Article Text

Abstract
Objectives Sport and Exercise Physicians represent a relatively new specialty focusing on exercise in complex diseases including musculoskeletal diseases. Our objective was to describe the characteristics, type and complexity of patient presentations, their management strategies and referral information in Australian practice.
Methods A cross-sectional study including a cohort of 11 senior Sport and Exercise Physicians in Australia studied all new patient consultations within an 8-week period. Data were analysed relating to presentation, referral source, follow-up referrals, and patient management strategies.
Results Data from 419 patients were recorded. The majority, 97% (n=406), had musculoskeletal conditions, 53% (n=222) had one or more associated comorbidities and 47% (n=195) had ongoing symptoms for >12 months. Most patients, 82% (n=355), were referred by general practitioners. Prior consultations included physiotherapy 72% (n=301) and orthopaedic 20% (n=85). A multidisciplinary network of referrals from Sport and Exercise Physicians was observed, including 210 referrals to 9 allied health specialities and 61 referrals to 17 medical specialities. Over 74% (n=311) of patients received exercise-based intervention as part of the treatment plan, including 57% (n=240) physician managed exercise interventions.
Conclusion Our work shines a light on the nature and complexity of the role of Sport and Exercise Physicians in an Australian practice context. Findings will assist in implementing measures to promote patient care at the community level in managing musculoskeletal conditions. Sport and exercise medicine stakeholders and government policy makers can use this information in developing appropriate programmes to support patients and create integrated sport and exercise medicine services for the community.
- sports & exercise medicine
- sports medicine
- physician
- health promotion
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known?
Little is known about how the role of Sport and Exercise Physicians in clinics can assist in implementing measures to provide better patient care in managing musculoskeletal conditions.
Stakeholders and government policy makers do not have sufficient information to influence changes in healthcare system and thereby develop appropriate programmes to support patient care and create integrated sport and exercise medicine services to the community.
What are the new findings?
Ninety-seven per cent of patients seen by Sport and Exercise Physicians have musculoskeletal conditions with nearly half reporting symptoms for more than 12 months.
7/10 saw a physiotherapist and 2/10 saw an orthopaedic surgeon prior to consulting a Sport and Exercise Physician.
A multidisciplinary approach was detailed by Sport and Exercise Physicians, including 210 referrals to nine allied health specialities and 61 referrals to 17 medical specialities.
Over 74% of patients received exercise-based interventions as part of the treatment plan during the first consultation, and the majority include physician managed exercise interventions.
In addition to standard treatment measures, interventions specific for sports medicine practice were observed in broad areas of nutrition and weight management, orthotics and footwear, special tests (eg, PROM, CogSport, SCAT5), taping and bracing, ergonomics, lifestyle modification and mental health
Introduction
Sport and exercise medicine is a relatively new medical specialty globally and is established as an integral component of the health system.1 2 Sport and Exercise Physicians are specialist doctors whose scope of practice focuses on protecting and promoting the health of individuals and communities.3 4 The Australasian College of Sport and Exercise Physicians (ACSEP) is the professional body representing Sport and Exercise Physicians and trainees since 1985. Currently, there are more than 150 Sport and Exercise Physicians practicing in sport and exercise medicine clinics across Australia and New Zealand.5
At the elite sports level, the physicians’ role is to look after the health and well-being of athletes.3 However, athletes are only one part of practice. Sport and Exercise Physicians play an equally important role in protecting the health and well-being of the community.4 In clinics, the patients include active populations, in particular middle and older age groups with a variety of acute and chronic musculoskeletal conditions with associated comorbidities. At the community level, the Sport and Exercise Physicians role expands to lead and promote safe participation in sport and exercise at all levels, and to work towards incorporating lifestyle intervention programmes into the daily lives of patients focusing on preventing and treating chronic and non-communicable diseases (NCDs).6
