Article Text

Abstract
Our primary objective was to explore the barriers preventing clinicians from implementing what they think is ideal practice as it relates to using tools to aid diagnosis and monitor progress in mid-portion Achilles tendinopathy. Our secondary objectives were to describe the assessments employed by clinicians in their own practice to aid with (a) diagnosis and (b) monitoring progress in Achilles tendinopathy and explore the outcome measure domains clinicians believe to be the most and least important when managing patients with Achilles tendinopathy. We employed a qualitative descriptive study design. Thirteen participants (eight female, five male) from across Australia, consisting of two junior physiotherapists, five senior physiotherapists working in private practice, four senior physiotherapists working within elite sports organisations and two sport and exercise medicine doctors, were included and one-on-one interviews were performed. Audio was transcribed then entered into NVivo for coding and analysis. Four main themes were perceived as barriers to implementing ideal practice of assessment and monitoring in people with Achilles tendinopathy: financial constraints, time constraints, access to equipment and patient symptom severity. Assessments related to function, pain on loading, pain over a specified time frame and palpation are commonly used to assist diagnosis. Assessments related to disability, pain on loading, pain over a specified time frame and physical function capacity are used to monitor progress over time. Furthermore, pain on loading and pain over a specified time frame were considered the most important outcome measure domains for assisting diagnosis whereas pain on loading, patient rating of the condition and physical function capacity were the most important outcome measure domains for monitoring progress. A number of barriers exist that prevent clinicians from implementing what they view as ideal assessment and monitoring for Achilles tendinopathy. These barriers should be considered when developing new assessments and in clinical practice recommendations.
- tendon
- validity
- physiotherapist
- physician
- sports & exercise medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Clinicians perform a number of different assessments for tendinopathy, across a variety of different outcome measure domains.
However, research quantifying what is current assessment and monitoring as well as the barriers in clinical practice does not exist.
What are the new findings
Four main themes were perceived as barriers to implementing ideal practice of assessment and monitoring in people with Achilles tendinopathy: financial constraints, time constraints, access to equipment and patient symptom severity.
Pain on loading and pain over a specified time frame were considered the most important outcome measure domains for assisting diagnosis.
Pain on loading, patient rating of the condition and physical function capacity were considered the most important outcome measure domains for monitoring progress.
Introduction
Achilles tendinopathy is characterised by pain, stiffness and a loss of function in both athletic and sedentary populations1 2 with exercise rehabilitation recommended as best management for this condition.3–6 Various assessment tools exist for mid-portion Achilles tendinopathy and have been used for diagnosis, as study inclusion criteria and as outcome measures to monitor progress.5 7–11 Examples include a patient’s self-reported pain with functional tasks, validated patient-reported outcome measures or an objective assessment of functional capacity.12 13 However, not all tools have been validated,14 thus it is valuable to find out what is being used (and how) in clinical practice regarding the assessment and monitoring of Achilles tendinopathy.
There is little consistency between published studies in the assessments used to quantify demographic information, diagnose the condition or assess improvements in different systems (eg, tendon structure or muscle force production) relevant to rehabilitation.12 13 15 For instance, across exercise rehabilitation trials to treat mid-portion Achilles tendinopathy, we identified numerous assessment tools used to assess different aspects of pain and function,12 13 yet few reported data related to their reliability and validity.12 13 The lack of data on the identified assessment reliability is an issue as it undermines any analysis to determine if change has truly occurred16 and likely makes the diagnosis and monitoring of mid-portion Achilles tendinopathy even more challenging for clinicians, because if research studies are not using consistent assessments how can we expect that from clinicians?
