Article Text

Abstract
Objective Sport and Exercise Medicine (SEM) Masters curricula vary. This Delphi study is aimed to create a consensus curriculum for doctors undertaking SEM Masters courses.
Methods A modified Delphi survey was used. An expert panel was established of individuals deemed to have adequate knowledge of the field. The research group developed the initial draft of the curriculum by collating and reviewing previously published UK-based postgraduate SEM-related curricula. There were two phases. In phase 1 the expert group either accepted, rejected or modified each learning objective (LO). During phase 2 the expert group were asked to accept or reject each LO that did not get accepted outright previously. The research group analysed the levels of agreements and the comments given by the expert panel after each phase.
Results The expert panel consisted of 45 individuals, with 35 completing phase 2 (78% retention rate). Of the 136 LOs initially collated: 71 (52%) were accepted outright, 60 (44%) were altered in some way and reincluded in phase 2, and 5 (4%) were removed after phase 1. The research group added 2 (1%) new LOs on reflection over comments made by the expert panel. The final curriculum contained 133 LOs, divided into 11 subthemes.
Conclusions The findings will better inform educators when developing SEM Masters curricula and inform students what they should look for when considering an SEM Masters. This consensus curriculum is an important step in standardising postgraduate SEM education.
- education
- sports & exercise medicine
- sports medicine
Data availability statement
No data are available. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
key messages
What are the new findings
This Delphi study has produced an up-to-date consensus on what skills and knowledge are expected of an individual with a Masters in Sport and Exercise Medicine (SEM) in the UK.
Practical skills such as ultrasound, joint and soft tissue injections and compartment pressure testing were deemed too specialised to be included in SEM Masters curricula.
How to develop and deliver exercise medicine services and musculoskeletal services were also deemed inappropriate to include on SEM Masters curricula.
What is already known
An important aspect in the ongoing evolution of SEM is ensuring adequate SEM skills and knowledge in individuals working as SEM clinicians.
There is currently no standardisation of SEM Masters courses in the UK.
Introduction
Sports and Exercise Medicine (SEM) became established as a specialty in 2005 in the UK and this has driven increasing demand for education on its core components.1 SEM postgraduate education varies throughout the world. Some countries offer postgraduate courses in SEM, such as Masters of Science or Postgraduate Diplomas.2 Within the UK, there is currently no consensus on what learning objectives (LOs) should be included within both SEM Masters and Diploma courses. Consequently, students undertaking postgraduate SEM qualifications at different universities will develop different skills, leading to less standardisation of clinicians employed in SEM posts.
Increased integration of SEM into the National Health Service (NHS) could provide significant benefits.3 An important aspect for the evolution of SEM in the UK is ensuring the development of SEM curriculum for every level of training. Many SEM jobs in the UK require having an SEM Masters in their eligibility criteria. However, there is limited previous research looking into what a Masters course in SEM should include. A study in 2005 in the UK developed LOs for an ideal SEM Masters course, although how the findings influenced or were implemented into curricula is unknown.2 This Delphi study aims to develop an up-to-date consensus on what skills and knowledge are expected of an individual with a Masters in SEM in the UK. This will aid in creating a unified and standardised SEM Masters education by universities throughout the UK. It will also ensure students can appreciate whether their SEM Masters education has provided the necessary skills and objectives to work as a competent SEM clinician.
This study has focused specifically on what LOs doctors undertaking an SEM Masters should hope to achieve. It should be noted that other healthcare professionals also undertake Masters degrees in SEM, and the LOs for these groups are likely to be different due to their role within the multidisciplinary team.
Methods
Study design
A modified Delphi survey was used to seek consensus on a postgraduate SEM Masters curriculum for doctors. Expert contributions to the study remained anonymous to the research group, in keeping with the principles of Delphi methodology.4
Establishing the research group
The research group included the authors DV, KRM, PB, CN, AP and GF. The research group were selected due to their experience in medical education. DV, CN and AP have experience in the exercise medicine sector. DV and CN have experience in delivering SEM education. DV and KRM have undertaken a Masters in SEM. GF and PB have experience in Delphi methodology. DV and KRM have experience in the education of early career SEM professionals through British Association of Sport and Exercise Medicine (BASEM) and roles within UK Universities. Content decisions were finalised by the research group.
