Article Text

Abstract
Although it is advocated that end-users are engaged in developing evidence-based injury prevention training to enhance the implementation, this rarely happens. The ‘Implementing injury Prevention training ROutines in TEams and Clubs in youth Team handball (I-PROTECT)’ uses an ecological participatory design incorporating the perspectives of multiple stakeholders throughout the project. Within the I-PROTECT project, the current study aimed to describe the development of holistic injury prevention training specifically for youth handball players through using knowledge from both end-users (coaches and players) and researchers/handball experts. Employing action evaluation within participatory action research, the cyclical development process included three phases: research team preparation, handball expert-based preparation and end-user evaluation to develop injury prevention training incorporating both physical and psychological perspectives. To grow the knowledge of the interdisciplinary research team, rethinking was conducted within and between phases based on participants’ contributions. Researchers and end-users cocreated examples of handball-specific exercises, including injury prevention physical principles (movement technique for upper and lower extremities, respectively, and muscle strength) combined with psychological aspects (increase end-user motivation, task focus and body awareness) to integrate into warm-up and skills training within handball practice. A cyclical development process that engaged researchers/handball experts and end-users to cocreate evidence-based, theory-informed and context-specific injury prevention training specifically for youth handball players generated a first pilot version of exercises including physical principles combined with psychological aspects to be integrated within handball practice.
- Adolescent
- Ecological
- Handball
- Implementation
- Prevention
Data availability statement
Data are available from the authors on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known?
Evidence-based injury prevention training is highly effective in reducing musculoskeletal injuries in youth team ball sports under controlled conditions but has had limited public health impact because it is not widely or properly implemented or sustained in real-world sports settings.
The lack of engaging end-users at the individual (athlete and coach) and organisational (administration) levels to plan, develop and implement injury prevention training is an important contributor to insufficient implementation.
There are no injury prevention programmes available for youth handball players that target both upper and lower limbs or include psychological aspects of injury prevention
What are the new findings?
This study engaged end-users and researchers/handball experts in participatory action research to cocreate holistic injury prevention training specifically for youth handball players.
A cyclical development process was used, including three phases: research team preparation, handball expert-based preparation, and end-user evaluation, along with continuous rethinking and growing knowledge within an interdisciplinary research team.
A pilot programme was generated, encompassing examples of handball-specific exercises including physical principles of injury prevention (movement technique upper and lower extremities, respectively, and muscle strength) combined with psychological aspects (increase end-user motivation, task focus and body awareness) to integrate in handball practice warm-up and skills training.
Further studies may reveal if injury prevention training cocreated in a cyclical development process involving researchers and end-users helps make such training a regular part of handball practice.
Introduction
Although highly effective in reducing musculoskeletal injuries in youth team ball sports under controlled conditions, evidence-based injury prevention training has had limited public health impact because it is not widely or properly implemented or sustained in real-world sports settings.1 2 Not engaging end-users at the individual and organisational levels to plan, develop and implement injury prevention training (or any other health promotion intervention) is an important contributor to insufficient implementation.3–5 Collaborating with end-users provides insights into the implementation context,2 6 7 helps identify and overcome implementation barriers (eg, lack of motivation and context-specificity,8–12 and creates end-user ownership in an inclusive way with all voices heard.13 Moreover, social or behavioural theories can inform intervention development to improve programme adherence.14
Although youth handball players are vulnerable to lower and upper extremity injuries,15 16 available injury prevention interventions target either lower17 18 or upper19 limbs. Furthermore, it is recommended that injury prevention training combine physical and psychological interventions,20 as psychological training also reduces the risk of injury.21 To our knowledge, there are no injury prevention programmes available for youth handball players that target both upper and lower limbs or include psychological aspects of injury.
