Article Text

Abstract
Objective To conduct a scoping review providing an overview of the health conditions occuring in retired male and female professional footballers, with an emphasis on musculoskeletal, mental, neurocognitive, cardiovascular and reproductive health conditions.
Methods In January 2022, a comprehensive systematic literature search in three databases (MEDLINE via PubMed, SPORTDiscus via EBSCOhost and EMBASE) was conducted for common health conditions among retired male and female professional footballers. Primary research studies (full text available online) which described the incidence or prevalence of a health condition (musculoskeletal, mental, neurocognitive, cardiovascular, reproductive) among retired male and female professional footballers were included for review. Case reports, qualitative research and grey literature were omitted.
Results In total, 917 eligible articles were identified from the databases, with 41 meeting the eligibility criteria. Osteoarthritis of the hip, knee and ankle were found to be common among retired professional footballers. Mental health symptoms (eg, anxiety, depression) are experienced by retired male and female professional footballers. The incidence of neurocognitive disease appears to be higher among retired male professional footballers than among matched controls. There is very limited evidence examining the presence of health conditions in retired female professional footballers.
Conclusion Osteoarthritis of the lower limb, musculoskeletal pain and mental health symptoms are common among retired professional footballers. Knowledge about the occurrence and timing of musculoskeletal, mental health and neurocognitive conditions among retired professional footballers can be used by a wide range of stakeholders to proactively intervene during and after a player’s career to mitigate risk.
- Football
- Osteoarthritis
- Review
- Mental
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known
Elite athletes overall seem to have better health outcomes than the general population.
Musculoskeletal conditions, such as osteoarthritis, appear to be prevalent among retired professional footballers.
Professional footballers may be at heightened risk of mental health issues during the transition from playing to retirement.
What are the new findings
Osteoarthritis of the lower limb, musculoskeletal pain and mental health symptoms are common among retired professional footballers.
There are very limited data available to understand the health issues encountered by retired female professional footballers.
Knowledge about the prevalence of musculoskeletal, mental health and neurocognitive conditions among retired professional footballers can be used by a wide range of stakeholders to proactively intervene during and after a player’s career to mitigate risk.
Introduction
Elite athletes appear to have better long-term health outcomes than the general population.1 2 This is likely to apply to professional footballers, although the literature has highlighted specific health conditions which may be prevalent among retired professional footballers, including musculoskeletal,3–7 mental8–13 and neurodegenerative health conditions.14–16
Professional football is known for its high injury rate compared with other sports, with an injury rate of about 1.3 injuries per player per season.17 The management of these injuries may occasionally require surgical intervention, and this, along with the cumulative effect of repetitive microtrauma and considerable joint demands, compounds the risk of complications for professional footballers in retirement, especially early-onset osteoarthritis (OA).3 A diagnosis of OA has implications for quality of life, function and broader health (eg, cardiovascular health) in later life.18 19 Injury is also a stressor which may predispose a footballer to mental health symptoms, alongside decreased performance, deselection or negative media attention.20 The onset of mental health symptoms appears to be most apparent during the transition to retirement and this may be linked to a loss of identity and the adoption of negative lifestyle behaviours (eg, alcohol excess).9 Retirement is likely to lead to reduced physical activity levels by former professional footballers and this, coupled with the aforementioned issues, may have implications for cardiovascular health.21
In recent years, significant attention has been given to the relationship between contact sport, concussion and subsequent neurodegenerative disease.22–24 With specific reference to professional football, the repetitive subconcussive effects of ‘heading’ is feared to place players at greater risk of conditions such as dementia in later life, although the evidence for this is limited.25 Initiatives to improve the management of concussion in football are underpinned by a desire to protect player welfare long-term.26
The increasing participation of women in sport, especially professional football, has seen a much needed emphasis placed on understanding the influence of sex hormones and the menstrual cycle in female athlete health and performance.27 Nevertheless, the research appears limited with respect to understanding the long-term reproductive health status of professional female footballers.28
Professional football is a highly rewarding career in many instances, and the long-term health benefits of the associated physical activity is undisputed. There is a growing evidence base examining long-term health issues in retired professional footballers, and this has focused on musculoskeletal and mental health issues—although neurodegenerative, cardiovascular and reproductive health may be avenues worth understanding further. Through better understanding, the potential influence of a career in professional football on players’ long-term health, a wide range of stakeholders may be better informed to intervene proactively during and after a player’s career in order to mitigate the risk of these conditions—without detracting from the spectacle of the sport. No scoping review, to our knowledge, has examined the extent of health conditions commonly afflicting professional footballers on retirement. A scoping review of this nature may guide the work of policymakers and other stakeholders, and inform research policy. Therefore, the aim of this study was to conduct a scoping review providing an overview of the health conditions occurring in retired male and female professional footballers, with an emphasis on musculoskeletal, mental, neurocognitive, cardiovascular and reproductive health conditions.