Expert Delphi panel
Experts are defined as individuals with knowledge and experience. For this study, they must have adequate knowledge in postgraduate SEM education.5 6 Invitations to express interest in being on the expert panel were emailed to all members of the BASEM and the Faculty of Sport and Exercise Medicine (FSEM) via their mailing lists. In addition, members of the research group shared invitations to submit interest in being on the expert panel via social media.
In their expressions of interest individuals were asked demographic information and questions selected by the research panel to determine eligibility. The following eligibility criteria were used:
Doctors that have completed their Foundation Training.
Hold a higher qualification in SEM: specifically either an SEM Masters degree or diploma. Alternatively, they could have membership or fellowship of the FSEM (MFSEM/FFSEM)
Have been a doctor for more than 5 years
Working in the UK at the time of the study.
The research group reviewed the responses and removed those that did not match the eligibility criteria. Regarding the size of the expert panel, a panel size of more than 30 is not considered to improve the quality of the study.4 7
Development of the initial curriculum
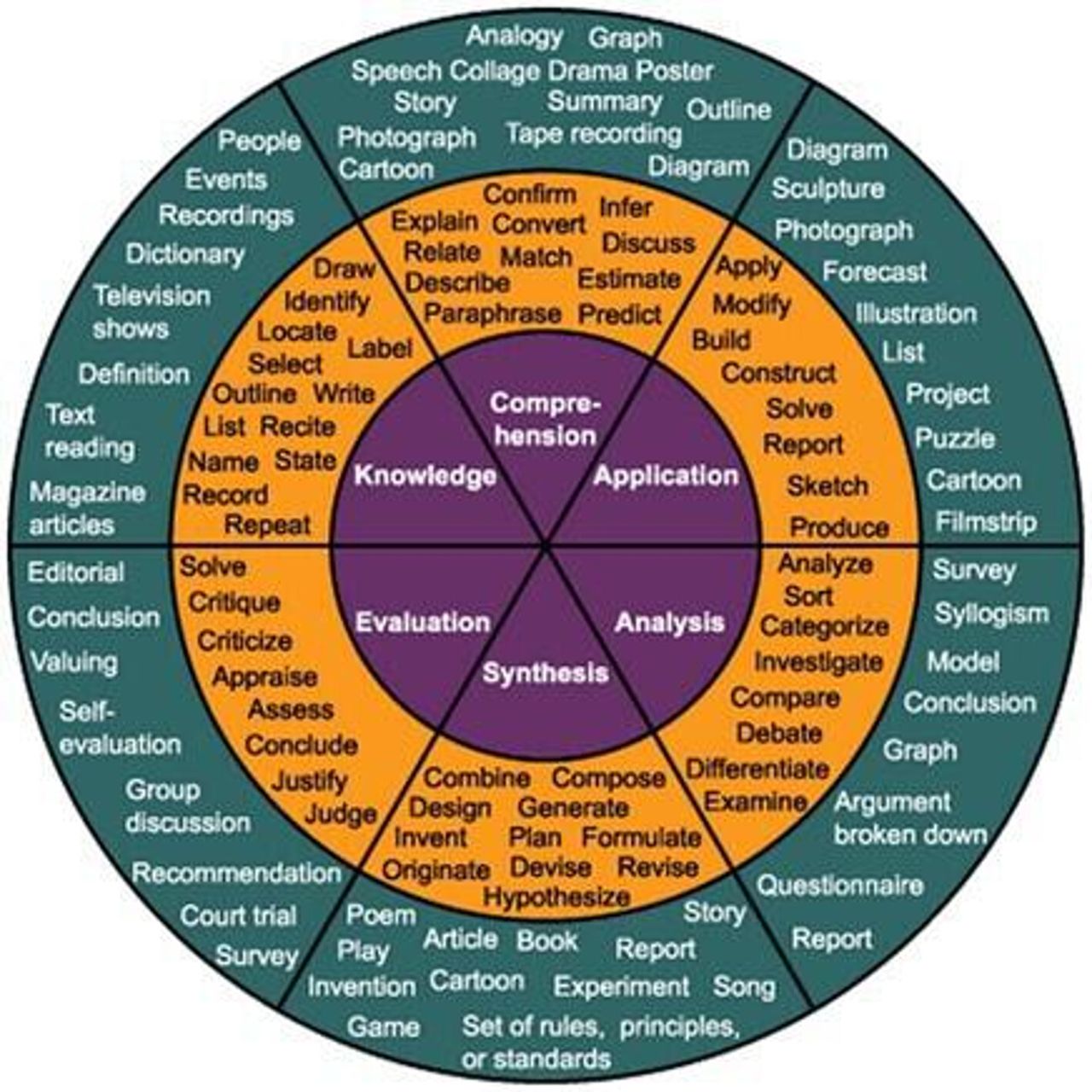
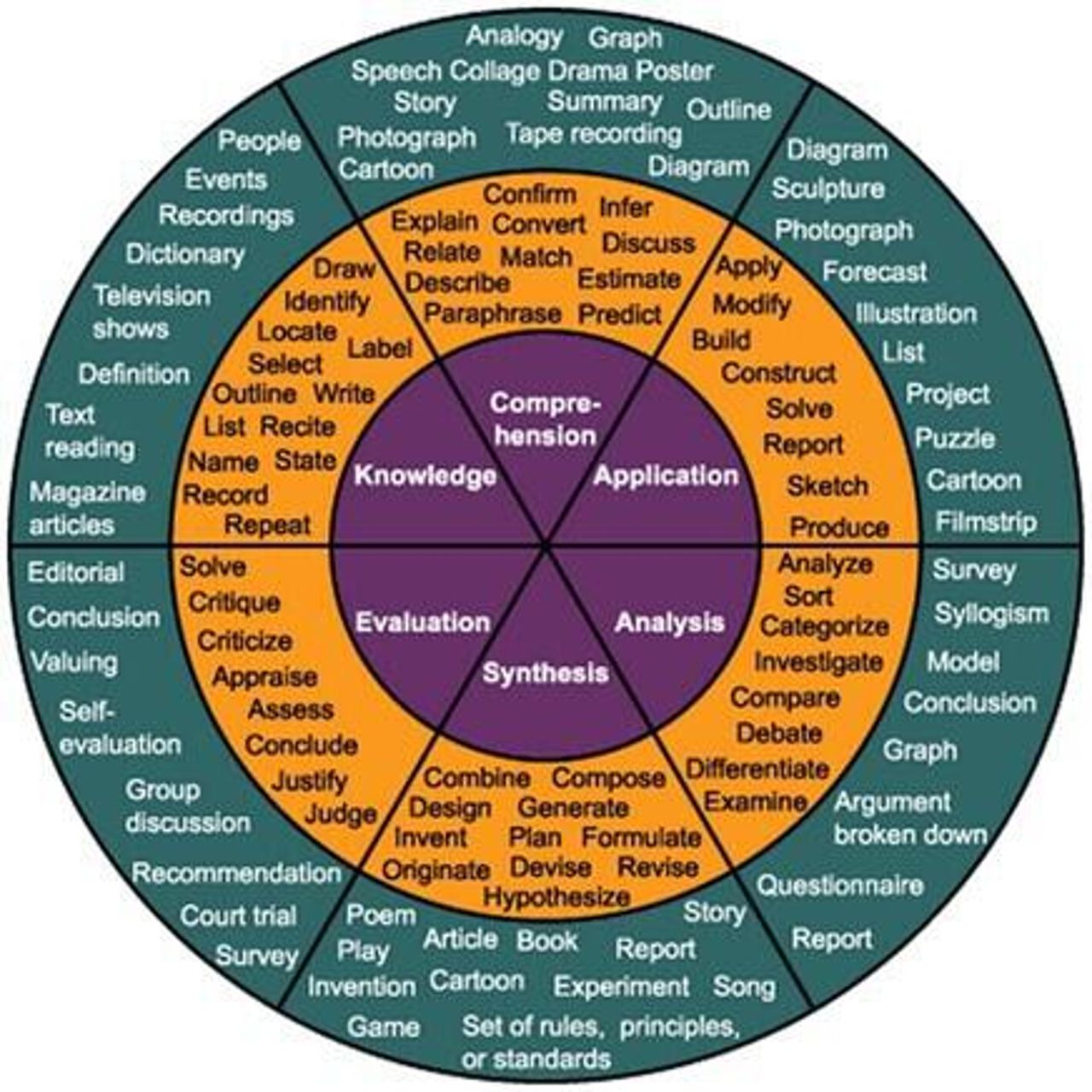
The research group developed the initial curriculum draft by collating and combining previously published LOs from UK-based SEM specialty training curriculums and a previous paper exploring the LOs required for an ideal SEM Masters curriculum published in 2006.2 8 9 This approach was used to ensure no potential relevant LOs were omitted. The LOs taken from the pre-existing curricula were grouped into suitable themes by the research group using themes previously published. All LOs were reviewed by the research group and edited, if needed, using Bloom’s taxonomy wheel (figure 1) to make them suitable for postgraduate level.10
{kind=link}
Bloom’s taxonomy wheel. Level 1 is knowledge, level 6 is evaluation. Image used within rules of license (creative commons attribution—sharealike license). Taken from: https://www.wylio.com/credits/flickr/4100721032%23.