In this context, the ‘Implementing injury Prevention training ROutines in TEams and Clubs in youth Team handball (I-PROTECT)’ project was initiated through dialogue between end-users and researchers in 2015 with the overall goal to make injury prevention training part of regular handball practice in youth handball through a series of studies. While available injury prevention training for handball players commonly has a researcher-perspective focusing on evidence-based content and poorly described end-user involvement,17–19 I-PROTECT has an ecological participatory design incorporating the perspectives of multiple stakeholders (health beneficiaries, programme deliverers, policymakers) throughout the project.7 22 The first I-PROTECT study identified the facilitators among stakeholders at multiple levels that could help embed injury prevention training in regular training routines.7 The findings suggested that context‐specific injury prevention training, incorporating both physical and psychological aspects, and accompanied by a context‐specific implementation strategy should be developed in collaboration with stakeholders.7 End-users wanted to know and understand why and how injury prevention training works. They wanted a set of age-relevant, fun, varied and handball-specific exercises to integrate within handball practice. Psychological aspects of injury prevention can include coach communication, behaviour change, and providing feedback and creating a positive and accepting training environment. End-users also emphasised the importance of strong club leadership and support from the district and national handball federations, for example, by including injury prevention training in the coach education.7 Based on the first I-PROTECT study results, the next steps included developing the I-PROTECT model, an end-user-driven implementable intervention featuring evidence-based, theory-informed and context-specific injury prevention training, and an associated implementation strategy, as described in a recent planning paper.22
This study aimed to describe the development of an injury prevention training programme specifically for youth handball players, incorporating knowledge from coaches, players and researchers/handball experts.
Material and methods
Action research as theory and practice
The I-PROTECT project is methodologically framed by the principles of action research, which ‘brings together action and reflection, theory and practice, in the pursuit of practical solutions to issues of pressing concern’.13 In contrast to other forms of applied research, action research implies ‘pragmatic cocreation of knowing with, not on about, people13’ in a cyclical developmental process, where researchers and stakeholders collaborate in a common project. In this study, the cyclical development process corresponded to the research team’s knowledge progress informed by input from stakeholders at different stages towards the outcome, that is, a first program version. Given that action research is a broad methodology with various research practices, the I-PROTECT project is further defined as a participatory action research (PAR) practice in which action evaluation (AE) is used as a specific PAR method. In AE, stakeholders are asked to define what goals they have, why these goals are important, and how they should be achieved before evaluating the goal-related activities in practice.23
Stakeholder engagement can be monitored on a 5-point rating scale, where very low (1) indicates that researchers make all decisions, moderate (3) that stakeholders contribute to decision-making, but researchers make the final decision, and very high (5) that stakeholders are involved in all decision-making.24 The current study is high (4) on this scale. The I-PROTECT project was initiated during a dialogue between researchers and end-users, in which end-users expressed that they wanted to use injury prevention training but needed help to do so. Therefore, our first I-PROTECT study explored the end-users’ needs and showed that they wanted to understand the importance, benefit and principles of injury prevention training (why) and have a set of handball-specific exercises (what) to integrate within handball training (how and when).7 Hence, in this study, key stakeholder representatives in the planning group underlined that they wanted researchers/handball experts to initiate the development of exercises. End-users would then test and evaluate exercises in practice in line with AE. Results from each phase were presented to key stakeholders in the planning group to enable discussions and agree on how to proceed to the next phase.
Guiding process
The starting point of this study was the results from the first I-PROTECT study in which end-users’ needs were identified.7 We then: (1) identified and synthesised research evidence and clinical experience; (2) consulted relevant experts and (3) engaged end-users to ensure their needs, capacity and values were considered. These align with the three first steps of the generalisable six-step intervention development process.6
Employing PAR and the guiding process, the current study included three phases: research team preparation, handball expert-based preparation, and end-user development and evaluation to develop the first draft of an injury prevention training programme. To grow the research team’s knowledge, rethinking was conducted within and between phases based on participants’ contributions (figure 1).