Methods
Search strategy
The protocol for this scoping review was established by combining the guidelines of the PRISMA Extension for Scoping Reviews (PRISMA—ScR) with a method outlined by Peters et al.29 30 The final protocol was not published in advance but can be requested from the corresponding author.
In January 2022, a systematic search was carried out in the databases MEDLINE (via PubMed), SPORTDiscus (via EBSCOhost) and EMBASE. Search strategies were tailored according to the database being examined. The keywords (and synonyms) common to both databases were ‘football/soccer’, ‘retired’ and ‘health conditions’. For each category of health conditions examined, the keywords searched in both databases consisted of ‘musculoskeletal system’, ‘cardiovascular system’, ‘psychological disorders’, ‘neurocognitive disorders’ and ‘reproductive system’. For MEDLINE, the MeSH terms of the different keywords were used where suitable. For synonyms and key words in both databases, the title and/or abstract rather than text word to ensure that the search terms returned were the primary focus of the article. The Boolean command ‘OR’ was used in between synonyms and in between the different categories of health conditions. The Boolean command ‘AND’ was used to combine the keywords (and synonyms) with each other. A more detailed overview of the search strategies used for MEDLINE, SPORTDiscus and EMBASE is outlined in the online supplemental appendix of the article.
Supplemental material
Inclusion criteria
The following inclusion criteria were defined:
Primary research studies which included prospective and retrospective studies, cross-sectional studies and case-control studies which aim to describe the prevalence of health conditions in a given population.
Studies published in peer-reviewed journals whose full-text was available online.
Studies written in English, French or Dutch.
Retired professional male and/or professional female football players included in the study population.
Studies which described the incidence or prevalence of health conditions related to the health categories of interest, that is, musculoskeletal, cardiovascular, neurocognitive, psychological, reproductive.
The following exclusion criteria were defined:
Case reports and qualitative research.
Grey literature, including conference proceedings (eg, poster presentations), annual reports, dissertations, unpublished and ongoing trials.
Duplicate articles returned in both searches were removed and the criteria stated above applied to the eligible articles. Articles were initially included based on the information detailed in the title and abstract and subsequent retrieval of the full text to confirm the basis for their inclusion. Two independent reviewers carried out this process. In circumstances where there was discordance, consensus was sought through the input of a third reviewer. Finally, reference lists for each of the studies included were assessed to ensure no relevant articles were omitted. Forward and backward citation tracking provided further reassurance that all of the relevant articles were included in the review.
Data-charting
A data-charting form was created by the research team in order to display the key data to extract from the selected articles. Topics that were included in the form were: article information (author, year of publication, country of origin), purpose of the study, demographics of the study population, study design, category of health condition under study (cardiovascular, musculoskeletal, neurocognitive, psychological, reproductive), assessment method of the health condition under study and the incidence and/or prevalence of the health condition discussed. The data extraction was performed by two of the aforementioned individual reviewers—in circumstances where there was differing data submitted between reviewers, this was resolved by the contribution of a third reviewer.