In 2019, three international consensus statements (ICON 2019) were developed by expert clinicians and researchers with a special interest in tendons as well as patients with tendinopathy, to consolidate our understanding of tendinopathy, including tendon terminology,17 reporting of participant characteristics18 and core health domains.19 In the absence of ‘gold-standard’ diagnostic criteria for tendinopathy and a lack of consensus by the expert researchers and clinicians around diagnosis, and inclusion criteria for tendinopathy research, one of the ICON 2019 consensus papers reported standards for reporting participant characteristics to provide greater detail of who is included within research studies to facilitate clinical translation.18 Another ICON 2019 consensus statement provided a list of nine core health domains that should be considered in tendinopathy research: (1) patient rating of the condition; (2) participation in life activities; (3) pain on activity/loading; (4) function; (5) psychological factors; (6) physical function capacity; (7) disability; (8) quality of life; and (9) pain over a specified time.19 Furthermore, a number of other domains identified within the ICON 2019 statement of core health domains were considered of little importance in monitoring19; however, some did feature within the ICON 2019 consensus statement of reporting participant characteristics and are important to consider when investigating the diagnosis and monitoring of tendinopathy in clinical practice: (1) tendon structure; (2) palpation; and (3) range of motion.18 These health domains represent the first step in consensus on what outcome measures are important to clinicians, patients and researchers.
The irony is that clinicians have it drilled into them to be evidence based, but when it comes to assessment tools for mid-portion Achilles tendinopathy the research studies they read do not use uniform diagnostic criteria or assessment tools, and the experts cannot reach consensus on exactly what is needed to diagnose the condition. Therefore, can we really expect clinicians to select the most valid and reliable assessment tools?
To address the confusion within the research, the Achilles Tendinopathy International Consensus Sub-Group has worked to identify all assessments used within clinical studies of Achilles tendinopathy and allocate them under the ICON core health domain of ‘best fit’.14 This project involves further reviews and a Delphi study to determine which outcome measures are most valid and reliable and make recommendations regarding which assessments best represent each health domain. However, this body of work does not definitively indicate what current practice ‘at the coalface’ is for clinicians when diagnosing and monitoring Achilles tendinopathy. Specifically, there is merit in knowing what assessments clinicians use and what assessments clinicians consider ideal practice when diagnosing and monitoring Achilles tendinopathy. Further to this, if discrepancy exists between what clinicians do and what they consider ideal practice, it is vital we understand what the barriers to ideal practice are so that strategies can be implemented to address the barriers.
Objectives
The primary objective of this study was to explore the barriers preventing clinicians from implementing what they think is ideal practice as it relates to using tools to aid diagnosis and monitor progress in mid-portion Achilles tendinopathy. Our secondary objectives were to describe the assessments (assigned to an outcome measure domain they represent) employed by clinicians in their own practice to aid with (a) diagnosis and (b) monitoring progress in Achilles tendinopathy and explore which outcome measure domains clinicians believe to be the most and least important when managing patients with Achilles tendinopathy.
Methods
We conducted a qualitative study using semistructured one-to-one interviews. This study has been reported using the Consolidated Criteria for Reporting Qualitative Research20 to identify the descriptions and experiences of clinicians who treat mid-portion Achilles tendinopathy related to specific concepts of interest.
Concepts of interest
To address the objectives of our study, we developed a series of interview questions that were presented to clinicians (online supplemental appendix A). Each of the 10 questions relate specifically to our concepts of interest. Questions explored which assessments were performed in a ‘real world’ setting as well as any additional assessments clinicians would use in an ideal world to assist diagnosis and to monitor patient progress over time. Additionally, outcome measure domains (informed from the ICON core health domains) that the interviewed clinicians’ thought were the most/least important were also explored. Finally, clinicians were asked which outcome measure domains they believed indicated meaningful progress for patients and what barriers they perceived in implementing ideal practice for assessment and monitoring of patients with mid-portion Achilles tendinopathy.
Supplemental material
Patient and public involvement
This study did not involve patients; hence, they were not involved. Clinicians (acting as the population of interest) were invited to participate in this study.
Research team and reflexivity
Personal characteristics
Four members of the research teams conducted all interviews (JD, WG, MCM and MT) with personal characteristics described in online supplemental appendix B.