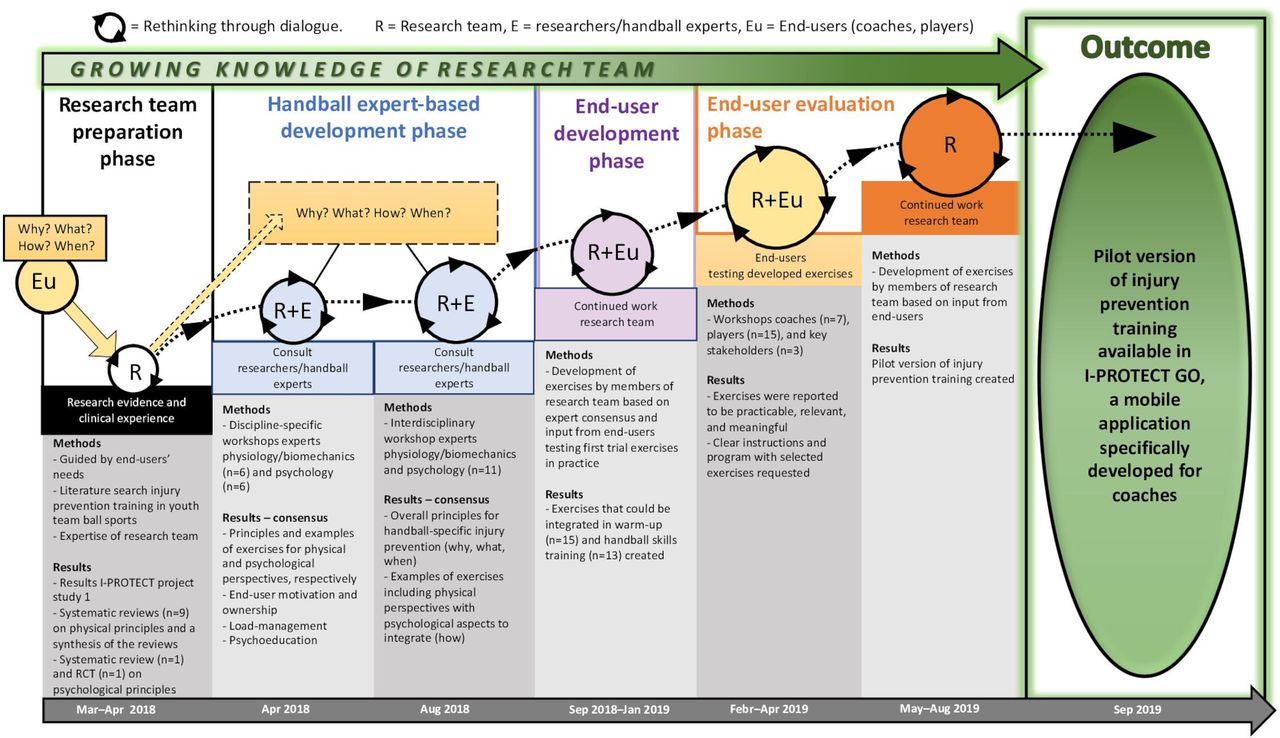{kind=link}
Development of pilot version of injury prevention training for youth handball players available in I-PROTECT GO, a mobile application specifically developed for coaches. The starting point was end-users’ needs identified in our first I-PROTECT project study.7 I-PROTECT, Implementing injury Prevention training ROutines in TEams and Clubs in youth Team handball.
Research team preparation phase
Systematic reviews and randomised controlled trials (RCTs) published in the peer-reviewed literature in the past 5 years were reviewed to identify physical and psychological principles of effective injury prevention training. Literature was also reviewed to identify key challenges to implementing injury prevention interventions in community youth team ball sports. The collective knowledge and experience of the research team of theory, evidence and practice, including end-users’ needs identified in our first I-PROTECT study,7 was also employed.
Handball expert-based development phase
Experts with relevant knowledge within the research field and/or implementation context living within reasonable travel distance from Sweden were identified and contacted by members of the research team (EA and SB). Sixteen experts were invited, and five declined to participate due to lack of time. The 11 experts (8 PhD, 2 MSc and 1 BSc degree) had research and/or clinical knowledge in sports medicine or sport psychology, and all handball knowledge (player, coach and/or coach instructor) and/or knowledge in physical/psychological development in youth.
Three structured 1 day face-to-face workshops—two discipline-specific (sports medicine and sport psychology, respectively) and one final interdisciplinary—were held to develop injury prevention training specifically for Swedish youth handball players. One expert participated in both discipline-specific workshops as she had knowledge of both physical and psychological aspects of handball. Two experts (one in sports medicine, one in sport psychology) could not attend the interdisciplinary face-to-face workshop but gave feedback on the results. The experts were provided with the outcome of the research team preparation phase and a summary of the results from the first I-PROTECT study,7 before the workshops via an Open Science Framework (Centre for Open Science, USA) homepage.
