Article Text

Abstract
Objectives In the UK, the National Health Service long-term plan advocates exercise as a key component of clinical services, but there is no clearly defined workforce to deliver the plan. We aimed to provide an overview of current UK clinical exercise services, focusing on exercise staff job titles, roles and qualifications across cardiovascular, respiratory, stroke, falls and cancer services.
Methods Clinical exercise services were identified electronically between May 2020 and September 2020 using publicly available information from clinical commissioning groups, national health boards and published audit data. Data relating to staff job titles, roles, qualifications and exercise delivery were collected via electronic records and telephone/email contact with service providers.
Results Data were obtained for 731 of 890 eligible clinical services (216 cardiac, 162 respiratory, 129 stroke, 117 falls, 107 cancer). Cardiac rehabilitation services provided both clinical (phase III) and community (phase IV) exercise interventions delivered by physiotherapists, exercise physiologists (exercise specific BSc/MSc) and exercise instructors (vocationally qualified with or without BSc/MSc). Respiratory, stroke and falls services provided a clinical exercise intervention only, mostly delivered by physiotherapists and occupational therapists. Cancer services provided a community exercise service only, delivered by vocationally qualified exercise instructors. Job titles of ‘exercise physiologists’ (n=115) bore little alignment to their qualifications, with a large heterogeneity across services.
Conclusion In the UK, clinical exercise services job titles, roles and qualifications were inconsistent. Regulation of exercise job titles and roles is required to remove the current disparities in this area.
- exercise
- rehabilitation
- exercise rehabilitation
- exercise physiology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data are included in the article / supplementary material.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Clinical exercise services are available for cardiac, respiratory, stroke, falls and cancer patients in the UK.
What are the new findings
Inconsistent job titles, roles and qualification requirements are evident across clinical exercise services for cardiac, respiratory, stroke, falls and cancer in the UK.
Regulation of exercise job titles, roles and qualifications is required for consistent provision of exercise in clinical settings.
Background
Long-term chronic and complex medical conditions are the largest financial burden on public healthcare.1 In 2019 in the UK, 38% of the adult population had a long-term condition, with 50% of all General Practitioner (GP) consultations, 65% of outpatient visits, and 70% of inpatient bed days attributed to long-term conditions.2 Ageing exacerbates the healthcare burden, as ageing is associated with an accumulation of long-term conditions, which leads to a decline in physical function linked to physical inactivity.3 Furthermore, healthcare expenditures in the UK have traditionally increased more than inflation resulting in consistent budget deficits.4 There is, however, overwhelming evidence of the efficacy of targeted exercise interventions for the prevention and management of ageing long-term conditions.5–8 Thus, embedding exercise into clinical services in acute settings is essential for managing ageing and long-term conditions and reducing long-term healthcare utilisation.1 9
Exercise provision as part of clinical services for ageing and medical conditions is highly inconsistent and piecemeal, that is, it has emerged separately for different conditions. In the UK, education and exercise programmes are most common in cardiac rehabilitation. The British Association of Cardiovascular Prevention and Rehabilitation (BACPR) have been instrumental in promoting and attempting to standardise delivery of exercise provision for secondary prevention for cardiac patients.10 The National Institute for Health and Care Excellence identifies six stages of cardiac rehabilitation in the UK.11 These stages have recently replaced the more commonly recognised terminology (internationally and in the UK) of service ‘phases’.11 Stages 1–3 (phases I and II) focus on acute recovery from an event or procedure, eligible patient identification and referral to cardiac rehabilitation programmes within 24–72 hours of hospital discharge.11 The waiting times in the UK for integration into stage 4 (phase III) exercise rehabilitation varies but usually occurs within 21 days (non-surgical patients) or 33 days (surgical patients).12 Stage 4 (phase III) is frequently delivered in clinical settings, incorporating specialised exercise assessment, prescription and education sessions using a multi-disciplinary team for 6–12 weeks.12 On completion, patients are re-assessed and discharged for long-term management into stages 5–6 (phase IV) community-led exercise.11 Exercise provision at phases III and IV is delivered by staff with a minimum of the BACPR exercise instructor qualification, including physiotherapists, nurses and exercise instructors.13 This standardised exercise provision in the UK is consistent with its international peers (eg, Australia) and is acknowledged as covering the core components of clinical care, including assessment, exercise prescription, education, behaviour change support and evaluation.11 14 15 In contrast to this approach for cardiac patients, exercise services for patients with other conditions are less well defined in terms of structure and, importantly, with delivery by a range of individuals with varying qualifications and skills.12 16 Previous audits of condition-specific clinical exercise provision in the UK (eg, National Audit for Cardiac Rehabilitation,12 Sentinel Stroke National Audit Programme17) have not attempted to distinguish between exercise staff job titles, roles or qualifications, nor have these been compared across conditions. This is important to consider since long-term health conditions, especially in older individuals, rarely occur in isolation (ie, individuals have multi-morbidity).3 If the National Health Service (NHS) is to achieve its priority of providing standardised, effective and cost-efficient exercise services for long-term health conditions, a system-wide understanding of what is currently being offered, to whom and by whom is required.