Results
Search strategy
We identified a total of 917 eligible articles, a figure which was reduced to 97 once duplicates were removed and the inclusion criteria were applied to titles and abstracts. This number reduced further to 33 once the inclusion criteria were applied to the full texts of each article. Prior to full-text analysis, an estimated 15 articles were excluded as they were written in a language other than those specified in the inclusion criteria. Sixty-one articles were excluded as they did not study the target population, or they did not report on a relevant health condition. Two articles were excluded as they included a duplicate data set with another study already included. A further study was removed as it did not report the results related to the health outcome in question. The reference check and citation tracking of the included articles resulted in eight additional relevant studies. Ultimately, a total of 41 studies were included in our scoping review. Several studies included in the final review reported on health conditions from more than one of the relevant health categories. The flowchart in figure 1 displays the search procedure conducted in our study. Twenty-five of the included studies had incomplete data for data-charting. The authors for 16 of the 25 studies (ie, where a correspondence email address was provided) were contacted to obtain the additional data. Two authors replied, but neither of them could provide any information on the missing data for their respective studies.
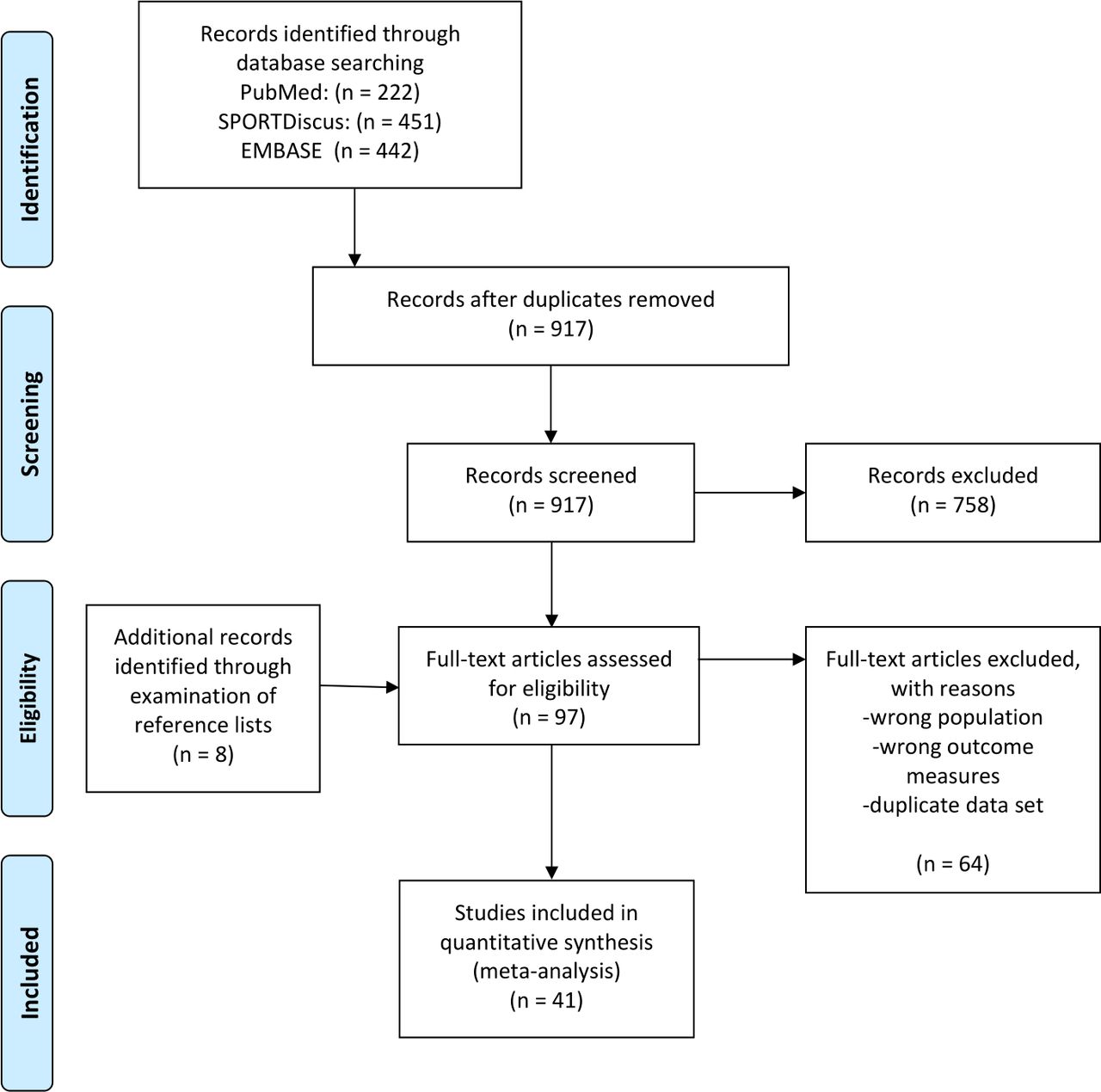
{kind=link}
PRISMA flow diagram for the scoping review.