The workshops aimed to identify and reach consensus on principles and propose examples of exercises of injury prevention training for youth handball players. The experts were asked to consider the following key aspects from stakeholders’ perspective, identified in the first I-PROTECT study7: to know and understand the importance, benefits, and principles of injury prevention training (why); be given examples of exercises that are age-relevant, fun, varied and handball-specific (what); and exercises that could be integrated in handball practice (how, when). Nominal group technique25 26 was used in the workshops including27: (1) Introduction and explanation (ie, study background and specific aim); (2) Silent (individual) ideas generation; (3) Sharing ideas without debate; (4) Group discussion and (5) Consensus. Sharing ideas and group discussion were first done in small groups (two or three participants), then in the whole group. Consensus discussion was performed in the whole group. Workshop participants documented their results. Handballs were used, and the proposed exercises were practised in small groups and the whole group. Research team members circulated between the groups to answer questions and/or reinforce the task(s) and goal of the workshop and ensure that the key aspects from the stakeholders’ perspective were considered. When needed, the research team ensured progress by emphasising the frame of the task. Research team members (EA and SB) planned, facilitated, and synthesised the results from each workshop. The experts reviewed and provided feedback on each synthesis, and then all agreed on a final version. The results from the workshops were discussed with the key stakeholders before the research team developed the exercises into a first programme draft.
End-user development and evaluation phase
The initial end-user acceptability of the first programme draft was evaluated in structured workshops with youth handball coaches (programme deliverers) and players (programme participants and beneficiaries). Coaches and players were recruited from the youth teams in the two community handball clubs participating in the I-PROTECT project. Eight coaches (all males) and 15 players (15–17 years, 8 females) volunteered to participate. Members of the research team (EA, SB and JL) led and facilitated the workshops, and a representative (n=3) from each of the two clubs and the regional handball federation (responsible for club/federation operation) participated in the workshops. The workshops started with an introductory didactic session to provide participants with information about the I-PROTECT project, current research evidence and results from study 1,7 and a summary from the researchers/handball expert workshops. Participants were given examples of exercises intended to be integrated into handball practice (warm-up and handball skills training) and practised the exercises. To evaluate acceptability,28 coaches were asked if exercises were practicable (ie, easy/difficult to put into practice), relevant, and/or meaningful. They scored individually as a yes/no answer together with any comments on a sheet. In addition, discussions with coaches and players were continuously facilitated (after each exercise, warm-up exercises, and handball exercises, respectively), and the received feedback was summarised to ensure mutual understanding. Finally, in group discussions with coaches and players, respectively, they were asked their perceptions about usability,28 to ensure their perspectives and suggested revisions were considered. These group discussions aimed to get feedback from coaches and players and agree on exercises that were easy to understand and use, efficient, acceptable, appealing and valuable. Research team members developed the exercises into a second programme draft based on feedback from coaches and players.
Reflexivity
Given the asymmetrical power relationship between experts and practitioners, particularly when youth are involved, we anticipated that the youth might hesitate to express their actual experiences (eg, if an exercise felt uncomfortable) or opinions (eg, if they did not enjoy the programme). Therefore, we engaged in continuous dialogue with participants following the PAR methodology. The interdisciplinary research team represented different expert fields (both theory and practice), that is, sports medicine (EA), sport psychology (SB) and handball (JL) and adopted continuous reflection to reinforce rethinking and growing knowledge (figure 1), as reported in previous PAR studies.29 The joint reflective knowledge process sometimes required thoroughly discussing the meanings of different key concepts and interpreting results to reach a common understanding. These discussions resulted in a more complex and pragmatic understanding than would be possible from a single discipline approach. The research team indicated and emphasised that all participants (coaches, players, researchers/handball experts) were experts within their field(s) to encourage and optimise input, creativity and feedback.
Results
The main results are provided in figure 1.
Research team preparation phase
Nine systematic reviews, including physical principles, along with one systematic review and one RCT on psychological principles of effective injury prevention training in youth team ball sports, were identified. Literature on key challenges to implementing injury prevention interventions in team ball sports, that is, lack of time and interest, lack of programme variation, low priority, lack of context-specific training, lack of support, was also identified. The research team’s experience included knowledge of existing injury prevention training programmes for team sports, particularly handball (Fittoplay.org and a Swedish knee control programme), expertise in implementation science and behaviour change, and knowledge of the implementation context from our first I-PROTECT study. The literature identified is provided in online supplemental appendix 1.