Research studies from several countries have identified the need for specialist exercise staff within clinical settings.18–23 Indeed, in some countries (eg, Australia, USA and Canada), established routes exist for accreditation of tertiary qualified exercise specialists (eg, accredited exercise physiologists (AEP), certified clinical exercise physiologist and clinical exercise physiologist, respectively), who are recognised as allied health professionals with knowledge and skills to deliver exercise assessment, prescription, delivery, supervision and optimisation for individuals within specific scopes of practice that include ageing and long-term conditions.24 25 There is evidence from Australia that AEPs provide a substantial economic benefit which translates to an annual well-being gain of $11 847 per person and a benefit–cost ratio of 6:1 across cardiovascular disease.26 In addition, AEP specific services have increased physical fitness and improved physical well-being and mood.27 28 There is no such accredited exercise specialist in the UK, and there is minimal guidance on staff competencies or standardised education required to deliver quality assured exercise testing and programming for clinical populations. Consequently, UK clinical exercise services are diverse in terms of staff qualifications, expertise and training. In contrast to the situation in comparable countries, physiotherapists often undertake clinical exercise delivery in a dual-capacity rather than a specialised and accredited graduate exercise healthcare professional (physiologist).16 24 While, this could be viewed as a cost-effective approach, physiotherapists’ implementation and knowledge of exercise prescription and physical activity guidelines has previously come under scrutiny in other countries,29–31 with exercise physiologists recognised as the specialist healthcare professionals in this area.22 23
In the UK, no current best practice model for all long-term conditions exists for how services should be structured to achieve clinical exercise outcomes. Even if cardiac rehabilitation is viewed as best practice, this is not employed for other specialised services. In the example of cancer (a priority in the NHS long-term plan), a UK strategy founded on an evidence-based platform has been introduced utilising both pre/rehabilitation exercise interventions to help reduce the potentially negative side effects of treatment and to improve survival.32 33 In this case, an appropriately trained exercise workforce is essential in the exercise assessment, prescription, delivery, supervision and optimisation of physiological outcomes and behaviour change.34 A recent study identified that the exercise provision for long-term conditions (including cancer) has previously focused on exercise referral schemes (ERS).16 Such services rarely employ staff with the knowledge, skills and competencies of other health professionals within clinical settings.16 35 ERS were, however, designed for apparently healthy individuals with risk factors, and different skills and competencies might be required when delivering specialised clinical exercise services designed for those with long-term complex medical conditions. Therefore, a better understanding of the job titles, roles and qualifications of those delivering specialised clinical exercise services is required to provide a basis for comparison.36 This study aimed to collate delivery information across the five most prevalent clinical exercise services in the UK (cardiovascular, respiratory, stroke, falls and cancer), focusing on understanding staff job titles, roles and qualifications. A coherent understanding of extant service provision can inform recommendations for systematic and consistent exercise provision in clinical settings, a key priority in the NHS long-term plan.1
Method
Design
A quantitative, systematic mapping approach was used to review clinical exercise services across the UK for cardiac, respiratory, stroke, cancer and falls. The intention was to use ‘mapping’ to establish the relevant components of exercise services to create a virtual ‘picture’ of current provision in the UK and not to ‘map’ services in the geographical sense. This form of data collection presented an overview of information in a condensed format to enable comparison across services.36 Data collection occurred across two stages: (1) identification of eligible clinical services and the extraction of publicly available information; (2) follow-up telephone calls and emails with representatives from each service to clarify details not apparent in the online material (eg, service delivery protocols, job roles and staff competencies). Data were then extracted based on relevant items from the physical activity referral scheme taxonomy (PARS)37 (online supplemental appendix 1).
Supplemental material
Data collection
Data were collected between May and September 2020 and focused on ‘usual face-to-face’ service provision delivered before the March 2020 COVID-19 lockdown (after which face-to-face clinical exercise provision in the UK was temporarily paused, with ~50% of cardiac services moving to online delivery only38). All data were collected by one author (AC). Members of the research team (LEFG, HJ, PMW) independently reviewed a random sample of 5%–10% of the extracted data to ensure continuity and validity of methods. They completed monthly debriefing sessions to discuss the data collection.
