Article Text

Abstract
Objectives Provide a robust framework to provide a safe environment for return to training and competition of the US national soccer teams following domestic and international travel.
Methods US Soccer COVID-19 working group created a return to play manual for its national teams, prescribing discrete phases to return to training and competition. This was underpinned by strict health and safety and travel protocols for specific venues and persons. This was complemented by an aggressive testing cadence and isolation policies for delegations (players, internal and external support staff). Between September 2020 and April 2021, there were nine events for males and females at the youth, senior and Paralympic level, with international opponents hosted domestically.
Results In total, 6590 point of care (POC) (n=1810) and PCR (n=4780) tests combined were run. Overall positivity rate for players and staff in male events of 0.10% (n=2) and 0.00% (n=0) for females were recorded. Staff positivity rate was 0.14% overall, and external vendors 0.10%. Total POC and PCR positives in male events (n=2) occurred either the day of arrival or the following day.
Conclusion The implementation of strictly adhered to protocols and testing cadences yielded low positivity rates within team delegations. By comparison, initial league-wide COVID-19 testing in mid-2020 in other sports reported league-wide positivity rates of 2.9% (National Football League), 2.7% (Major League Soccer) and 5.3% (National Basketball Association). The English Premier League reported an increase in positivity rate in early 2021 from 1.22% to 1.74%.
With the implementation of regimented protocols and stringent testing, it is possible to hold elite-level international sporting competitions involving long-haul travel while ensuring continued safety during a global pandemic.
- COVID-19
- soccer
- sports medicine
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
This article demonstrates acknowledges that other domestic sports leagues around the world have experienced degrees of success in their return to play protocols during a global pandemic. The international sporting events are missing in this literature, however.
What this study adds
However, we have been able to show how a robust framework of health and safety protocols can facilitate a safe and effective return to training and competition for international soccer programme. Furthermore, maintaining these standards enabled multiple events across genders, youth and senior age categories while also supporting international travel of our own players and those of opposing Federations.
How this study might affect research, practice or policy
Indeed, this may serve as a necessary framework to allow sporting competition to continue safely in similar health scenarios in the future.
Introduction
COVID-19 spread rapidly across the world in early 2020, with the most recent data from the World Health Organisation (WHO) showing 147 million reported infections and over 3 million deaths worldwide.1 The serious threat to public health meant rapid measures had to take effect with the population subjected to quarantine and lockdown procedures in their respective nations at the request of local and national governments. Additionally, at local levels, further public health and safety measures were enforced, such as the wearing of masks and face coverings, regular hand washing and sanitising as well as practising social distancing. On a wider scale, a ban on most international travel was also put into effect in an attempt to curb the spread of the virus.
Obviously, there has been a huge impact on all aspects of modern life, with additional impacts on businesses, the economy and sporting environments. Many sporting events and competitions, such as the Tokyo 2020 Olympics, have since been rescheduled or even cancelled, causing large disruption to traditional sporting calendars. Consequently, lockdowns and suspension of sporting competitions means revenues are severely depleted due to losses from an absence of games and television/broadcast rights and spectators, which account for the majority of organisations income, up to 59% in the English Premier League.2
In the summer of 2020, domestic professional sports in the USA began to return to formal competition. Having completed periods of mandatory controlled training environments under the auspices of their respective governing bodies, soccer (National Women’s Soccer League, NWSL and Major League Soccer, MLS), ice hockey (National Hockey League, NHL) and basketball (National Basketball Association, NBA) teams held reduced format tournaments in controlled ‘bubble’ environments.
Hosted in one location, all teams were subjected to rigorous safety and testing measures to minimise the risk of virus transmission and provide an effective environment in which to train and compete. In their initial rounds of COVID-19 testing in June 2020, positivity rates of 2.7% (MLS), 5.3% (NBA) and 5.8% (NHL) from cohorts of 600 players, 300 players and 396 players, respectively.3–5
Despite the success associated with holding such events for domestic sports leagues, it took longer to be able to sanction any international sporting events and fixtures. There are, of course, inherent challenges associated with organising such events, including gathering athletes from various global origins, risk of exposure from air travel, provision of regular testing (athletes, team staff and external vendors), accommodation type, food provision, and maintaining social distancing at all times when not on the field of play.
Within the US Soccer Federation, a COVID-19 working group sought to create a manual for the safe return of its national teams (male and female, senior, youth and extended (Paralympic, beach and futsal)). Drawing from guidelines of FIFA (Fédération Internationale de Football Association), CDC (Centers for Disease Control and Prevention) and WHO as well as specific local restrictions, the manual provided a framework for the operation of national team training camps and matches.