Procedure
The initial survey to express interest in joining the expert panel was made using Google Forms (Google). Demographic information was obtained through this form. For the Delphi itself, electronic surveys were created using Qualtrics software and a link to it was emailed to all eligible members of the expert panel.11 The participant information sheet was attached to the email, along with contact details of the research group. Consent was gained via a mandatory question given before starting the Delphi. The instructions clearly stated that experts should consider the curriculum to be relevant for doctors undertaking a Masters in SEM, not considering other professions that may also undertake a Masters in SEM.
Engagement from the expert panel is crucial for any Delphi study and the aim was for the response rate to not fall below 70%.12 Experts were given 12 days to complete each phase of the Delphi. Non-responders after 8 and 10 days received a system-generated reminder. Text reminders were also sent to the expert panel if no response had been received on day 11. Only experts that completed phase 1 of the Delphi were invited to participate in phase 2. The data were collected between October and November 2020.
Phase 1: review of the draft curriculum
During phase 1, panel members reviewed the curriculum and were asked to accept, reject or modify each item. Participants were given the option of providing an anonymous comment after each decision. The percentages of agreement for each LO were calculated and, along with all comments, were read through and discussed by the research group. The response to each LO was discussed regardless of the level of agreement from the expert panel. After the collected data were reviewed, the research group agreed to either accept, reject or alter each LO to create a second version of the proposed curriculum. LOs with levels of agreement above 75% with no comments were accepted. The research group reviewed all comments on LOs that had been accepted and the LOs were amended accordingly and included in phase 2. LOs with levels of agreement below 75% without comments were rejected. For those with comments, these were reviewed by the research group, and where it was felt appropriate a modified LO was added for further review in phase 2.
Phase 2: second review of proposed curriculum (accept or reject)
A link to the second version of the curriculum was sent to all expert panel members that completed phase 1. For this phase, they were only provided with the option to accept or reject each LO. As reported by Keeney et al, a consensus was defined by 75% agreement.13 Previous literature reports varied levels appropriate for consensus, ranging from 70% to 100%.6 There was an optional open comments box at the end of each theme for further comments. The LOs accepted outright after phase 1 and did not require further input were included for reference. Again, the percentage of agreement was calculated, the research group reviewed all comments and a consensus was reached to either accept or reject each LO. Phase 2 would be repeated until a final consensus on the syllabus was reached.
Results
The initial proposed curriculum
There were 136 LOs collated from prior SEM syllabi. The research group divided these across 11 distinct themes.
The expert panel
Of the 94 people interested in being on the expert panel, 48% (45/94) met the eligibility criteria. The reasons for non-eligibility included having worked as a doctor for less than 5 years (n=19), not holding an SEM Masters/Diploma/FFSEM/MFSEM (n=17) and not being based in the UK (n=13). The expert panel consisted of 20 SEM consultants, 4 orthopaedic consultants, 1 rheumatology consultant, 17 general practitioners, 11 SEM registrars and 14 doctors that did not specify their training or job role but did confirm that they had been a doctor for more than 5 years. All the 14 doctors that did not specify their training/job role had completed a SEM MSc or Diploma and 57% had been a doctor for 13 years or more. Twenty-one individuals on the expert panel (47%) had experience teaching SEM Masters and Diploma courses.