Musculoskeletal conditions contribute to a large proportion of injury and illness burden, and are reported to have the fourth greatest impact on the health of the world’s population, accounting for 6.8% of the total disease burden.7 8 In Australia, this is the leading contributor to total disability burden (27.4%), and is second only to cancer.9 Most are either persistent or recurrent in nature, and associated pain and disability can significantly affect patient’s activities of daily living, sleep, mental health, ability to work and impact quality of life.10 Among athletic populations, injuries and illnesses can have negative socioeconomic consequence to the patients, their families and to society.11 In Australia and New Zealand, sports and physical activities are a core part of the cultural lifestyle that is enjoyed by participants of all ages and abilities in the community. The prescription of exercise has been demonstrated to be beneficial in all nine of the National Health Priority Areas (cancer control, cardiovascular health, injury prevention, mental health, diabetes mellitus, asthma, arthritis and musculoskeletal conditions, obesity and dementia).12 In this context, the role and expertise of Sport and Exercise Physicians is increasingly important, at both elite and community levels.13
An accurate profile of the patient load undertaken by Sport and Exercise Physicians, particularly the patient characteristics and conditions seen, and the roles and services provided is important to optimise better patient care. Furthermore, a good knowledge of patient referral systems in the current sport and exercise medicine network is also useful in planning workforce capability. This is the first study to objectively assess Sport and Exercise Physicians services in the Australasian region or internationally. The primary aim of this study was to evaluate patient presentations to Sport and Exercise Physicians in Australia (specialists with ACSEP), examine the nature and complexity of new presentations, and analyse the physicians’ management strategies.
Method
Research design
This study is a cross-sectional descriptive cohort study involving prospective data collection from Sport and Exercise Physicians and their patients. Data gathered from Sport and Exercise Physicians were the primary component of this study, and supplementary data were gathered from patients.
Participants
Participants in this study included two groups: specialist Sport and Exercise Physicians and new patients seen during the study period. Inclusion criteria were physicians currently practicing in Australia with more than 10 years of clinical experience as a specialist. The chief investigator (JF) and ACSEP Fellows of the research team (DH) purposefully sampled to select physicians from a range of locations and practice settings.
Inclusion criteria for patients were new patient presentations to clinics seen during an 8-week period. All genders and adults (≥18 years) were included.
Both groups were provided with a plain language information sheet describing the aim and nature of the study, and their responsibility. Informed written consent was required prior to recruitment. Data collection occurred between September 2020 to January 2021.
Data collection
An online survey questionnaire was used to gather data from both groups. Physicians completed the questionnaire for each new patient presentation on the day of the consultation. Each physician completed the questionnaire for up to 50 new patients during an 8-week period between September 2020 and January 2021. The questionnaire included three parts designed to capture the nature and complexity of patient presentations and management strategies (online supplemental file 1). Part 1 collected clinical data such as primary symptoms and duration, medical history, previous investigation if any and previous treatment by other medical and allied health professionals. Part 2 included information related to referral sources and follow-up referrals involving other medical and allied health specialities. In part 3 physicians recorded their management plan including specific investigations, treatment, interventions and follow-up plan.
Supplemental material
Patients completed the EuroQol 5 Dimension 5 Level (EQ- 5D-5L) questionnaires on two occasions: before the first consultation (pretest) and 8 weeks after treatment (post-test).14 The EQ-5D-5L is a standardised descriptive instrument for measuring generic health status that has been widely used in population health surveys. It has five domains (mobility, self-care, usual activities, pain/discomfort and anxiety/depression) and patients indicate their health state using 5-point scale (no problems, slight problems, moderate problems, severe problems and extreme problems).
Data analysis
Descriptive statistical analyses were performed to examine the frequency of responses in the physician survey. A descriptive content analysis was used for summarising physician management including investigations, treatment and referrals to other healthcare providers. To evaluate the complexity of patient presentations, data were analysed and presented under the following domains: (a) duration of symptoms (chronicity), (b) previous diagnostic challenges, (c) number and type of previous medical and allied health consultations, (d) number and type of previous investigations and treatment.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Eleven physicians (mean age=58 years; mean clinical practice experience as a Sport and Exercise Physician=22.5 years) consented to take part in the study and completed a total of 419 surveys over the study period. The physicians represented four states of Australia (New South Wales=5; Victoria=3; Queensland=1; Tasmania=1) and one territory (Australia Capital Territory=1). Two physicians were based in regional and remote areas while nine were based in metropolitan areas.