Relationship with participants
All participants were clinicians, identified by the research team through professional networks. To minimise relationship bias, we allocated interviewers (JD, WG, MCM or MT) based on having no relationship with the participant. There was no foreseeable bias within the characteristics of the interviewers.
Study design
Methodology
We employed a qualitative descriptive study design to capture the clinical assessments and outcome measure domains participants deemed important when assessing and monitoring mid-portion Achilles tendinopathy over time.21 Qualitative descriptive methodology is suitable in healthcare research as it helps to focus research questions directly on the experiences of participants rather than through researcher interpretation or a theoretical lens.22 Qualitative descriptive study designs are inherently simple, yet flexible, and allow researchers to perform descriptive research based on qualitative methodology.23 Furthermore, some of the key features of qualitative descriptive research include semistructured interviews or small focus groups, purposive sampling, descriptive statistics and thematic analysis24 making this research design ideal when considering our objectives.
Participant selection
We used purposive sampling25 to recruit Australian participants from four clinical subgroups: (1) junior physiotherapists, (2) senior physiotherapists working in private practice, (3) senior physiotherapists working in elite sport, and (4) sport and exercise medicine doctors (inclusion criteria for each group are listed within online supplemental appendix C). Purposive sampling is a non-probability sampling technique which selects participants who possess the maximum amount of information about a particular topic.26 We sampled continuously until thematic saturation21 27 was achieved (n=13), as determined by the principal investigator (MCM); however, we would have continued to sample further participants had saturation not been achieved.
We invited 28 participants into this study who were contacted by email and provided the participant information sheet, consent form, interview script (online supplemental appendix C) and instructions on how to enrol into the study. Of these, 15 participants either declined to be involved or failed to respond (five junior physiotherapists, two senior physiotherapists working in private practice, three senior physiotherapists working in elite sport and five sport and exercise medicine doctors). Overall, 13 participants (eight female, five male) from across Australia (online supplemental appendix D) consented to participate in this study. At the point of data saturation, two junior physiotherapists, five senior physiotherapists working in private practice, four senior physiotherapists working within elite sports organisations and two sport and exercise medicine doctors were enrolled.
Setting
All interviews were conducted between May 2020 and May 2021 using an online platform (Zoom Cloud Meetings28) with only the participant and the interviewer present.
Data collection
The duration of interviews ranged from 20 to 55 min and were audio recorded. We employed a cognitive interviewing technique following the conclusion of each of the first three interviews to ensure questions were understandable and facilitated discussion that addressed the concept topic. These participants were asked (1) if there were any questions they did not understand and (2) whether they felt the questions addressed the concept topics appropriately. Thereafter, we made minor amendments to the interview schedule to better explain the outcome measure domains with examples being provided for participants on request. The principal investigator (MCM) generated transcripts using Descript V.20.1.429 and subsequently cross-checked them with the audio recording. Final transcripts were not provided to participants for member checking.
Analysis
Data analysis
A single researcher (MCM) coded all data using QSR NVivo (V.12.6.1.970)30 under the guidance of a member of the research team (CB) who has substantial experience with QSR NVivo for qualitative research analysis. We sought significant statements that captured individual perspectives of participants. A template thematic analysis approach was used whereby the coding structure was guided by an initial skeleton code frame based on the concept of interest, and subsequently built on during the coding phase (coding structure presented in online supplemental appendix E).31 The clinical assessments mentioned by participants within script questions 1, 2, 6 and 7 were coded to one of the previously mentioned outcome measure domains, which acted as our themes (eg, the coding nodes within NVivo). The outcome measure domains were used due to the absence of any other relevant coding structures from existing literature, and because it has been established the ICON health domains are of interest to researchers, clinicians and patients. Where an assessment did not fit within one of the outcome measure domains it was included as ‘other’ to ensure that results were not biased by only presenting the domains identified within the ICON statement. For all questions related to participants selecting the most/least important outcome measure domains for assessment of monitoring, all responses were coded as the outcome measure domain directly indicated by the clinician. Themes were derived from the data related to the barriers for the implementation of ideal clinical assessment and monitoring.
