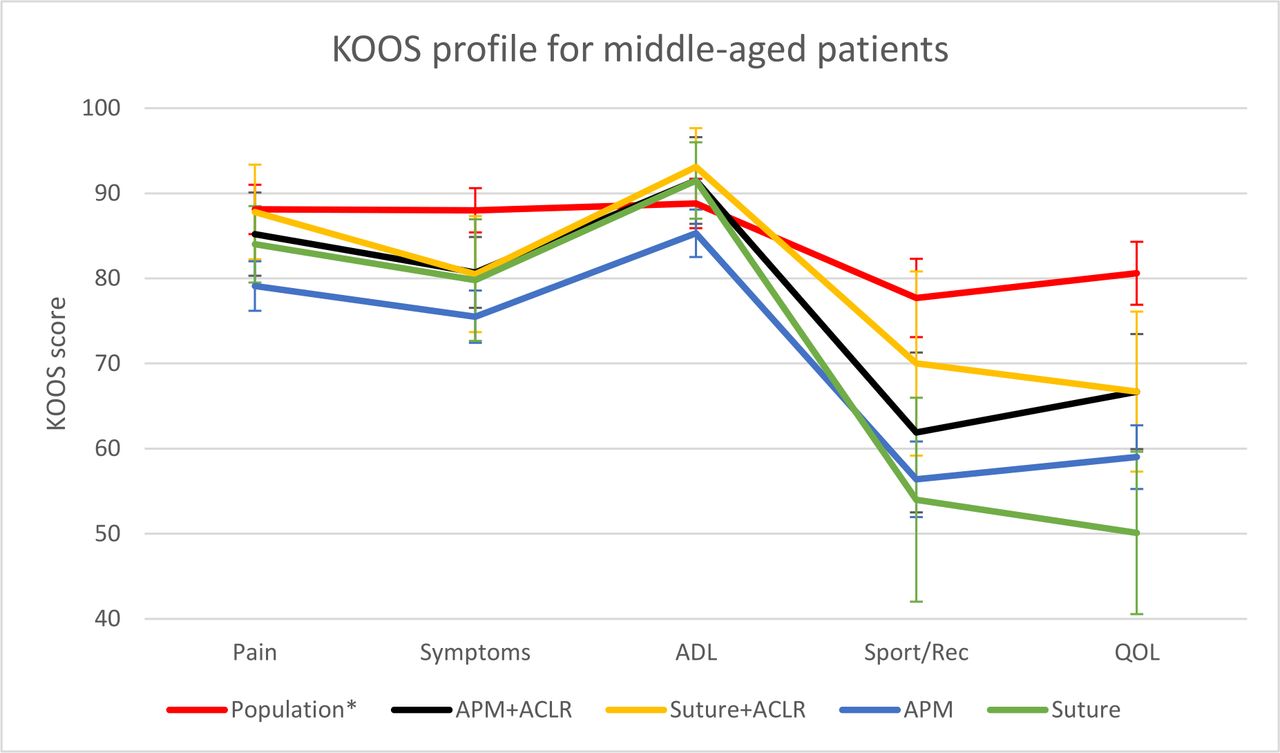
Middle-aged patients with APM score lower in all subscales of KOOS than the corresponding normal population. The difference is clinically relevant in the subscales Sport/Rec and QOL (see figure 5 and online supplemental appendix 3). Meniscus suture repair in middle-aged patients has a lower score compared with a normal population only in the subscales Sport/Rec and QOL, which also show a clinically relevant difference (figure 5 and online supplemental appendix 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
KOOS profile for middle-aged patients. KOOS profile for participants aged 35–54 years old with mean value and 95% CI of the mean of each subscale, set as error bars. *Population data calculated from Paradowski et al. Klicka eller tryck här för att ange text.22 ACLR, anterior cruciate ligament reconstruction; ADL, activities of daily living; APM, arthroscopic partial meniscectomy; KOOS, Knee and Osteoarthritis Outcome Score; QOL, quality of life;.
Concurrent ACLR
Briefly, middle-aged patients had KOOS values closer to the normal population than younger patients. Both younger-aged and middle-aged patients with the combination of ACLR and meniscus suture have better KOOS scores than other combinations of surgery (figures 4 and 5 and online supplemental appendices 2 and 3).
Discussion
The most important finding of our study is that patients cannot expect to regain full knee function after meniscus surgery at a mid-term follow-up (mean range 3.7–5.0 years), regardless of age and surgical procedure. Meniscus lesions, treated according to meniscus saving strategies based on the surgeons’ decision and individual tear pattern with APM or suture repair, resulted in similar KOOS scores in both younger-aged and middle-aged patients. None of the groups reached the KOOS scores of the normal population. However, middle-aged patients had KOOS values closer to the normal population than younger patients. This challenges the common belief that younger patients with more traumatic lesions benefit more from meniscus surgery than middle-aged patients. In addition, we found that patients operated with concomitant meniscus suture repair and ACLR, especially in middle-aged patients, had KOOS values closer to the normal population.
To our knowledge, this is the first study that compares knee function in patients after meniscus surgery with a normal population. Thorlund et al,15 in their discussion, reflect on the scores of KOOS for traumatic tears and degenerative tears as compared with the same normal population from Sweden in our study. Their findings indicate lower scores overall, especially lower in Sport/Rec and QOL. Contrary to their hypothesis that traumatic tears have a better outcome, no such difference was shown. Instead, a statistically significant improvement in PROMs from the pre-operative baseline was seen after APM for degenerative tears.15 Pihl et al28 showed that as many as 50% of both young and old patients were dissatisfied with their knee function 3 months after surgery.