Musculoskeletal health conditions
Twenty-eight articles retrieved from the search focused on outcomes pertaining to musculoskeletal health in retired professional footballers (all studies presenting prevalence rates). Twenty-six of these studies featured retired male professional footballers, and two of these examined health conditions in retired female professional footballers. The musculoskeletal conditions and presentations assessed included OA of various joints of the lower limb, joint pain, back pain and deformities of the lumbar and cervical spine. The key data from the 29 studies are outlined in table 1.
Musculoskeletal health conditions in former professional football players: data extraction from included studies
The prevalence rate of knee OA in retired male professional football players was found in 15 articles to range from 9% to 80%.3–5 31–42 Hip OA was reported on in 12 articles and the prevalence was found to range from 2% to 14% in the majority of studies, with one study showing a prevalence of hip OA as high as 50%.4 33 36 43 Five studies investigated the prevalence of ankle OA and found it ranged from 4% to 12%.4 33 44 45 Only one study found a higher prevalence of OA in the control group compared with the group of retired professional footballers.41 The method used to diagnose OA in various limb joints differed across studies, with some relying on clinical assessment, or imaging findings, or in some cases through self-reporting by study participants—or in some instances, a combination of methods.
Knee pain was reported by 37%–52% of retired male professional football players,4 5 and hip pain was found in 13% of this cohort.34 Radiological abnormalities in the lumbar spine, specifically osteophytosis, ranged from 24% to 51% with the highest prevalence of osteophytosis at level L4 and the lowest at level L2.46 Spinal issues were identified in one study, with 58% of retired players having reduced motion of the cervical spine, 21% of players having a history of cervical pain or stiffness and 33% of players having slight to moderate scoliosis.47
Two studies included retired female professional footballers and assessed the prevalence of knee OA and ankle OA, knee and back pain in this population. Knee OA ranged from 14% to 60%.7 48 Based on a questionnaire distributed to retired female professional footballers, 7% reported a diagnosis of ankle OA.48 The same study identified that 47% of the retired female professional players had knee problems, with 9% suffering with severe knee pain. Additionally, 47% of the same cohort had back issues of some description, with 9% experiencing severe back pain.
Mental health conditions
Mental health symptoms were assessed in 9 out of the 41 articles included in this scoping review (all but one study presenting prevalence rates). Only one of the nine articles examined issues exclusively in retired female footballers, although another study investigated the presence of psychological health conditions in retired male and female footballers but did not differentiate between gender when reporting the study results.13 The remainder of articles assessed related to retired male professional footballers. A summary of the key information from each article is outlined in table 2.