Reporting
Results of the template thematic analysis are presented as figures or tables inclusive of the key themes and separated into the key topics of interest. Quotations were included as supporting statements to the key themes outlined within the results.
Results
Assessments used to assist diagnosis
Assessments performed by clinicians in a ‘real world’ setting
Clinicians identified assessments representing four key outcome measure domains they used most to assist diagnosis: function (85%, 11/13), pain on loading (92%, 12/13), pain over a specified time frame (77%, 10/13) and palpation (85%, 11/13) (figure 1A). Footwear was mentioned by 46% of clinicians as being assessed in routine practice and was coded under a separate outcome measure domain of ‘Other’.
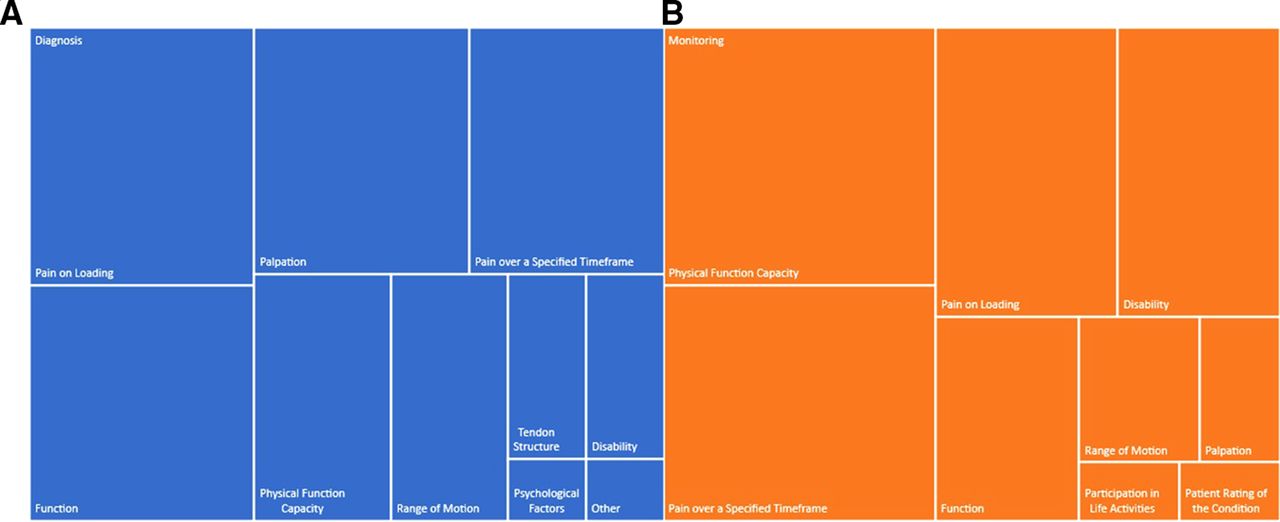
(A) Tree map representing the assessments clinicians perform in a ‘real world’ setting to assist diagnosis. (B) Tree map representing the assessments performed by clinicians in a ‘real world’ setting to monitor progress, where a larger box represents a larger response. Outcome measure domains that were not assessed by clinicians are not included within the figure.
Additional assessments clinicians would perform in an ‘ideal world’ setting
Clinicians identified three outcome measure domains of interest for assessments they would use in an ideal world: physical function capacity (54%, 7/13), disability (31%, 4/13) and tendon structure (31%, 4/13) (online supplemental appendix F). One clinician reported they would ideally assess calf circumference, and this was coded under a separate outcome measure domain ‘Other’. Clinicians felt in an ‘ideal’ world assessing physical function capacity using a force plate (eg, ground reaction force for jumping and landing), disability using self-reported outcome measures (eg, Lower Extremity Function Scale) or tendon structure using imaging (eg, ultrasound) would be valuable to assist diagnosis.