Phase 1
In phase 1 of the study there was a 100% (45/45) response rate from the expert panel. Fifty-two per cent (71/136) of the LOs were accepted without the need for alteration, and 44% (60/136) were altered. The reasons for alterations are given in table 1. Thirty LOs were altered for more than one reason. Regarding the alterations made to the Bloom taxonomy level, 44% (n=15) were moved to a higher taxonomy level, 41% (n=14) were moved to a lower taxonomy level and for the final 15% (n=5) the wording was altered but the LO was kept within the same taxonomy level.
The reasons for alterations to LOs after phase 1
Five LOs (4%) were rejected and all were removed due to being deemed too high level for postgraduate SEM Masters. The objectives removed for being too high level are given in table 2, alongside comments given by the expert panel that contributed to the research group deciding on their removal. The first two LOs listed in table 2 regarding developing, leading and delivering exercise medicine services and MSK services received an agreement of 78% and 80%, respectively. Despite being above the approval threshold, the research group discussed these objectives at length, taking on board comments given by the expert panel, and determined these LOs were too high a level for a Masters level.
The LOs removed after phase 1 and comments given by the expert panel which contributed to justifying the removal of the LO
On reviewing the comments given by the expert panel, the research team added the following two LOs to the proposed curriculum:
Discuss a range of common ethical issues in a team sport environment (added to ‘sports team and event management’ subtheme)
Recognise the key medico-legal requirements and considerations in team medicine (added to ‘sports team and event management’ subtheme).
These were both added due to comments made by members of the expert panel at the end of the survey when asked if they had any final thoughts. The first was added due to a participant stating: ‘I would also add a section on Ethics and how this may impact the SEM physician’ (participant 31). The second was added due to a member of the expert panel stating: ‘Medico-legal issues in sports’ (participant 18). On discussing these within the research group the value of both comments were noted, and it was therefore deemed important to add related LOs.
Phase 2
Of the 45 that completed phase 1, 78% (35/45) of these individuals also completed phase 2. All LOs (100%) were accepted in phase 2 of the study, with all objectives achieving over 85% agreement. No alterations were made to any LOs. Therefore, no further phases were required. The final curriculum consisted of 11 subthemes (outlined in table 3) and 133 LOs. The full version of the final curriculum can be found in the online supplemental information.
Supplemental material
The finalised subthemes and number of learning objectives within each subtheme
Discussion
Summary of findings
An expert panel of 45 (100% of those eligible) completed phase 1 of this modified Delphi study, with 35 also completing phase 2 (78% retention rate). One hundred and thirty-six LOs were reviewed, with five removed during phase 1 after being deemed too high level for an SEM Masters degree. Two additional LOs were added, resulting in a final curriculum of 133 LOs, all of which were accepted by the expert panel during phase 2.
The importance of a standardised SEM Masters curriculum for doctors
Obtaining a high-quality and relevant education in SEM should be a critical goal for all physicians working in SEM.14 Although there is no specific data on this, anecdotally, the research group is aware that a large proportion of doctors working in the field of Sport and Exercise Medicine are not SEM consultants or on SEM specialty training programmes. For this group, their SEM knowledge and experience will be heavily influenced through the completion of an SEM Masters. It is reasonable to assume physicians will want their SEM Masters to be as relevant as possible to being an SEM physician, particularly given the cost and time-commitment of undertaking a Masters degree.
As a relatively new specialty SEM is continuing to find its place within the UK healthcare system; many fellow healthcare professionals have limited knowledge of the specialty and the skills SEM physicians possess.15 16 As a specialty we need to demonstrate we can stand alongside conventional specialties by being prepared to methodically examine our practice, ensure physicians practising within SEM are sufficiently capable and ensure they are working at a high level consistent throughout the UK.17 It is becoming increasingly common for SEM posts to include having an SEM Masters in their desirable or essential job criteria. The need to standardise SEM Masters curricula is therefore becoming increasingly important. It will be beneficial to the professionalism of the specialty to ensure individuals working in SEM posts that require an SEM Masters possess similar, consistent skills and knowledge.