Patient characteristics
Of the 419 patients seen, demographic data were available for 337 patients. The mean age of the patients was 45 years (range 14–87) with 50.4% females (n=170) and 49.6% males (n=167). Fifty-three per cent of the patients had other comorbidities at presentation. (online supplemental file 2). These include overweight/obesity (n=110, 26.3%), work-related concerns (including sport for professional athletes; n=51, 12.2%), psychological issues (n=65, 15.5%), smoking cessation (n=5, 1.2%), hypertension (n=26, 6.2%), sleep issues (n=18, 4.3%), travel requirements (n=9, 2.1%).
Supplemental material
Presentation characteristics
Nearly 97% of patients (n=406) presented to the physicians with a musculoskeletal-related condition. The most frequent presentations were for thoracic and/or lumbar spine (n=90, 21.5%) or knee-related conditions (n=81, 19.3%). Specific anatomical locations of these musculoskeletal presentations are presented in figure 1.
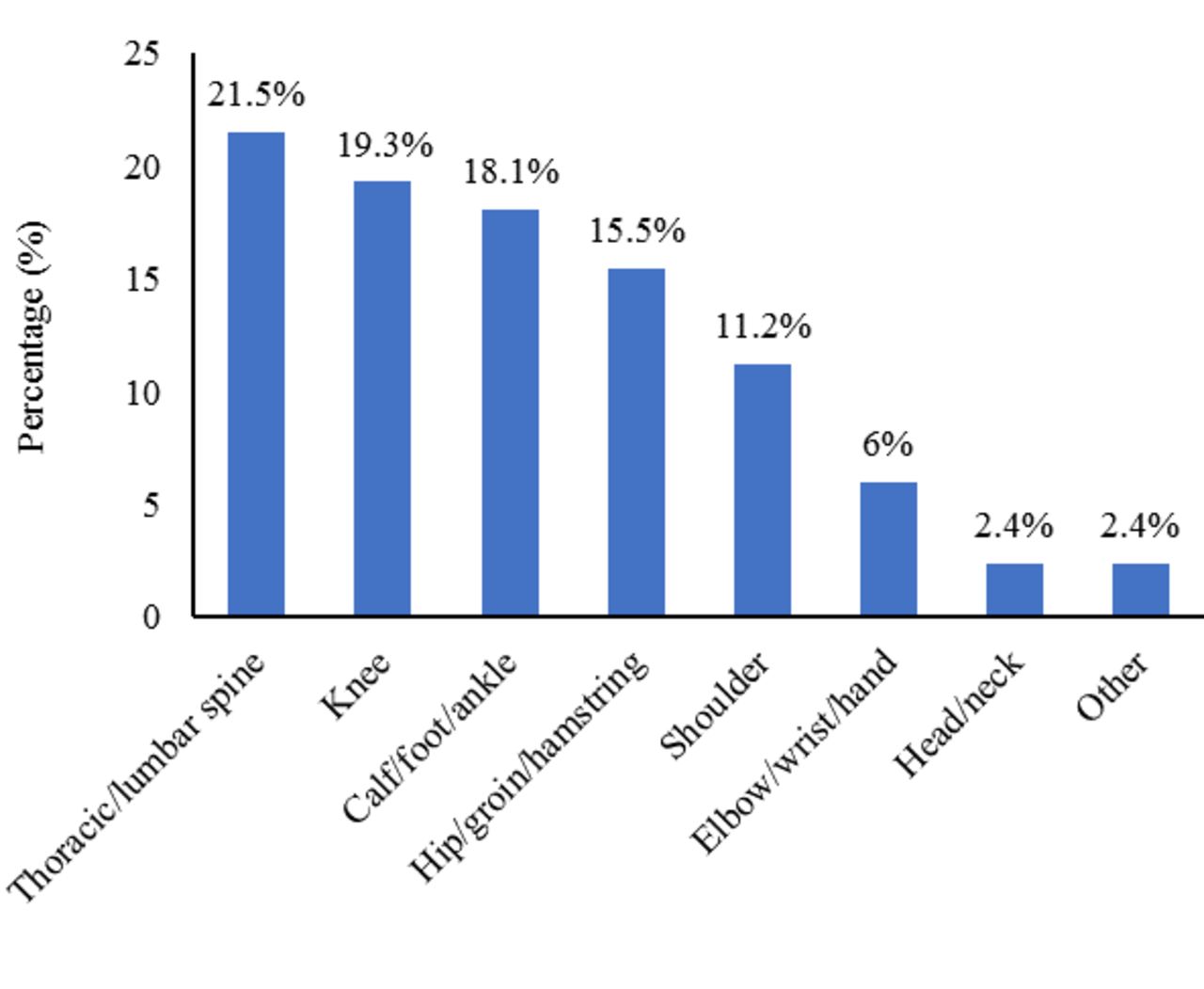
Presentations according to anatomical location of conditions.