Outcome measure domains viewed as important by clinicians
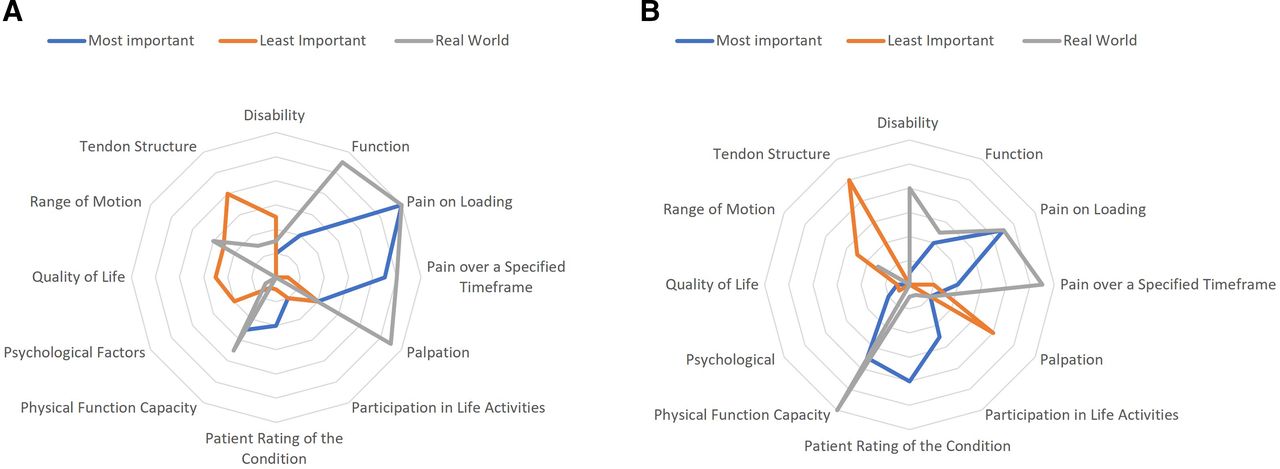
Clinicians identified assessments belonging to two outcome measure domains as being most important for diagnosing Achilles tendinopathy: pain on loading (92%, 12/13) and pain over a specified time frame (69%, 9/13) (figure 2A). Clinicians identified assessments belonging to one outcome measure domain as being least important for diagnosing Achilles tendinopathy: tendon structure (62%, 8/13)(figure 2A).
{kind=link}
{kind=link}
(A) Outcome measure domains clinicians view as important to assist diagnosis. (B) Outcome measure domains regarded as important by clinicians to monitor progress.
While 85% of clinicians routinely assessed palpation and 46% routinely assessed range of motion, these were not identified as important outcome measure domains for diagnosing tendinopathy. Only 31% of clinicians rated palpation in their most important outcome measure domains and no clinicians rated range of motion within their most important outcome measure domains (table 1). Themes representing clinically performed assessments used by clinicians for diagnosis yet not considering important outcome measure domains included palpation, which clinicians felt was expected by the patient, and range of motion which is assessed but not potentially useful for diagnosis.
Assessments clinicians routinely use within clinical practice when diagnosing Achilles tendinopathy, yet do not consider the underlying core outcome measure domain as important
Assessments used to monitor progress over time
Assessments performed by clinicians in a ‘real world’ setting
Most clinicians identified assessments belonging to four outcome measure domains as being used to monitor progress: disability (62%, 8/13), pain on loading (69%, 9/13), pain over a specified time frame (85%, 11/13) and physical function capacity (92%, 12/13) (figure 1B).