Supplemental material
Handball expert-based development phase
Discipline-specific workshops
The sports medicine experts agreed on physical principles and examples of exercises, and to increase player/coach motivation and ownership (online supplemental appendix 2). Generally, exercises were to be integrated into handball practice. Some exercises (eg, throwing) could be performed before training when waiting to access the courts, and muscle strength exercises could be integrated into either warm-up (all ages) or strength training (older players). The sport psychology experts agreed that the main aspect should be reducing stress levels with focus areas for the individual, team, and organisation. Generally, sport psychology exercises and perspectives were outlined (online supplemental appendix 3).
Supplemental material
Supplemental material
In both workshops, experts agreed on the following overall guidance/principles to increase motivation and end-user (player, coach) ownership of exercises: age-relevant (younger 13–14 years, older 15–17 years); sport-specific and meaningful; fun, varied, challenging and progressions of difficulty; player-attractive and coach-attractive (packaging); injury prevention and performance-enhancing; and use role models to demonstrate exercises (eg, films as in fittoplay.org). The existing guidelines employed by handball coaches in Sweden, that is, use of a ball, perceived fun, and high activity were thought to help integrate the training within the regular practice.
After summarising the results, the research team and experts agreed that the organisational perspective, load-management (physical and psychological perspectives), and packaging would be developed in future project work.
Interdisciplinary workshop
A consensus was reached about the overall principles on why handball-specific injury prevention is important (reduce injury, enhance performance, fun, more players available), what components to include in exercises (handball-specific, meaningful, fun, skill development, the external focus of attention, cooperation, competition, mindfulness and task focus, throwing and also jumping with/on the non-dominant side for symmetry), and when to perform (prewarm up, start-up, warm-up, handball skills training, fitness training (all ages) and strength (15–17 years)). It was also agreed that the proposed exercises were relevant for males and females. Thus, no gender-specific exercises were suggested. Specifically, examples of exercises including a holistic view were developed from four physical perspectives (movement technique lower extremities, movement technique upper extremities, muscle strength, and all-round training for physical fitness) and three psychological perspectives (decrease stress and increase task focus, increase motivation through applying self-determination theory (SDT), and external focus of attention) (table 1, online supplemental appendix 4). At the end of the workshop, it was agreed that further work was needed to develop handball-specific injury preventive strength exercises and sport psychology exercises.
Supplemental material
Consensus from the interdisciplinary workshop with experts in sports medicine and sport psychology including four physical perspectives and psychological aspects to integrate
Continued work in the research team
Based on the results from the expert consensus and subsequent discussion with key stakeholders, research team members (JL, EA, SB) continued to develop exercises to integrate within warm-up and handball skills training. A team member (JL), who is also a coach, tested trial exercises with players to receive their input and to evaluate, from a coaching perspective, whether exercises were feasible to perform at handball practice (figure 1). Handball-specific exercises were developed to target lower extremities, upper extremities, and muscle strength, respectively, with integrated psychological aspects (increase end-user motivation, task focus and body awareness) (table 2). Muscle strength exercises targeted the core, although several exercises also targeted leg and shoulder strength. Based on our clinical experience, grip/wrist strength training was added and integrated into relevant exercises to enhance performance and ensure handball-specific exercises. General aspects of injury prevention, that is, balance, coordination, posture and/or flexibility, were included in several exercises.
Examples of handball-specific injury prevention exercises (n=26) including physical principles and integrated psychological aspects developed by research team based on the results from expert consensus and subsequent discussion with key stakeholders, and feedback from coaches (n=7) and players (n=15) from workshops
End-user development and evaluation phase
Workshops with coaches and players
Feedback from coaches and players (see table 2) aligned with autonomy (eg, meaningful exercises), perceived competence (eg, progression of difficulty), and relatedness (eg, pairwise exercises) (table 2). All coaches reported that the exercises were, in principle, practical (ie, able to put into practice), relevant and meaningful to incorporate in warm-up and handball skills training. Some coaches perceived that three exercises were not relevant or too difficult to put into practice for younger players. Coaches requested clear instructions (why and how) for each exercise and examples of correct/incorrect movement techniques. They requested a programme including selected exercises instead of a bank of exercises to choose from. They also wanted the exercises available on a digital platform. Players perceived the exercises as fun, relevant, and handball-specific and indicated that clear instructions (why and how), as well as pair and group exercises, enhanced motivation for uptake. Two physical fitness exercises (obstacle course and dance) were discussed as an optional warm-up, and coaches and players believed both could work for all ages. However, these exercises were not prioritised at this stage of programme development.