Consultation characteristics
The length of consultations was greater than 30 min in 71% of consultations, (40% for 30–45 min, 23.9% for 45–60 min and 7.4% for >60 min). Only 0.5% (n=2) were short consultations of less than 15 min.
Nature and complexity of presentations
The nature and complexity of presentations were analysed as described in the methodology and presented in this section under four domains.
Duration (chronicity) of symptoms
Most patients had chronic symptoms, with nearly half of the patients (n=195; 46.5%) having symptoms for more than 12 months. Seventy (17%) patients had symptoms for 6–12 months, 74 (18%) had symptoms for 3–6 months and 80 (19%) had symptoms for less than 3 months.
Diagnostic challenges
Despite the generally chronic nature of their symptoms, 177 (42%) patients had no definitive diagnosis at the time of presentation. Of those who had a previous diagnosis (n=242), the diagnosis was revised in the majority (n=129; 53.3%) after the first consultation and modified for 22 others (9.1%).
Previous medical and allied health consultations
Figure 2 summarises previous consultations by other medical and allied health providers before presentation. Most patients (n=301; 71.8%) had been seen by a physiotherapist prior to their consultation. Most patients (n=329; 78.5%) had seen their general practitioner and also an orthopaedic surgeon (n=85, 20.3%).
Previous investigations and treatment

Overview of previous consultations by other medical and allied health providers.
Most patients (n=312; 74.5%) had undergone radiological investigation before their consultation. These included X-ray (n=159, 37.9%), MRI (n=168, 40.1%), CT (n=47, 11.2%), ultrasound (n=83, 19.8%) and dual-energy X-ray absorptiometry (n=4, 1.0%). Forty-six patients (11.0%) had laboratory/pathology investigations.
Most (n=239; 57%) patients were prescribed or directed to take medications by previous practitioners, primarily non-steroidal anti-inflammatory drugs (n=197; 47%). Further, 158 (37.7%) patients had other treatments such as injections (n=75, 47.5% of treatments), surgical interventions (n=13, 8.2% of treatments), shockwave therapy (n=8, 5.1% of treatments) and other (n=68, 43.0%). Prior treatments are presented in online supplemental file 3.
Supplemental material
Management led by Sport and Exercise Physicians: investigations and treatments.
The following section summarises the management by physicians during the first patient visit, including investigations and specific treatment strategies.
Investigations requested by the Sport and Exercise Physicians
Investigations requested by the Sport and Exercise Physicians during the first visit are summarised in table 1. Approximately half of the patients had radiological investigations performed (n=245; 58.5%).
Overview of investigations requested by Sport and Exercise Physicians
Treatment strategies delivered by the Sport and Exercise Physicians
Treatment strategies delivered by the Sport and Exercise Physicians are presented in figure 3, and include medications, other specific treatments and injection therapies. Non-steroidal anti-inflammatories were the most commonly prescribed medication (n=30; 7.2%). Less than 30% of patients were referred for diagnostic or therapeutic injections (n=120; 28.6%). Of these, corticosteroid injections were the most common (n=56), followed by platelet-rich plasma/autologous blood injections (n=20) and visco-supplement injections (n=18).