Aspects too specialist for SEM Masters level
The expert panel rejected the practical LOs around performing ultrasound, joint and soft tissue injections and compartment pressure testing, with comments implying that they are too high level for SEM Masters courses. Ultrasound imaging is increasingly used in SEM to diagnose and monitor injuries; diagnostic ultrasound has previously been described as the ‘sports physicians stethoscope’.18 A 2017 International Consensus statement outlining a generic syllabus for SEM specialty training includes an ‘advanced skill’ of ‘targeted ultrasound examination of a peripheral musculoskeletal problem’.9 How best to provide ultrasound training to SEM clinicians, or a consensus decision as to whether it is needed, remains a controversial issue.18 The research group anecdotally acknowledges that many SEM clinicians choose to self-fund ultrasound training courses and equipment. The findings of this study indicate that ultrasound training should not be included in SEM Masters’ teaching.
LOs focused on developing and delivering exercise medicine services and musculoskeletal services were also not deemed appropriate to include in this curriculum, with several expert panel members commenting on issues with SEM Masters including these LOs. The research group discussed these objectives at length and deemed that these objectives would be more suitable for SEM consultant level or specialist SEM trainees. FSEM have created resources to aid SEM doctors in setting up SEM clinics and services, such as ‘Sport and Exercise Medicine: A Fresh Approach in Practice’ published in 2014.19 Interestingly, the 2017 International Consensus syllabus for SEM specialist training does not include learning how to set up an SEM service, nor does the most recent UK SEM specialist training programme curriculum.8 9 With increasing interest in how SEM can best be integrated into the NHS given the benefits SEM services can provide, it would be of great interest for further research be done to determine how the SEM specialty can most effectively increase the number of SEM services offered in the UK.3
Catering to all SEM Masters students
Doctors at any stage in training can undertake a Masters in SEM, and doctors at different stages in training may require different outcomes from a Masters course. It is also important to acknowledge that other healthcare professionals undertake an SEM Masters degree, such as physiotherapists, osteopaths and sports therapists. While there will be overlap, the outcomes these professionals wish to achieve from an SEM Masters are likely to be different to the LOs for doctors. Future research may consider exploring an appropriate SEM Masters curriculum for other healthcare professionals; it would be interesting to compare and contrast these with this curriculum.
Strengths
A modified Delphi was conducted thoroughly, following the appropriate methodology.4 The expert panel consisted of highly qualified individuals from relevant professional backgrounds. A high level of engagement and response rate was achieved. Many, often detailed, comments were received from expert panel members to justify responses. The research group contains individuals with a wide range in level of training. A high level of acceptance was achieved for each of the LOs included in the final curriculum. As no repeats to phase 1 or phase 2 were required, there were only two rounds of the Delphi before the finalised curriculum being created. Less than three rounds are recommended to reduce participation fatigue.13 20 21
Limitations
Although demographic data was removed, due to the nature of the questions asked to deem eligibility criteria, the research group may have been able to deduce who expert panel members were, resulting in bias. In addition, despite Masters degrees being primarily academic degrees, the only mention of research in the final proposed curriculum is in one LO listing research as a skill commonly used in practice by SEM physicians that the learner should be able to demonstrate. This is likely due to vocational-based curriculums being used to create the initial proposed list of LOs developed by the research group. It may be appropriate for educators creating curricula for SEM Masters to consider including additional research-related LOs. Given the nature of a Delphi study, the study is limited by the research group members and expert panel. The study methodology is by design opinion-based and open to researcher and participant bias. In addition, it would have been beneficial to know the specific training/job role of the 14 doctors on the expert panel that did not provide this information. However, all of these doctors had an MSc or Diploma in SEM and had all been a doctor for 5 years or more, with the majority having been a doctor for over 10 years.
Conclusion
The findings of this study will better inform educators involved in developing SEM Masters curricula, and inform students as to what they should look for when considering undertaking a Masters in SEM. This consensus curriculum is an important step in the standardisation of postgraduate SEM education. The next step will be to ascertain views of the finalised consensus curriculum from individuals involved in delivering, teaching and examining SEM masters content in the UK.
Data availability statement
No data are available. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was granted by Hull York Medical School.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @krmarino1
Contributors DV conceived the idea of creating a piece of work on this topic. DV, AI and KRM were involved in data collection. DV, KRM, PB, CN, AP and GF sat on the research group and analysed the data. All authors contributed to the critical revision and approval of the final editorial. DV is the guarantor of this study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.