Continued work in the research team
Research team members (JL, EA, SB) continued developing the exercises based on coach and player feedback, for example, include clear instructions for exercises (why, how, movement technique and feedback) and provide an example programme (table 2). This generated a pilot version of exercises including physical principles and psychological aspects to be integrated into handball practice (figure 1, table 3). Information Technology consultants were appointed to produce a mobile application prototype, called I-PROTECT GO, including this pilot version of the programme.
Pilot version of injury prevention training including exercises integrated within warm-up and handball skills training, respectively
Supplementary video
Supplementary video
Supplementary video
Supplemental material
Discussion
In this study, researchers/handball experts and end-users cocreated holistic injury prevention training specifically for youth handball players. A cyclical development process including multiple phases, rethinking and growing knowledge generated a first pilot version encompassing examples of exercises informed by physical principles combined with psychological aspects to integrate into warm-up and skills training within handball practice.
In most previous work, researchers and/or clinicians developed injury prevention programmes to evaluate efficacy in controlled trials30–33, with little or no end-user engagement. In this study, we cocreated injury prevention training by applying PAR and using a cyclical development process including dialogue between researchers and stakeholders, and continuous collective reflection and rethinking to grow knowledge within an interdisciplinary research team. This process aimed to facilitate sustained and high-fidelity delivery and practice of injury prevention training. PAR is particularly appropriate for this as it involves stakeholders throughout the research process. As a result, they see the practical value of the outcome as it reflects their perspectives.
The literature search identified several systematic reviews, including physical perspectives of injury prevention within team ball sports, but few studies on psychological perspectives. This was expected as psychological interventions are rare in this context.21 Knowledge of the implementation context is important to facilitate the adoption and sustained use of evidence-based injury prevention training.34 Therefore, results from our first I-PROTECT study were crucial in this programme development phase as these identified facilitators among stakeholders at multiple levels, which could help injury prevention training become part of regular training routines.7 These results,7 and the identified research evidence, were discussed within the planning group and underpinned subsequent phases.
To avoid an overly complex task initially, research team members decided to start with discipline-specific workshops with the researchers/handball experts. This enabled participants to interact and develop knowledge within their intellectual comfort zone before generating more multifaceted knowledge in the subsequent interdisciplinary workshop. Although the experts agreed on overarching physical and psychological principles and proposed examples of exercises, it was challenging to develop handball-specific exercises incorporating both physical and psychological principles that could be integrated into different parts of handball practice. In contrast to our holistic approach, existing injury prevention training (eg, Fit to play, FIFA 11+, Knee Control) appears to be less complex with a focus on physical aspects only (mainly lower extremity) and is typically part of, or an optional, warm-up. After consensus from the interdisciplinary workshop, research team members continued to develop handball-specific injury preventive exercises focusing on physical perspectives incorporating psychological aspects integrated within warm-up and handball skills training that the end-users tested and evaluated.