Mental health conditions in former professional football players: data extraction from included studies
Depression, anxiety, sleep disturbance and adverse lifestyle behaviours (eg, alcohol excess, poor nutrition) are among the mental health symptoms and conditions which were identified in retired male professional footballers. A likelihood of depression and anxiety was reported in 6% and 12%, respectively, in a paper by Fernandes et al which was similar to the levels of anxiety and depression seen in the general population.10 However, this cohort of retired male professional footballers reported lower health-related quality of life and higher analgesic usage. In another cohort of retired male professional footballers, depressive symptoms were experienced by a slightly higher percentage of study participants at 16%.49 Mixed depression and anxiety was assessed in three of the articles. The incidence of symptoms related to mixed depression/anxiety in these studies ranged from 26% to 39%.10 12 50 In one large-scale study in retired professional footballers, hospital admissions for common mental health disorders were lower than population controls, with no difference in suicide.12
Sleep disturbance was reported by 28% of former male professional footballers in two studies,12 51 although in another study performed in retired male professional footballers, they were found to have better sleep quality than control subjects.13 Adverse alcohol use was reported to be as prevalent as 32%, while poor nutrition choices seemed to be more commonly adopted by players on retirement.9
One study examined the presence of mental health issues exclusively in retired professional female footballers. In this demographic, it was found that 9% met the criteria for a diagnosis of clinical depression in the first 2 years of retirement, with 20% seeking help from a psychologist and 21% describing their mood as ‘low’.52 The study by Kilic et al also provided data on the population of retired female professional footballers but the results are combined with male data making it difficult to interpret these findings based on gender. Nevertheless, in this cohort, anxiety/depression was seen in 19% of retired professional footballers and alcohol misuse in 8%.13
Neurocognitive health conditions
Three studies retrieved from the search presented information exclusively about the occurrence of neurocognitive health conditions in retired male professional football players (all studies presenting prevalence rates). An additional study, referred to in the musculoskeletal health section above, found that 4% of retired professional footballers suffered with neuropsychological issues (eg, memory complaints) in later life.39 There were no studies found which detailed neurocognitive issues among retired female football players, while only one study explored the neurocognitive performance of retired elite female footballers.53 A summary of the key information from the included studies can be found in table 3.
Neurocognitive health conditions in former professional football players: data extraction from included studies
Neurocognitive health conditions that were found included neurodegenerative disease, dementia, mild cognitive impairment (MCI) and brain atrophy. In a study by Mackay et al, mortality from neurodegenerative disease was higher and mortality from other common diseases lower among retired professional soccer players than among matched controls. Dementia-related medications were prescribed more frequently to former players than to controls.14 More than 10% of the former players screened by Vann Jones et al were found to have possible MCI.15 One third of retired professional footballers in a Norwegian study found evidence of brain atrophy on neuroimaging, although it was not highlighted whether these findings were accompanied by clinical symptoms related to neurocognitive disease.16
Cardiovascular health conditions
None of the retrieved articles directly or exclusively explored the occurrence of cardiovascular health conditions in retired male or female professional football players. However, some studies indirectly examined issues related to cardiovascular health in retired professional footballers. Two studies highlighted that retired footballers were more likely than current footballers to adopt behaviours which may increase their risk of cardiovascular disease; for example, smoking, alcohol misuse and poor nutritional behaviours.9 50 Another study found no difference between risk of death from ischaemic heart disease between retired professional footballers and matched-controls.3 A lower reporting of diabetes and heart attacks among a cohort of retired professional footballers in the UK confirmed the potential long-term physical health benefits of professional football.10
Reproductive health conditions
No articles were retrieved covering the occurrence of reproductive health conditions in former professional male or female football players.
Discussion
The aim of this scoping review was to provide an overview of the health conditions occurring in retired male and female professional footballers, with an emphasis on musculoskeletal, mental, neurocognitive, cardiovascular and reproductive health conditions. There was a high prevalence of OA of various lower limb joints among retired male professional footballers, with evidence of knee OA in up to 80% of this cohort, and one study suggesting the presence of hip OA in 50% of retired players. Knee and back pain were also commonly reported by retired male professional footballers. Knee OA was reported in up to 60% of retired female professional footballers. Mixed anxiety and depression was found to be as high as 39% in retired male professional footballers. The only study carried out exclusively in retired female professional footballers found that 9% met the criteria for a diagnosis of clinical depression within 2 years of retirement. Dementia was among the neurocognitive conditions found to be present in retired male professional footballers. Only one study investigated neurocognitive health conditions among retired female professional footballers. There were limited specific data on the presence of cardiovascular conditions among retired professional footballers, and no studies retrieved examined reproductive health conditions among retired professional footballers.