Additional assessments performed by clinicians in an ‘ideal world’ setting
Clinicians identified assessments belonging to four outcome measure domains they would assess in an ideal world: tendon structure (54%, 7/13), disability (15%, 2/13), physical function capacity (15%, 2/13) and function (8%, 1/13) (online supplemental appendix G). Clinicians felt in an ‘ideal’ world monitoring tendon structure using imaging (eg, ultrasound tissue characterisation), monitoring disability (eg, administering a Victorian Institute of Sport Assessment-Achilles) or monitoring ground reaction force (eg, through use of a force plate) would be valuable.
Outcome measure domains regarded as important by clinicians
Clinicians identified assessments belonging to three outcome measure domains as being the most important for monitoring progress: pain on loading (69%, 9/13), patient rating of the condition (62%, 8/13) and physical function capacity (54%, 7/13) (figure 2B). Clinicians identified assessments belonging to three outcome measure domains as least important for monitoring progress: tendon structure (77%, 10/13), palpation (54%, 7/13) and range of motion (38%, 5/13) (figure 2B).
Most clinicians (92%, 12/13) routinely monitor physical function capacity and 85% (11/13) routinely monitor pain over a specified time frame. However, only 54% (7/13) and 31% (4/13) of clinicians felt physical function capacity and pain over a specified time frame, respectively, were among the most important core outcome measure domains (table 2). Alternatively, no clinicians (0%) routinely assessed psychological factors, yet 15% (2/13) reported that psychological factors were one of the most important outcome measure domains (table 2). Participants recognised the importance of addressing the psychological factors among patients in monitoring progress, yet no participating clinicians actually did this.
Outcome measure domains regarded as important by clinicians to monitor progress
Defining meaningful progress
Clinicians found it difficult to articulate meaningful progress given that it is outcome measure specific. However, two key themes emerged: (1) clinicians are happy with progress provided they observe a positive trajectory (regardless of the magnitude of change), and (2) clinicians tend to have a finish goal they expect a patient to achieve (table 3).
Defining meaningful progress
Barriers to implementing optimal assessment
Clinicians identified several barriers to performing what they would consider optimal monitoring of their patients with Achilles tendinopathy (table 4). The four main themes were: ‘Financial constraints’ (9/13), ‘Time constraints’ (8/13), ‘Access to Equipment’ (4/13) and ‘Patients Symptom Severity’ (3/12), with eight other minor themes emerging. In terms of ‘Financial constraints’, clinicians were aware of the costs to patients in terms of deciding which course of treatment to recommend. Participants reported ‘Time constraints’ as being an issue to monitoring patients with the focus being on management as opposed to reassessment. Participants recognised that ‘Access to Equipment’ can be a problem in a shared clinical environment. Participants also reported ‘Patient Symptom Severity’ was a barrier to monitoring as they did not want to perform assessments likely to aggravate patient symptoms.
Barriers to implementing optimal assessment for assessment and monitoring of patients with mid-portion Achilles tendinopathy
Discussion
A plethora of different assessment tools exist to assist in the diagnosis and monitoring of progress for mid-portion Achilles tendinopathy. Despite this, no consensus exists on which of these tools are meaningful for use in clinical practice. The ICON 2019 consensus statement progressed the field by developing core health domains on which to map tendinopathy outcome measures.19 Building on this work, this is the first study to qualitatively explore the perceptions and experiences of clinicians in relation to assessment and monitoring of patients with mid-portion Achilles tendinopathy, with assessments mapped to the ICON 2019 core health domains.
The use of clinical assessments to diagnose Achilles tendinopathy
Clinicians commonly use assessments that measure function, pain on loading, pain over a specified time frame and palpation to assist diagnosis. Despite this, in our study, clinicians considered only pain on loading and pain over a specified time frame as being important outcome measure domains. Furthermore, we demonstrated that clinicians use, and consider relevant, some of the health domains classified by the ICON 2019 as ‘non-core health domains’. Specifically, clinicians reported routinely palpating the tendon and measuring range of motion as part of the diagnostic process for mid-portion Achilles tendinopathy. While palpation may be considered as useful for ruling out a diagnosis of Achilles tendinopathy, its value in prognosis is poor. Mechanical sensitivity of the tendon will also vary due to a number of different centrally mediated processes32 and should be interpreted with caution.