Eligibility
Inclusion
A clinical care service that included physical activity or exercise, had a formalised referral process in place and specifically focused on the management of cardiac or respiratory conditions, stroke, cancer or falls prevention. This included but was not exclusive to:
Structured physical activity/exercise programmes.
Physical activity/exercise behaviour change consultations.
Referral to a third-party provider for physical activity/exercise prescription.
Exclusion
Services were excluded if no contact information could be found, or insufficient public domain information was available (incomplete data sets).
ERS that provided non-specific exercise or physical activity for multiple health conditions and risk factors were excluded.
Procedure
Stage 1: internet search
Location search
The first part of the search focused on identifying clinical services across trusts, health boards and commissioning groups, sourced via NHS websites. These were then broken down into individual trusts and then sites (eg, hospitals) for each of the 135 clinical commissioning groups in England, 14 regional NHS Scotland health boards, 7 local health boards and 3 NHS trusts which focus on Public Health Wales, and 5 health and social care boards across Northern Ireland. Individual services responsible for exercise provision were identified using the service specialism within each site. These services’ webpages and social media accounts were searched for information about clinical exercise provision for cardiac, respiratory, stroke, falls and cancer services (eg, job descriptions and personal specifications).
Condition-specific search
The second part of the internet search focused on clinical exercise services listed in the public domain, such as previous national audits across condition-specific services such as the National Audit for Cardiac Rehabilitation, Sentinel Stroke National Audit Programme, MacMillan ‘Move More’ programme and British Lung Foundation reports. Services were identified, and any available information was extracted. Duplication of services across these processes was removed.
Stage 2: follow-up contact
Services were contacted by telephone, email (to arrange a telephone call), or video conferencing by the first author (AC). On initial contact, service providers were asked to identify the most appropriate individual to provide operational information and pass on their contact details. These individuals were then contacted via telephone and, if no response was elicited, emails were sent (a minimum of two over a 4-week period). All staff contacted were contracted (full-time or part-time) or freelance (paid by the hour) capacity. Service representatives were given a verbal or written explanation of the study protocols with verbal consent for participation obtained before data collection. Services were advised that only information available in the public domain was requested during this process.
Data extraction
A data extraction framework using Microsoft Excel worksheets and based on the PARS taxonomy questionnaire37 was used to record information for each service. The PARS taxonomy is a newly validated, peer-reviewed tool for recording physical activity service information and was developed to promote standardised physical activity intervention classifications to improve policymakers’ interpretation and understanding of the evidence base.37 Although developed for generic physical activity interventions, the framework was used as a guide for the data extraction, providing specific headings in areas of interest. This included the following sections.
Level 1: classification of providers, settings and activities
Providers were coded as: the NHS (free health services within the UK), local authorities (local government services) and third-sector organisations (charities, voluntary or non-profit groups). Settings were coded as: clinical NHS (defined as a hospital site where exercise is undertaken in either internal rooms or attached buildings), community (eg, buildings that were in some cases NHS operated and not attached to a hospital or non-leisure centre buildings such as local community centres) and leisure centres (usually local authority operated). Activities were coded as either one-to-one or group-based exercise sessions.
Level 2: characteristics of staff qualifications and roles
Staff qualifications were coded as vocational (practical/work-orientated levels 1–4) and academic (BSc/MSc). Level 4 vocational qualifications (such as BACPR) are the highest levels obtainable in the fitness industry. They are usually a mixture of theory and practical based learning over a period of months specialising and focused on one scope of practice, for example, cardiac rehabilitation, falls, stroke, respiratory or cancer. Undergraduate academic qualifications are typically 3 years in duration with postgraduate a further year (full-time) and cover a broader scope of practice. Service structure data were coded based on cardiac rehabilitation definitions of phase III provision and referral onto phase IV. Functional assessment delivery was coded by job title.
Data analysis
Data were analysed for frequencies and percentages using the statistical analysis software package (V.26).
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Service identification
A total of 890 services were identified as eligible for inclusion, and complete data was obtained from 731 of these services (table 1). All of these services had structured exercise components. None had behaviour change consultations only.