Perspective of the findings
This is the first scoping review of health conditions in retired professional footballers and as such comparisons are limited. The aim of this scoping review was not to compare health conditions among retired professional footballers with other populations and, as such, any comparisons are made with caution considering the unsuitability of the research question to address this. There is established evidence demonstrating that OA is associated with occupations that demand challenging and repetitive use of the knee joints.54 The findings of this scoping review support the notion that OA is more prevalent among retired professional footballers than the general population. Knee OA was present in up to 80% of retired professional footballers, while in comparison, 13% of women and 10% of men aged 60 years and older have symptomatic knee OA.55 It is reported that 18% of the general UK population have sought treatment for knee OA, and 8% have sought treatment for hip OA.56 The prevalence of knee OA (13%) among current professional footballers is significantly less than retired professional footballers.57
The incidence of depressive symptoms among retired male professional footballers was as high as 39%, while 9% of retired female professional footballers met the criteria for a diagnosis of clinical depression within 2 years of retirement. The estimated worldwide prevalence of depression is 4.5%, with up to 25% of adults estimated to experience an anxiety disorder at some point in their life.58 Mental health complaints appear slightly less prevalent among current professional footballers compared with retired players; 26% of active players demonstrate evidence of anxiety/depression.9
These findings indicate that musculoskeletal and mental health conditions are potentially more prevalent among retired professional footballers than age-matched controls and active footballers. The limited data on neurocognitive, reproductive and cardiovascular conditions make it challenging to draw detailed comparisons with other populations.
Gender bias
The comparative lack of female participants in the studies included in this scoping review reflects wider trends in sports medicine research where females are under-represented.59 60 There is increasing professionalism and interest in women’s football, and efforts should be made to better understand sex-specific issues experienced by retired female professional footballers.
Additional studies which focus on assessing the presence of OA in retired female professional footballers are required, and the impact this has on quality of life and other important health outcomes may be needed. No studies were identified which assessed the prevalence of hip OA in female athletes, and this may provide useful insight. It is likely that the type of frequency and timing of mental health symptoms faced by retired female professional footballers differs from that of males, and subsequently this may influence the approach to provision of mental health support for females during and after their careers. Only one study included in this scoping review explored mental health symptoms in retired professional female footballers, and the findings from this study warrant further investigation.
There is emerging evidence to suggest women are more at risk of concussion than men, and that current gender-neutral return to play guidelines may not sufficiently consider gender differences.61 Additionally, women are believed to be more at risk of neurocognitive disease than men.62 With this in mind, urgent studies are required to assess the risk of neurocognitive disease in retired female footballers and to improve the management of concussion in the Women’s game.
Last, there is a better understanding of the relationship between menstrual cycle and performance in female footballers.27 Our search could not identify any studies which examined the effects of a career in football on long-term reproductive health, and future studies of this nature may provide useful information which can improve the health of female footballers during and after their career.