Of interest, while clinicians commonly assessed these outcome measure domains, they were not rated by clinicians as being essential for reaching a diagnosis. Our findings echo those in other conditions, such as low back pain and knee osteoarthritis, where a disparity exists between what is recommended and what is performed clinically.33 34 These findings highlight the heterogeneity of assessments used in clinical practice as diagnostic criteria for Achilles tendinopathy. This is an important finding as it means that there is likely to be substantial heterogeneity of clinical phenotypes within an Achilles tendinopathy population, even when diagnosed by healthcare providers.
The use of clinical assessments to monitor Achilles tendinopathy
Clinicians commonly measure disability, pain on loading, pain over a specified time frame and physical function capacity to monitor progress over time. When comparing the similarity of what assessments are being performed and what outcome measure domains clinicians thought were important, there was much more similarity within assessments used for monitoring, as opposed to diagnosis. For example, both pain on loading and physical function capacity were assessed in clinical practice and viewed as important by clinicians. However, we identified a disparity between some outcome measure domains that clinicians monitor to assess progress over time and those that clinicians think are the most important. For instance, some clinicians reported psychological factors as an important outcome measure domain yet they do not assess psychological factors within their clinical practice. It was also surprising to see very few clinicians mentioned that they would assess and monitor psychosocial factors throughout rehabilitation, in stark contrast to what is considered important for other musculoskeletal conditions.35 36 However, these findings reflect what has been seen in other musculoskeletal conditions with psychosocial screening tools not being routinely used.37 This may be explained by the several barriers clinicians identified that exist to implementing ideal practice.
Barriers to performing ‘ideal’ practice
Two clinicians reported they would not include additional assessments to assist with diagnosis and three clinicians reported they would not include additional assessments to assist with monitoring within an ‘ideal’ world scenario. This suggests that clinicians felt doing more would add value. However, there is no current evidence that suggests performing more assessments provides additional value or improves patient outcomes in mid-portion Achilles tendinopathy. In fact, the concept of ‘over-testing’ might actually be associated with harm.38
The main barriers to implementing what clinicians felt was ideal practice were ‘financial constraints’, ‘time constraints’, ‘access to equipment’ and ‘patients symptom severity’. These barriers reflect those identified in other chronic musculoskeletal complaints.37 39 Exploring these barriers in terms of their potential for modification, and thus the potential to optimise practice is warranted. Certain barriers could be removed at the individual level, for instance, by training clinicians to efficiently, effectively and routinely use patient-reported outcome measures. Likewise, other barriers could be removed at the institutional and cultural levels by optimising relationships and communication between different subgroups of clinicians. In contrast, we recognise barriers that exist which may not be modifiable. For example, clinicians concern that a patient’s financial constraints are difficult to overcome, although this does assume the clinician has established a thorough understanding of personal resources. This may not necessarily be the case and was not reported by physiotherapists working within elite sport where cost is not a barrier. While several strategies exist to remove this barrier, one solution is to avoid costly assessment protocols not supported by the evidence, such as imaging,40 and given the potential for iatrogenic effects related to overtesting this barrier might actually be useful. However, it should be acknowledged that some factors (such as geographical or cultural factors) influence whether imaging is a financial burden with many countries globally not having out-of-pocket expenses for patient imaging. These resources could then be redirected to fund ideal practice management, which could be mediated through clinician education. Likewise, the development of online, freely available resources for patients might assist in reducing the number of required consultations.41 The provision of better educational resources (either isolated or in conjunction with exercise rehabilitation) for patients may also help decrease the time burden clinicians identified as being a key barrier and are being trialled in other chronic musculoskeletal complaints such as chronic lower back pain.41 42