Ericsson et al29 mentioned as early as 2006 that patients after APM score worse in all five subscales in KOOS compared with a knee-healthy population. Similar findings are confirmed in our study. KOOS ADL, however, is not a sensitive subscale for our patient category, especially in younger patients, since many have a high level of function and thereby not many problems in ADL. It might be that KOOS4 is a better outcome than using all subscales separately since KOOS ADL is excluded.
When looking at the percentage of a symptomatic knee, according to the definition by Englund et al,25 53.8%–66.7% in our study had a symptomatic knee. According to PASS values from Pedersen et al,26 38.1%–90.9% of our patients cleared the cut-off for acceptable symptoms. However, this value for PASS was only 3 months after surgery, and data has shown that patients improve even after 3 months postoperatively.14 Therefore, the PASS value will probably be higher.
Older patients overestimate their recovery speed after knee surgery and have lower demands on their knee function than younger individuals.28 Younger patients also have higher expectations about return to recreational sport.28 Since satisfaction after surgery is closely linked to expectations of the surgery, this could partly explain why our main hypothesis is rejected.
A study from 202130 showed that patients younger than 40 years with meniscus sutures had less improvement in KOOS score than APM after 12 months and 5 years follow-up. This is contrary to our results, where we see a trend to better KOOS scores after meniscus suture, especially in combination with ACLR. An explanation could be that they did not include patients with concurrent cruciate ligament reconstruction. Furthermore, nothing is mentioned about the inclusion or treatment of patients with knee instability due to ligamentous injury, which was not treated with cruciate ligament reconstruction.30 ACLR has a suggestive protective role for a subsequent meniscus injury. Nonetheless, the risk for meniscus injury is still higher for the contralateral knee.31 Also, the success rate of meniscus repair is higher with concomitant ACLR.21
Even though our study and the studies mentioned above show that PROM is lower for patients with a meniscus injury, there is a lack of studies with a high level of evidence regarding the treatment for traumatic tears. There are heterogeneous results from the mentioned studies regarding the outcome after meniscus surgery. A recent meta-analysis32 compared different surgical treatments for meniscus injuries, regardless of cause. The consensus was that there is a lack of good level 1 studies for the surgical treatment of traumatic meniscus injuries. A new RCT has compared the effects of surgical treatment versus physical therapy for traumatic tears and it suggests that early meniscus surgery is not superior to physical therapy.11 From our study, we can see that younger patients, presumed to have traumatic tears, score lower than a normal population and have similar KOOS results as middle-aged patients after surgery.
Strengths and weaknesses
A major weakness of our study is the selection bias since only about one-third of the eligible patients answered the survey, and those that answered had a higher mean age than the non-responders. However, we did perform a small drop-out analysis, and the two groups had similar characteristics regarding surgery performed. This study might have a higher degree of degenerative tears and subsequently more cases of APM, as opposed to younger patients with traumatic tears with a higher chance of meniscus suture repair. Notably, this is a convenience cohort and the division into traumatic or degenerative tears is solely based on age which is a major weakness since both younger-aged and middle-aged patients could have degenerative and traumatic tears irrespective of age. Similarly, the meniscus tears are not classified, which is a shortcoming of the study and makes it impossible to do any sensitivity analysis of the data. Furthermore, middle-aged patients with ACLR and meniscus sutures probably have a combination of both traumatic and degenerative tears, but all tears suitable for suture were sutured.
Another major bias is the confounding-by-indication. The patients are selected for treatment according to injury and patient characteristics. This bias is probably greatest in middle-aged patients with ACLR and meniscus sutures since they have a higher demand for a stable knee compared with others of the same age and might also have a relatively better physique. These patients are probably more motivated to go back to recreational sports. Almost all our patients underwent physical therapy before and after the surgery, but no data are gathered on how they adhered to their rehabilitation. Rehabilitation plays a big role in outcome after surgery, which must be considered when interpreting the results. Younger patients had similar BMI as middle-aged but higher scores on Tegner, which could explain the low scores in QOL and Sport/Rec after surgery since younger patients aim for a more demanding activity level. However, the Tegner score is after surgery, and we do not know the activity level before surgery.
It is unknown whether the individuals that did not answer the survey were more satisfied or not with their knee function. Individuals with chronic pain have a higher tendency to answer surveys.33 It is not likely that our main conclusions from this study would have been substantially different since we have collected data from many patients (n=421), although some groups have a low number of patients.
Since this is a retrospective cohort study, no data exist on KOOS before surgery. Furthermore, this is not a multicentre study: the participants in the study come from only one hospital, and thus the results cannot be extrapolated.
A strength of the study is that the results are relevant since patients were operated on according to meniscus saving guidelines, with high numbers of meniscus repairs performed when possible.23 34 Also, PROMs were measured using a validated PROM for knee and meniscus injury, KOOS.
The results of this study could be used to inform patients about the surgery’s outcome and stress that there is a risk that they will not be fully restored after surgery. This regardless of age, concurrent injuries, traumatic lesions or not and meniscus resection or suture.
Conclusion
Patients with meniscus injuries do not reach the same KOOS score as the normal population, irrespective of age or type of meniscus surgery performed. However, combined with ACLR in younger-aged and middle-aged patients, meniscus suture gives a better subjective outcome than isolated meniscus surgery.
Data availability statement
Data are available on reasonable request. Data files exist but include personal identification number of all participants, which is why it is not made public.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Regional Lund University Ethics Committee, study identification number: 2019-02850. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Abstract presented at the virtual ESSKA congress 2021.
Contributors SA collected and processed the data, performed the statistical analysis and drafted the manuscript. IK and PN participated in the design of the study and helped to draft the manuscript. PN is the guarantor. All authors read and approved the final manuscript.
Funding The Swedish Research Council, Kock Foundations, Governmental Funding of Clinical Research within National Health Service, ALF, and the Faculty of Medicine, Lund University, Sweden.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.