Exercise provision services for cardiac, respiratory, stroke, falls and cancer in the UK
Level 1: classification
Services
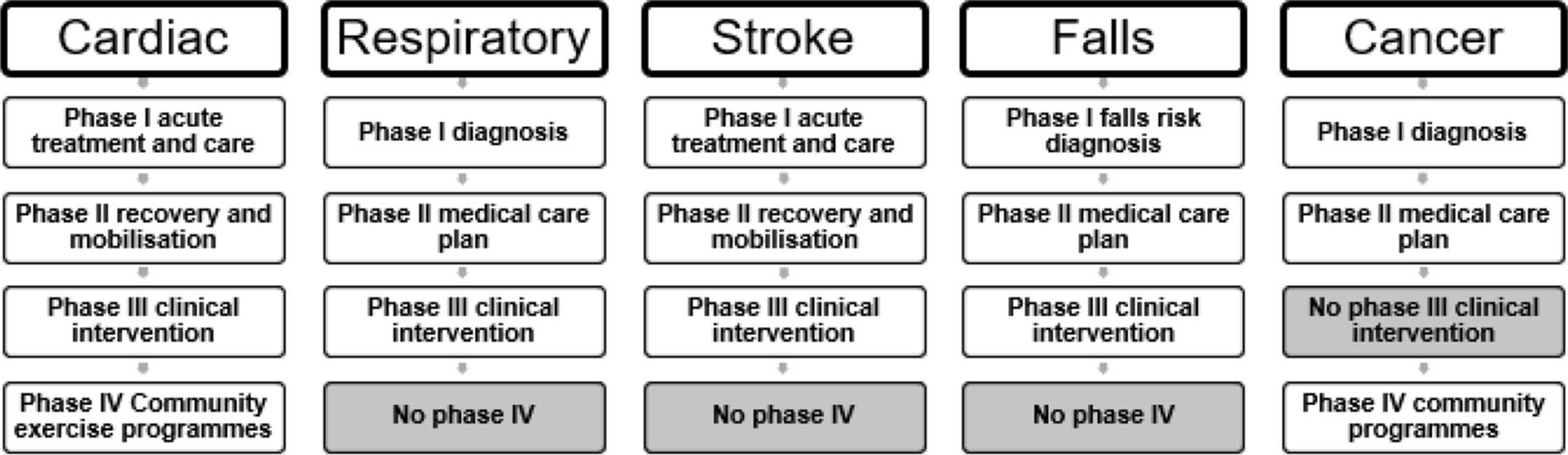
Cardiac services followed the most standardised approach with a 6-stage (4-phase) delivery model (figure 1). Using this model as a tool for comparison and keeping with the internationally recognised term ‘phases’, respiratory, stroke and falls services followed phases I–III but had no specific route to community exercise programmes (stage IV). Cancer services followed stages I and II and had no stage III but a route to community exercise programmes (phase IV).
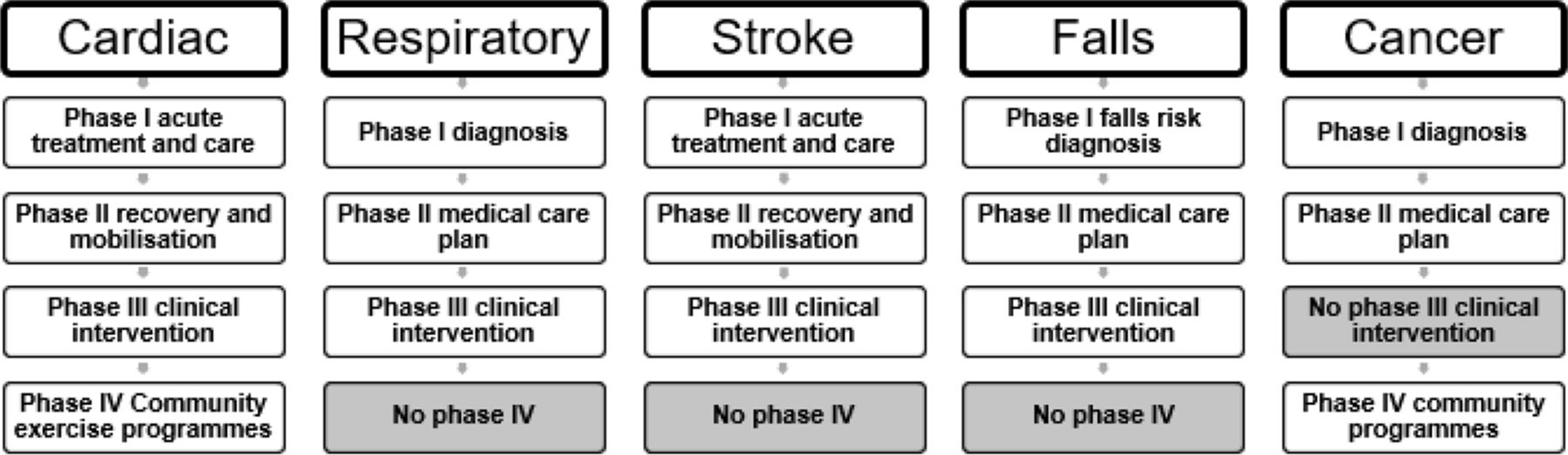
Clinical exercise pathways for cardiac, respiratory, stroke, falls and cancer services in the UK.