(A) Medications, (B) other specific treatments and (C) injection therapies referred by physicians. NSAID, non-steroidal anti-inflammatory drug; PRP, platelet-rich plasma.
Sport and Exercise Physicians delivered management strategies summarised in figure 4. At the initial consultation, 74.2% of patients (n=311) received an exercise-based intervention, 240 (57.3%) received physician managed exercise measures/interventions and 188 (44.9%) referral-based exercise interventions.
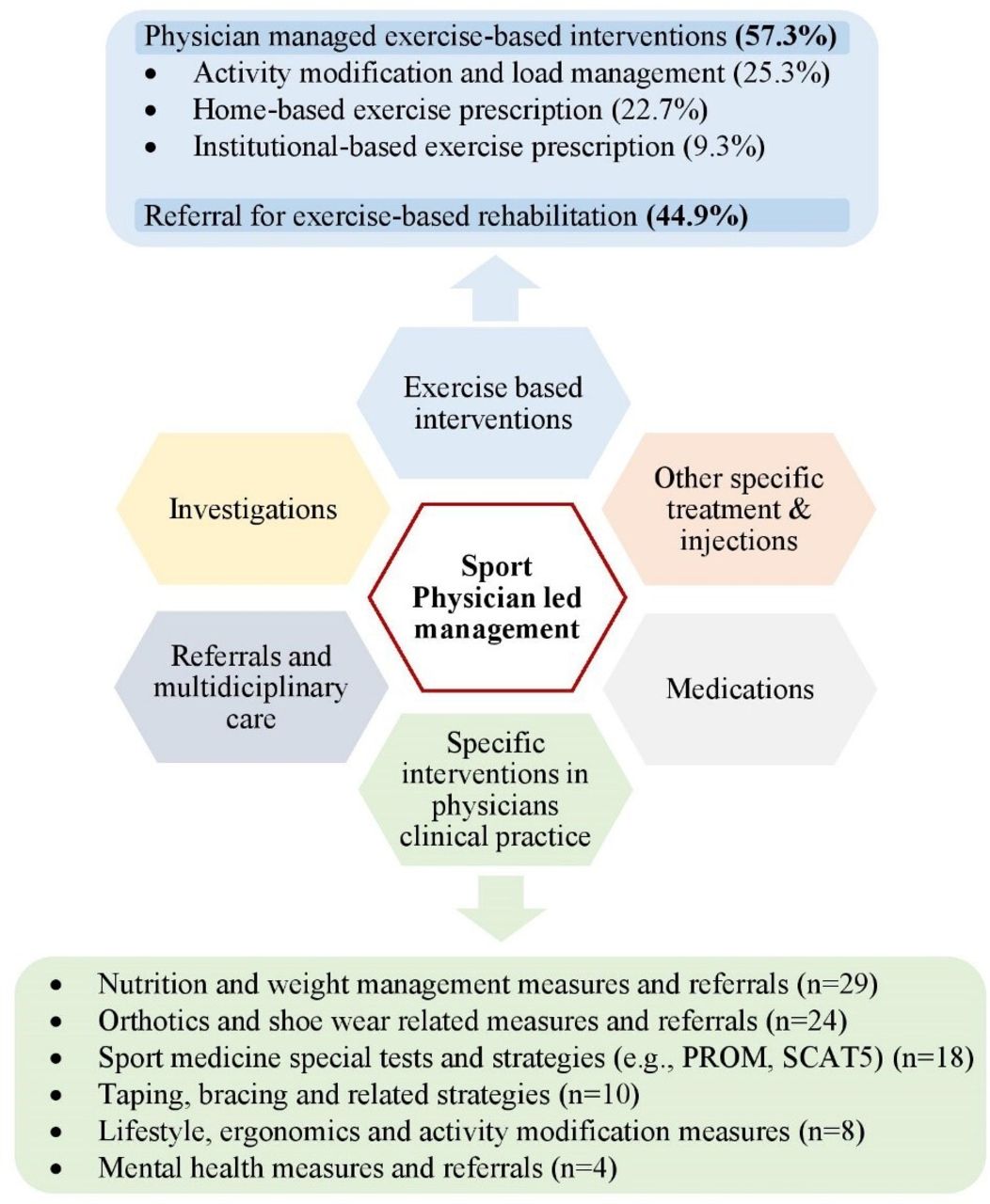
Overview of Sport and Exercise Physician led management strategies including interventions specific to sports medicine clinical practice.