Few previous studies have involved end-users in programme development. In one study, end-users provided feedback on a programme developed by a research team,6 and in another study, end-users identified critical elements to include in an injury risk reduction program.35 We started our study with end-users’ needs, and coaches and players tested and evaluated exercises during development. Feedback from coaches and players was generally well aligned with SDT (ie, autonomy, perceived competence, and relatedness) (table 2), a framework for understanding factors that promote motivation,36 that the experts agreed should be applied in the exercises. Coaches and players also generally perceived the exercises as meaningful, handball-specific, varied and fun, suggesting that the exercises addressed the key needs of stakeholders.7 Sport-specific and fun exercises have been identified as facilitators by others,8–11 as well as exercises that may enhance performance,11 while lack of motivation, enjoyment, engagement, sport-specificity and variations are frequently identified barriers to uptake of injury prevention training.8–12 Feedback for improvements included having clear instructions about why (purpose and relevance to handball) and how (correct/incorrect movement technique, video of exercises) and the progression of exercises for variation. End-users also requested a typical programme, not just a bank of exercises, via a digital tool to support self-management, adoption, and uptake. After the end-user workshops, research team members developed the first version of injury prevention training, which was then evaluated by coaches and players.37
The main strength of this study is that PAR was applied, where coaches, players, and researchers/handball experts collaborated to cocreate the programme based on interdisciplinary research evidence and end-users’ perspectives. The cyclical development process enabled the research team to rethink and grow knowledge through dialogue with researchers/handball experts, end-users, and key stakeholders. To our knowledge, our pilot version of injury prevention training is the first programme that includes a holistic approach. Moreover, we incorporated injury preventive principles into handball-specific exercises for regular handball practice. Another strength is the interdisciplinary composition of the research team, where all researchers contributed with valuable disciplinary expertise and relevant practice-based experience. Although an interdisciplinary approach is valuable, it is not without challenges. Increased understanding of another discipline area and merging perspectives into higher levels of learning and knowledge required extra time for reflection and rethinking. Replacing discipline-specific workshops with interdisciplinary workshops was considered too complex and difficult but could have diminished paradigm-specific starting points. There are also other limitations to acknowledge. Although the feedback from coaches and players is likely representative of other teams, the generalisability of the findings may be compromised due to the two participating clubs being active in the same city. Because youth handball is voluntary work for coaches and undertaken during the spare time for players, end-users had limited time to participate despite their high interest in participating in the study. The collaborative and reflective process used in our study was time-consuming. Further studies could explore more efficient ways to cocreate an evidence-based, theory-informed and context-specific injury prevention training programme. Finally, we cannot exclude the possibility that a different research team and a group of end-users would generate other results. Nonetheless, the outcomes of this study make a valuable contribution to developing safer handball training for youth.
Conclusion
A cyclical development process that engaged coaches, players and researchers/handball experts to cocreate evidence-based, theory-informed and context-specific injury prevention training for youth handball players, generated a first pilot version of exercises including physical principles combined with psychological aspects to be integrated within handball practice. The pilot version was made available in a mobile application (I-PROTECT GO), specifically developed within the I-PROTECT project, for coaches to test and evaluate with their teams. A need to further develop injury preventive strength exercises and sport psychology exercises was identified.
Data availability statement
Data are available from the authors on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Regional Ethical Review Board in Lund, Sweden. Reference number: EPN 2014/713. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the key stakeholders and the participating coaches and players. The authors also thank Dr Louise Thoma for conducting the literature search and summarising current relevant literature for physical perspective of injury prevention in youth team sports, as well as LU Innovation (hub for innovation at Lund University) for collaboration with producing the first prototype of the mobile application I-PROTECT GO.
References
Supplementary materials
Footnotes
Twitter @EvaAgeberg
Contributors EA, SB and EMB designed the study, and AD and JL contributed to this process. EA and SB were responsible for data collection, and JL assisted in this process. JL, KM, EAd, AB, JE, SG, UJ, KL, GM, MM and UT participated in workshops in the handball expert-based development phase and provided feedback on syntheses from the workshops. EA and SB analysed and interpreted data, and EMB, KM and JL provided feedback. EA drafted the manuscript. SB contributed to the writing about psychological perspectives, and EMB about participatory action research methodology. SB, EMB, KM and JL provided feedback on early versions of this manuscript. AD, EAd, AB, JE, SG, UJ, KL, GM, MM and UT provided feedback on later versions of the manuscript. All authors read and approved the final version of the manuscript, and agreed with the order of presentation of the authors. EA is responsible for the overall content as guarantor.
Funding This work was mainly supported by the Swedish Research Council for Sport Science and the Crafoord Foundation. Grants were also received from Anna-Greta Crafoord’s foundation, Kock’s foundation, Magnus Bergvall’s foundation, Alfred Österlund’s foundation and Sten K Johnson’s foundation. No funding bodies were active in study design, data collection, analysis or interpretation, nor in preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.