Provider, setting and activity type
The NHS were the principal service providers for cardiac (89%), respiratory (84%), stroke (95%) and falls (82%) exercise provision (table 2). Cancer exercise services were provided by NHS (30%), local government (44%) or third sector organisations (25%). NHS sites, either clinical or community, catered for most service provision, with cancer services being the exception. Disease-specific group sessions were most prevalent in cardiac (96%) and respiratory (100%). While some exercise services offered group sessions (51%) in falls, one-to-one sessions were more common in falls (89%) and stroke (100%) exercise provision. Cancer exercise provision included a large proportion of both disease-specific group (91%) and one-to-one sessions (76%).
Providers, settings and activity types available to patients across the cardiac, respiratory, stroke, falls and cancer clinical exercise services in the UK
Level 2: characteristics
Staff titles and roles in exercise delivery and functional assessment
Physiotherapists, either independently or in combination with other staff, including exercise physiologists, exercise instructors and occupational therapists, delivered exercise provision in cardiac, respiratory and falls services (table 3). In stroke, physiotherapists and occupational therapists (95%) were the primary deliverers of exercise provision. In cancer, exercise instructors were the primary deliverers of exercise provision on their own (79%). Exercise physiologists were employed by 46 (6%) services and exercise instructors by 257 (35%) services across all specialisms (see online supplemental tables 1–5). Physiotherapists completed the initial functional assessments on patient entry into most services. The exception was cancer services, with exercise instructors primarily completing the functional assessments (73%).
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Exercise delivery and functional assessment completion by job title across cardiac, respiratory, stroke, falls and cancer services in the UK
Staff qualifications for those delivering exercise
The qualifications of staff delivering the exercise components were identified independently of job title or whether they held salaried positions within the services (table 4). Some staff were recognised as having a stand-alone qualification (eg, BSc), while others held a combination of qualifications (eg, BSc and level 4 vocational exercise instructor). Staff qualified in physiotherapy (undergraduate or postgraduate), either individually or combined with other qualifications (eg, level 4 vocational exercise instructor), were widely employed across exercise provision for cardiac (37%), respiratory (67%) and falls (41%) services. Level 4 qualified exercise instructors without a tertiary degree were employed to deliver cancer exercise provision (88%) but were also prominent in cardiac (37%) and falls (29%) services. MSc qualified exercise physiologists were employed in cardiac (18%), respiratory (8%) and cancer (1%) services but not in falls and stroke exercise delivery. In 129 stroke services, exercise provision was delivered by physiotherapists and occupational therapists.
Exercise delivery staff qualifications across cardiac, respiratory, stroke, falls and cancer in the UK
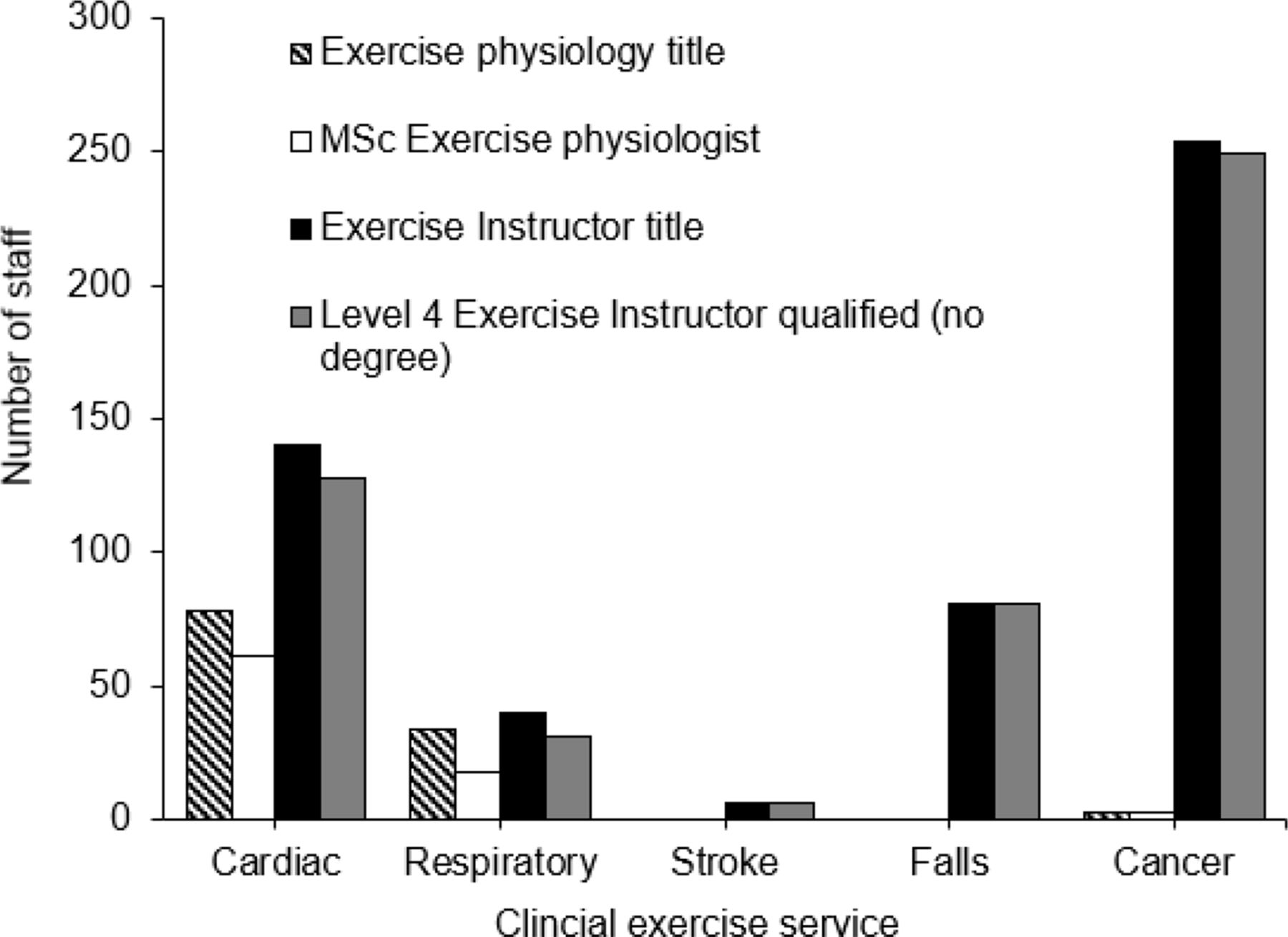
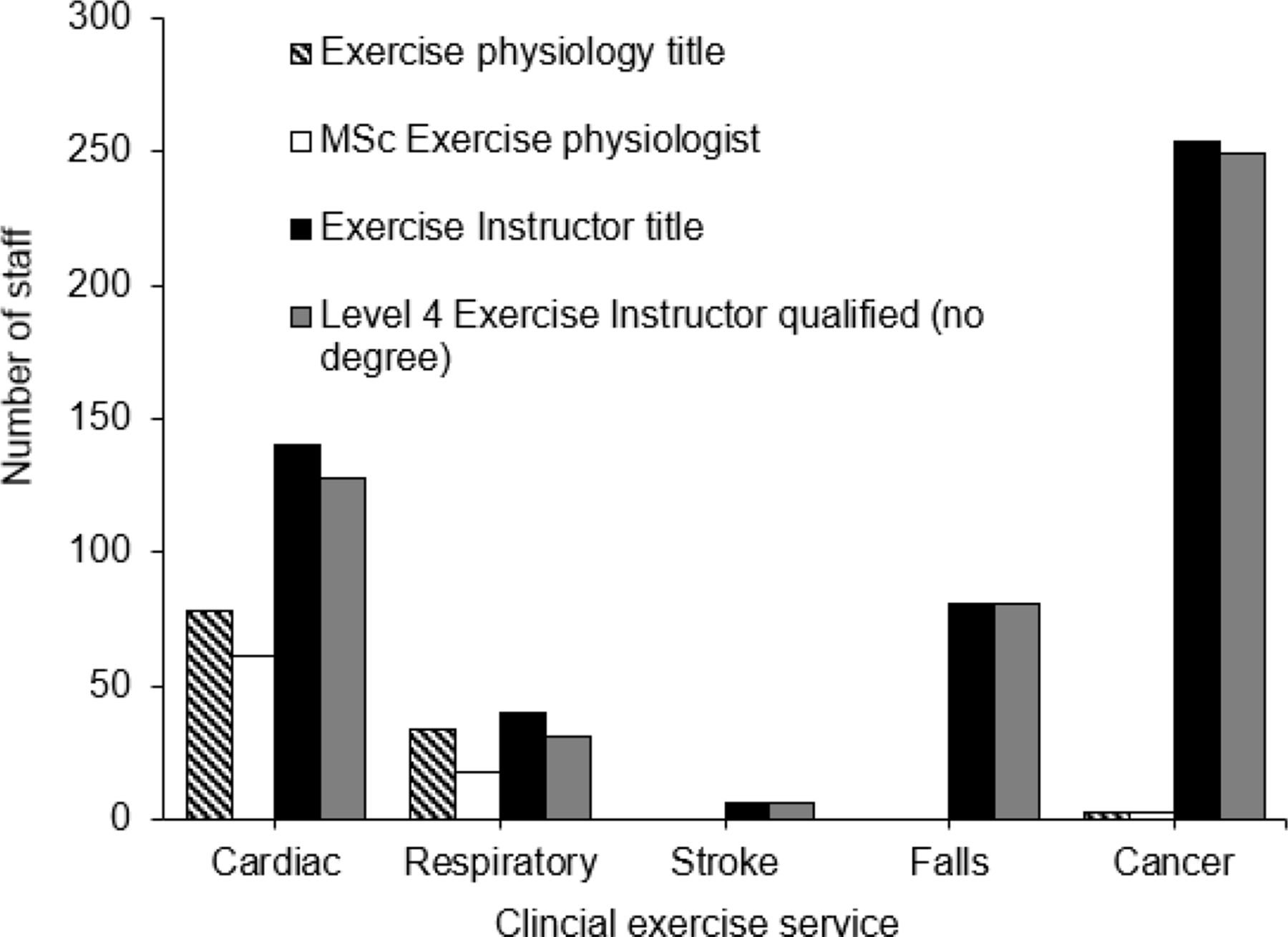