Access to equipment is difficult to overcome but the use of reliable measures of physical function capacity which do not require equipment should be encouraged (eg, single leg heel raise) as these may provide valuable information and negate the need for equipment.43 However, patient symptoms can significantly improve in the absence of any changes in calf endurance, as measured by a single leg heel raise,44 so the clinicians must be clear on why they are assessing physical function capacity. Patient symptom severity will always be a barrier in irritable presentations. However, assessments providing a measure of physical function capacity without increasing pain should be considered. The reality that outcome measure domain focus shifts during the clinical journey assists with this issue, with the initial focus being on pain-related outcome measure domains, then progressing to more disability and functional outcome measure domains as the patients’ clinical status improves.45
Limitations
We used one-on-one interviews as they can generate a range of themes on a per-person basis and provide very detailed transcripts for analysis.46 One-on-one interviews were used to ensure participants were comfortable with discussing their own barriers to ideal practice, specifically related to what they do not do as well as they could. For this reason, we decided against conducting focus groups as we believed participants would feel more comfortable in a one-to-one setting rather than in a focus group setting containing respected peers.27 As such, interviews are ideal practice for exploring the descriptions of the experiences and perceptions held by individuals and while they are associated with small sample sizes compared with larger quantitative studies they are rich in data and appropriate to answer the questions posed in this study.27
The ICON 2019 consensus statement of core health domains of tendinopathy is only recently published so it would be unlikely any large-scale change in clinical practice would have occurred. Hence, this study cannot assess the impact of the consensus statement, and only depicts what is currently being performed in clinical practice. Given the applicability of using the core health domains as nodes to code the data, we performed this for both diagnostic and monitoring measures mentioned by participants. However, we recognise diagnosis was never the purpose of the core health domains paper.
We interviewed a heterogeneous population of clinicians across disciplines and across career stages to capture breadth of perspective, which results in some limitations. First, our final sample only included one sport and exercise medicine physician and one sport and exercise medicine registrar. Therefore, sport and exercise medicine may be under-represented within our sample. Second, we did not include other healthcare providers who manage mid-portion Achilles tendinopathy (eg, podiatrists, exercise physiologists or general practitioners). Although thematic saturation was reached within the interviews conducted, the results are not intended to be representative of the broader population and cannot be assumed to represent other provider groups. Nonetheless, the findings were insightful, and generalisability could be rectified by future larger studies (eg, survey). Such a study could be developed based on the themes identified within this study and administered to large numbers of clinicians. This would provide more accurate estimates on the disparities between current clinical practice and ‘ideal’ practice, and what the barriers to ideal practice are. Furthermore, a survey could enable analysis of how demographic features such as specialty and experience might impact these perspectives.
Conclusion
No consensus exists that helps clinicians decide which clinical assessment tools assist in the diagnosis or monitoring over time of patients with Achilles tendinopathy. Assessments related to function, pain on loading, pain over a specified time frame and palpation are commonly used to assist diagnosis. Assessments related to disability, pain on loading, pain over a specified time frame and physical function capacity are used to monitor progress over time. Furthermore, pain on loading and pain over a specified time frame were considered the most important outcome measure domains for assisting diagnosis whereas pain on loading, patient rating of the condition and physical function capacity were the most important outcome measure domains for monitoring progress. Finally, four main themes were perceived as barriers to implementing ideal practice of assessment and monitoring in people with Achilles tendinopathy: financial constraints, time constraints, access to equipment and patient symptom severity.
Recommendations for clinicians on what assessments should be used in clinical practice should consider the barriers to optimal clinical assessment. Considering these barriers may assist compliance with recommendations in providing optimal clinical care for patients with Achilles tendinopathy.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The University of Notre Dame Australia Human Research Ethics Committee (approval number: 2020-014F). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @myles_physio
Contributors MCM, JD, EKR, WG and MT conceived the idea. MCM, CB, PC, JD, SD, WG, EKR and MT designed the methods. MCM, JD, WG and MT performed all interviews. MCM performed the data analysis. All authors contributed to developing the final manuscript. MCM is the overall study guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.