In a pandemic whose status is highly fluid across all regions of the world, the manual provided guidance and required protocols for medical testing and screening, athlete and staff care, hotel and travel operations, training protocols, game operations, visiting federation team and match official protocols. This is similar to those outlined in the review of the major professional sports in the USA and Canada.6 US Soccer required all participating players, staff and referees to adhere to US Soccer’s protocols and testing for each camp and match. The group also recognised the potential to adapt the framework in line with an ever-changing landscape.
The main premise of this paper is to provide a robust framework to provide a safe environment for return to training and competition of the US national soccer teams following domestic and international travel during a global pandemic. The secondary emphasis is incorporating opponents to be part of the controlled environments created in an international-level soccer tournament
Materials and methods
In April 2020, the US Soccer Federation formed a COVID-19 working group to then create a robust framework for which its national soccer teams to follow to enable a safe return to training and competition. The return to play manual consisted of four discrete phases of progressively modified health and safety protocols according to the guidelines of FIFA, CDC and WHO. These phases consisted of; team training camp without matches, training camp with matches but no spectators, inclusion of matches with limited spectators and return to full capacity stadia with additional protocols.
Specific protocols mandated in the ‘controlled team environment’ are detailed in tables 1–3.
US Soccer Federation Procedures and Protocols (travel and base environment)
US Soccer Federation Procedures and Protocols (training facility)
US Soccer Federation Procedures and Protocols (COVID-19 testing)
The first training camps were held in October 2020, and followed in November and December 2020, January, February, March and April 2021.
Study populations
The nine training camps in this time period involved the senior men’s and women’s national teams as well as the U23 men’s youth national team and Paralympic national team. Ages ranged between 18 and 38. Training camp durations lasted between 7 and 30 days. The specific details, including locations and continent of origin of selected players, are in table 4. In the week prior to travelling, all members of the delegation attended mandatory virtual meetings where the intended protocols and procedures were presented. This was crucial for everyone’s education and subsequent compliance to then maintain the integrity of the controlled environment created. All participants gave informed consent to the US Soccer Federation and testing company used to undergo testing as necessary within the camp, with all results data confidential. Results were only accessible by the Chief Medical Officer and Medical staff leading each national team camp.
US Soccer national team’s calendar 2020–2021
Commercially available at-home COVID-19 PCR saliva tests from Vault Health were used for precamp and postcamp COVID-19 testing. Results were provided within 48 hours of sample collection. Vault Health states the sensitivity of their tests as 98% of all tests providing a conclusive positive or negative result (including new coronavirus variations), 2% inconclusive. The false-positive and false-negative result rate is 1%. The laboratory company used in national team camp testing protocols reported the Sofia SARS Antigen FIA lateral flow immunofluorescent sandwich assay and Roche Cobas assay to have a sensitivity of 95% limit of detection for SARS-CoV-2.

Schematic diagram of Federation testing cadence. POC, Point of Care.
Participants were not involved in the design, conduct, reporting or dissemination plans of our research. All participants had to submit to the testing protocols in order to be included in the national team event during the pandemic.
Results
In total, 8785 tests precamp/postcamp (n=1266), point of care (POC) (n=1803), PCR (n=5708) were run.

Testing results of US senior men’s and senior women’s national team players and staff.