In cardiac, there were 78 exercise physiologists identified (figure 2), 61 of which were MSc qualified (table 4). These additional roles (n=17) were occupied based on undergraduate and level 4 vocational exercise instructor qualifications. Similarly, there were 34 exercise physiologists in respiratory services, with 18 qualified at the MSc level. Again, these remaining roles (n=16) were occupied by undergraduate and level 4 vocational exercise instructor qualified staff. In total, 115 exercise physiologist titles were found across all services, with 82 having an MSc qualification in exercise physiology.
{kind=link}
{kind=link}
A comparison between exercise physiologist and exercise instructor job titles and qualifications across cardiac, respiratory, stroke, falls and cancer services in the UK.
Discussion
The NHS long-term plan advocates exercise within clinical care services in the UK. There are, however, few recommendations regarding service structures for this to occur, or the staff requirements, qualifications, accreditation or the continued professional development needed to fulfil service objectives. This study aimed to provide a coherent understanding of current (pre-COVID-19) clinical exercise services across cardiac, respiratory, stroke, falls and cancer in the UK, focusing on understanding staff roles, qualifications and delivery settings. We found that clinical exercise services were not consistent in staff job titles, roles or qualifications across service specialisms. In all services, exercise was delivered by either physiotherapists, occupational therapists, exercise physiologists or exercise instructors. The exercise specific job titles for individuals not part of statutory regulation was not uniform across services and did not align with qualifications. Our data suggest that regulation of exercise job titles, roles and qualifications could help standardise exercise provision within clinical settings in the UK.
An 82% (n=731) coverage of identified services provided a substantial sample size to represent the sector. Cardiac had the greatest number of clinical services, followed by respiratory, with stroke, falls and cancer having lower levels of provision. A lack of standardisation, however, was identified across service models. Cardiac rehabilitation was the only service using both a phase III and phase IV exercise approach consistently, a model that has been adopted internationally as it contains the core components of clinical care.12 15 39 Each of the other services (respiratory, falls, stroke and cancer) lacked recognised phasing of exercise provision. Stroke and falls rehabilitation services appear to be built around the traditional clinical therapy provision. Notably, physiotherapists and occupational therapists provide functional movement and activity of daily living support (eg, getting dressed) in the hospital or in-home settings through early service discharge teams based on patient needs rather than exercise in a more traditional form. Although exercise-specific provision is recommended, stroke severity can impact the duration of sessions and activities undertaken and is difficult to categorise or standardise.40 41 Furthermore, stroke and falls services lacked phase IV provision, referring patients directly to ERS if/when available. Cancer services typically lacked clinical phase III exercise provision contrasting with recommendations outlined in the cancer prehabilitation guidance document, which advocates universal (anyone), targeted (those with late effects of disease or treatment) and specialist (those with complex needs) interventions provided by both clinical and community hub multi-disciplinary teams.42