Duty of care and after career consultation
Our scoping review does provide insights into health conditions encountered by retired professional footballers which may pave the way for interventions during and after a player’s career in order to mitigate risk. Through understanding the common health conditions encountered by professional footballers in retirement, we may be better placed to intervene proactively during and after their career. The specific interventions which may benefit retired footballers has yet to be established, although they may include initiatives such as improvements in the management of concussion, injury prevention programmes, workload monitoring and a better understanding of surgical options for injuries during a player’s career.63 A wide range of stakeholders have a duty to protect the long-term health of footballers, and this can likely be achieved without detracting from the spectacle of football.64
Plausible interventions for retired players after their careers may include lifestyle education (eg, for improved mental and cardiovascular health) or the GLA:D programme for OA.21 65 There are growing calls for footballers to undergo a formal process on retirement in order to identify current health issues, signpost them to available resources and mitigate risk against future disease.21 64 Recently, an after career consultation (ACC) was developed in order to empower the sustainable physical, mental and social health and the quality of life of retired professional footballers.21 The ACC focusses on (among other aspects) musculoskeletal health, mental health, cardiovascular health and neurocognitive health. This review has identified that mental health problems such as anxiety and depression are as common among retired footballers as in the general population. However, retired footballers may be more at risk of issues during the transition to retirement which suggest that the timing of the ACC may be important.50 52 Through proactive support and intervention, the effects of a high prevalence of OA and pain medication usage among retired professional footballers may be reduced. It would also provide an opportunity for retired footballers to discuss any concerns they may have with respect to their long-term neurocognitive health. The ACC has primarily been developed for retired male professional footballers, and this review has highlighted that despite the limited research into retired female professional footballers, a female-specific protocol is warranted.
Strengths and limitations
This is the first scoping review to investigate the common health conditions encountered by retired professional footballers. Studies were included from 16 different countries, which indicates the limited breadth of the available data. Socioeconomic and cultural factors are likely to influence health outcomes for retired professional footballers, and in this context, studies performed in retired professional footballers from a broader range of countries would deliver a more accurate impression of the health conditions experienced by retired professional footballers. This, in turn, may improve the specificity of the health guidance that retired professional footballers receive.
The health categories emphasised during this review were chosen in order to ensure the most frequent conditions associated with retired football players were captured, although it is not unreasonable to consider that other categories or subcategories may have been worth exploring (eg, problem gambling). Given the composition of the research team, it was decided that only studies written in English, Dutch or French would be included for analysis. The impact of such language exclusion, and the omission of grey literature, is that the number of potentially excluded but relevant publications is estimated, but not known.
Scoping reviews do not formally assess the methodological quality of individual studies, and the risk of bias was not appraised systematically in this review. The interpretation of studies and their significance was assessed according to the expertise of the authors for discussion. The impact of this approach is that caution should be exercised when interpreting the significance of the incidence and prevalence of the included studies, as their reported rates may not be truly reflective of health conditions among retired professional footballers. A high number of studies included in this review were cross-sectional in nature, which makes interpreting the temporal relationship between exposure and health outcomes difficult. The definition of ‘professional footballer’ may have differed between studies, and not all studies included key data such as duration of career and time since retirement. Additionally, there were little data provided on playing positions, nationalities, career earnings or ethnicity—all of which may have provided improved insight into the findings. Small sample sizes and poorly matched control groups in some studies may have introduced potential errors in interpretation.
Future research examining health conditions among retired male and female professional footballers should include relevant injury history, career duration, time since retirement, playing position as well as any socioeconomic factors which may confound the findings (eg, current occupational status). A consistent definition of ‘professional footballer’ in studies is also required, for example, a retired professional footballer is defined as an individual who is remunerated for devoting several hours in all/most days (exceeding the time allocated to other types of professional or leisure activities) to playing football, and in which they competed in the highest or second highest national league.
Conclusion
A career in professional football is likely to confer long-term health benefits associated with physical activity. This scoping review, the first of its kind, has highlighted that musculoskeletal and neurocognitive conditions are relatively prevalent among retired professional footballers. Additionally, mental health symptoms exist among retired professional footballers, and they may be more vulnerable during the transition to retirement. Very few studies exist exploring health outcomes in retired female professional footballers, and considering the rapid growth in participation and interest in women’s football, efforts should be made to understand long-term health outcomes for female footballers. A wide range of stakeholders have a duty to protect the long-term health of professional footballers during and after their career. Potential interventions during a player’s career may include injury prevention measures, improved concussion care, better surgical decision-making and workload monitoring.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @VGouttebarge
Contributors All coauthors contributed to this manuscript. KA developed the search strategy in conjunction with VG and SC. SC wrote the initial draft of the manuscript, with AM, KA, GK and VG all contributing to subsequent iterations. The final manuscript was agreed and approved by all authors prior to submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.