{kind=link}
{kind=link}
{kind=link}
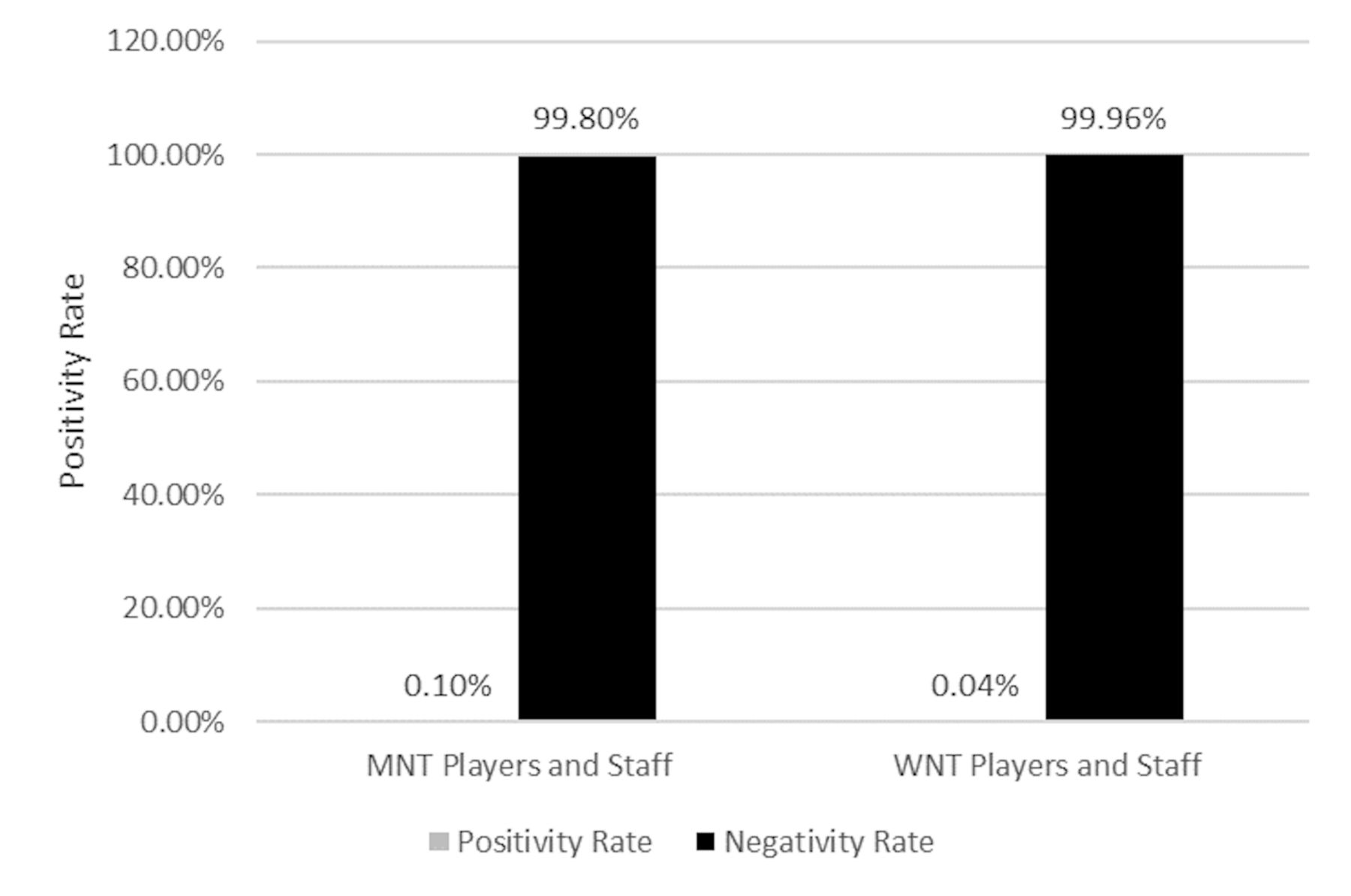
Positivity rate of US senior men’s and senior women’s national team players and staff.
Pre- and post-national team camp
The at-home tests provided before and after each national team camp had a positivity rate of 0.55% (n=1266).
The results in table 5show that the overall positivity rate from testing in national team camps, including all players internal and external staff, was 0.22% (n=8785).
National team players
The positivity rates for senior and U23 men’s national team players were 0.25% (n=1223). Positivity rates for senior women’s national team players were 0.16% (n=1255). Paralympic players positivity rate was 0.00% (n=15).
National team staff
Positivity rates for senior and U23 men’s national team staff were 0.26% (n=1177). Positivity rates for senior women’s national team staff were 0.07% (n=1524). In the Paralympic national team, the rate was 0.00% (n=9).
External vendors and staff
Positivity rates for senior men’s and women’s camp external vendors and the staff were 0.09% (n=1166).
Time point of positive tests
All positive tests were recorded within the first 2 days of arrival at the national team camp.
Discussion
This paper aimed to highlight the protocols and procedures put in place necessary to enable a return to play for national soccer teams. With the creation of a specific return to training and competitions manual, a robust framework was used to enable a safe environment for all in the delegation during the ongoing global COVID-19 pandemic.
With this in mind, nine international camps involving male and female senior and male youth teams took place over an 8-month period. Each of these entailed transporting players and staff from various global origins to be integrated free of COVID-19 into the teams ‘controlled environment’. This is the first testing data from an international soccer federation to show extremely low positivity rates, suggesting the effectiveness of the implementation of such protocols to maintain the safety and integrity of the environment during a global pandemic. Furthermore, this was also achieved while inviting international opposition delegations to fall under the same protocols.