We found staff roles and qualifications across services in the UK to be inconsistent. Exercise delivery staff within multi-disciplinary teams were primarily physiotherapists, although some services also used exercise physiologists and exercise instructors according to their job title. While other countries (Australia, USA, Canada and South Africa) have recognised that clinical exercise physiologists are at the forefront of exercise delivery,23 24 27 28 the UK does not currently recognise or regulate this profession. In other countries, the level of qualification for a clinical exercise physiologist is an accredited master degree in clinical exercise physiology. While the UK has master degrees labelled as including clinical exercise physiology, such degrees are not accredited or standardised for content, nor include competency-based assessment or clinical skills. Accordingly, our current data demonstrate that the number of exercise physiologists job titles where individuals had a relevant master degree (eg, MSc Clinical Exercise Physiology) were low (82). Moreover, qualification level bore little alignment to exercise physiologist job titles (n=115) with individuals also employed based on BSc degrees and vocational qualifications (n=33). Similarly, this level of qualification was present under the exercise instructor job title (n=59) rather than vocational qualifications alone. The current UK system does not stipulate a level of qualification for delivery of clinical exercise provision, with some employers accepting a level 4 exercise instructor qualification (eg, BACPR). This is likely a contributing reason for the discrepancies between job titles and qualifications. Previous research has highlighted concerns regarding competence and effectiveness of exercise provision in higher-risk and more complex conditions.18 19 43–45 We suggest that the UK consider formal regulation of clinical exercise physiologists akin to those of other countries. Such an undertaking would align the education and training with other allied health professionals, establish more consistent training of exercise specialists in clinical practice, and most importantly, standardise the exercise knowledge and skill levels of those working with patients with complex long-term conditions.45
The NHS generally provided services and operated in either clinical or community sites except for cancer pre/rehabilitation, which had a diverse range of support, including third-sector charity programmes.42 Interestingly, the 44% provision by local authorities appeared to be a legacy of cancer programmes (eg, Move More (macmillan.org.uk)), which were often delivered out of leisure centres (66% of services offered those venues) and staffed by exercise instructors with vocational qualifications. The location of cancer services could be a factor in the use of exercise instructors with accessibility and capacity linked to local exercise referral scheme availability. Exercise provision often focused on group activity (cardiac and respiratory) or one-to-one (stroke and falls), with cancer demonstrating a mixture of provision. Ultimately, a consistent level of provision and access should be available across services to ensure all patients are catered for.
Implications for practice
A standardised approach for all specialist services, possibly aligning with the staged (or four-phased) delivery model as seen in cardiac exercise services, requires exploration across all clinical exercise provisions. The current disparate structures in service models, staff roles and qualifications make it difficult to evaluate and compare both within and across services. Standardised services require staff roles to be outlined and job titles underpinned by appropriate levels of qualifications with the same level of regulation as other professions within the health and social care system. Such recognition could assist in providing assurances to the employers, clinical colleagues and the public that exercise healthcare professionals are appropriately qualified to deliver safe, effective and personalised exercise interventions for primary and secondary prevention across a spectrum of chronic diseases. Such changes would further explore service delivery effectiveness, patient outcomes and cost-effectiveness.
Strengths and limitations
A notable strength is the large sample size and the rigorous staged processes employed to gather information. Nevertheless, the descriptive data collected across five service models does not allow conclusions about these different models’ relative effectiveness or impact or any evident disparities. Furthermore, this study does not consider what works well or what needs improving to create a ‘best practice’ service model. It is also noteworthy to outline this information was obtained during the COVID-19 pandemic (May–September 2020) without an Open Science Framework registration, the information collected was reported based on the pre-COVID-19 service delivery, and we acknowledge some of the information collected might have changed due to staff re-deployment and halting of exercise services in response to the pandemic.
Conclusion
Clinical exercise provision is currently highly inconsistent and piecemeal in the UK. Staff job titles, roles, qualifications and service models differ between cardiac, respiratory, stroke, falls and cancer exercise services. The exercise specific job titles for individuals not part of statutory regulation were not uniform across services and did not align with qualifications. Future efforts should create a clear, consistent and regulated training route for staff across all specialist services in the UK if the NHS long-term plan is to be met. Additionally, regulation and integration of AEPs into clinical exercise services in the UK should be explored. Finally, research is needed into any unique services concerning staff constructs identified within this data to explore what works well and what could be improved within clinical exercise provision to assist in devising a best practice service model.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data are included in the article / supplementary material.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants. The purpose of this study was to define the current practice and was not aimed at producing generalisable academic knowledge. It was therefore defined as a service evaluation (“designed and conducted solely to define or judge current care”) and did not require research ethics approval. Ethical principles of consent, anonymity and data protection and privacy were adhered to throughout.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AC contributed to the design of the study, collected and analysed the data, and led the writing of the manuscript. HJ secured funding for the study. PMW, HJ and LEFG contributed to the study design and advised on data collection and analysis. All authors contributed to data interpretation and writing of the manuscript and approved the final version. AC is the guarantor.
Funding This research was funded by Research England International Investment Initiative funding (i-CARDIO).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.