Comparisons with other leagues
Our results highlight a positivity rate significantly lower than that previously reported in data published by national leagues and sports organisations. Our overall positivity rate (0.44% (n=7645) all delegates, 0.25% male players (n=1223), 0.16% female players (n=1255)) was lower than of the NHL in July 2020, 5.8% (n=2900 tests, 396 players) and 2.25% (n=12 000 tests, 1200 players) in January 2021 and the NBA (5.3% 302 players in June 2020, 8.8% 546 players in December 2020). In soccer, the reported positivity rate in MLS in June 2020 was 2.7% (n=668 players), with the English Premier League also higher than this study (1.22%–1.74%).3–5 7 It should be noted that the duration of testing is potentially different in the different sports due to the density of competitions and scheduling, as well as length of their respective seasons, which are likely to differ to timescales of US national soccer team events. As a result, COVID-19 testing prior to events may be more appropriate comparisons. For example, NBA, NFL, NHL and US Soccer all required two negative PCR tests to be returned to enter the event and allow safe. participation. Furthermore, NHL and NBA also detailed very similar protocol’s with regards to minimising COVID-19 infection risk. As with the US Soccer Federation return to play manual, protocols regarding testing, social distancing, face coverings, designated essential staff and processes pertaining to travel, provision of sanitised individual equipment and laundry services are all described.8 9 The robustness and success of the US Soccer return to play manual is however reflected in the unique circumstances of the coordination of players joining from all over the world. This entailed the communication and testing of individuals subject to potentially different restrictions in their home authorities before multisegment long-haul travel to join the camp and thus compete safely.
Strengths and limitations
Being the first to report diagnostic testing data regarding COVID-19 infection in an international soccer environment and with comparative success is very pertinent for global sport in the current circumstances. Moreover, holding events such as these, whereby players travel from all over the world, also incorporating opposition delegations, is evidence that defined and robust health and safety protocols can mitigate the risk of infection to hold international sporting events. These were largely centred around an aggressive testing cadence and the creation of a controlled camp environment. In particular, hosting an international female soccer tournament comprising of four other national teams (SheBelieves Cup) highlights their efficacy even more.
In addition to this, we also demonstrated the possibility to safely incorporate players based in other continents (Europe, Central and South America). Through strict pretravel, arrival, in-camp and postcamp return testing and safety measures, it was possible to prevent the occurrence of COVID-19 infection in our controlled environments.
However, when considering limitations associated with this study, it should be noted that direct comparisons between sports and populations may involve reporting of testing data that use differing testing companies, and therefore protocols for PCR/POC testing, which is subject to inherent variation and differing levels of reliability.10 Furthermore, these data were also collected at differing time points in the pandemic and may also reflect an evolution in virus education and awareness of best practices. Finally, the size of the reference population is also smaller in this study, given that it accounts for one national federation compared with entire domestic leagues consisting of multiple teams and athletes.
Conclusion
It is indeed possible to hold organised international sporting events, both with and without competitive fixtures, during a global pandemic. High-standard medical testing, reinforced by strictly adhering to local protocols, provide a safe environment in which to house these athletes following long-haul international air travel.
What are the findings?
A clear and comprehensive framework for health and safety protocols for short and long-haul travel, hotel spaces, food provision, training and match facilities should be defined before hosting any sporting event at any level during a global pandemic.
This framework, coupled with a high-level testing cadence, can help promote a low positivity rate and the safety of the host and visiting national team delegations.
Global education is critical to enhancing understanding of the situation and maintaining compliance when in the team environment.
What might it impact on clinical practice in the future?
This study shows the need for a coordinated approach between groups within the organising body. Key stakeholders from medical, administration, events, coaching and sports science departments should all communicate to ensure the most appropriate, robust framework is put in place.
Future large-scale, international events can employ a similar multi-disciplinary approach to ensure operation during a global pandemic.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval for the study was not required as this study qualifies as exempt research by the Institutional Review Board of Northwestern University (Chicago, Illinois).
Acknowledgments
The authors would like to acknowledge United States Soccer Federation COVID-19 task force for their detailed work and commitment on the draft of the return-to play manual. Additional appreciation of each team’s medical and safety staff for their tireless work in and out of camp. Finally, the players and staff, for their individual and team compliance, patience and adherence to the protocols which ensured a healthy and safe opportunity to return to sport.
Footnotes
Contributors GTC is the guarantor for the research study, also conceptualising the protocols and study design, AB organised testing provision and data storage, MB conducted data analysis and AG lead manuscript writing with GTC and AB.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.