Referral pattern to and from physicians in this study
Most patients (n=355; 81.8%) were referred by general practitioners, 4.6% (n=20) by medical specialists and 9.4% (n=41) by allied health professionals (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
An overview of multidisciplinary network of patient referral to and from physicians.
Physicians referred patients to a broad range of allied health and medical healthcare providers. Figure 5 provides an overview of referral patterns consistent with a multidisciplinary approach to patient management. Patients were referred to allied health professionals, including physiotherapists (n=170; 40.6%), exercise physiologists (n=15; 3.6%) and podiatrists (n=11; 2.6%). Most specialist medical referrals were to orthopaedic surgeons (n=19; 4.5%).
Cost analysis
The total cost for previous medical and allied health consultations, investigations and treatments was calculated to obtain an estimated cost for patients before visiting the Sport and Exercise Physicians (online supplemental file 4). On average, total estimated cost for previous allied health and medical consultations were $A140 053.94 (3235.30 per patient) and $A114 517.00 (1238.10 per patient), respectively. Based on the available data for previous radiological investigations, the total estimated cost was $A90 280.20, of which $A62 092.80 (68.8%) was for MRI. Methodology used to estimate the cost and assumptions made during calculation are detailed in online supplemental file 4.
Supplemental material
Patient satisfaction with treatment
Patients completed a total of 144 pretest and 36 post-test surveys. Patient reported general health scores for all five categories showed improved symptoms at 8 weeks, and are presented in online supplemental file 5. The results showed an increase satisfaction with treatment in mobility by 9.6% (pretest=202.2 and post-test=182.8), self-care by 9.5% (pretest=129.5 and post-test=117.20), usual activities by 17.9% (pretest=250.7 and post-test=205.7), pain/discomfort by 13.4% (pretest=283.8 and post-test=245.7) and anxiety/depression by 8.5% (pretest=174.6 and post-test=159.8).
Supplemental material
Discussion
The results of this study highlight that Sport and Exercise Physicians in Australia provide specialised care for complex, chronic musculoskeletal conditions, which require physician centred multidisciplinary patient care involving both medical and allied health specialities. The conditions seen by Sport and Exercise Physicians typically require further assessment, investigations and specific management strategies including interventions and exercise-based measures. These findings enable us to further understand the role of Sport and Exercise Physicians in the management of complex musculoskeletal conditions, which assists in promoting services and patient care at community level.4 15
The most significant finding of the study is that 74% of all patients received exercise-based interventions, more than 57% of which were delivered by the physician. This is in line with evidence indicating that exercise-based interventions are effective in managing all nine of the National Health Priority Areas including cancer control, cardiovascular health, injury prevention, mental health, diabetes mellitus, asthma, arthritis and musculoskeletal conditions, obesity and dementia.12 For musculoskeletal conditions, exercise-based interventions serve as a primary treatment modality in rehabilitating patients and restoring their functional capacity.12 16 Further, promoting lifestyle modifications, exercise and physical activities in the community is vital in primary, secondary and tertiary prevention of chronic medical conditions including NCDs.17
NCDs account for a major component of the public health and economic burden globally, with increasing prevalence among young adults and children.18 The ACSEP acknowledges ‘Exercise is Medicine’ for the management and prevention of NCDs, musculoskeletal conditions and to promote well-being in every aspect of health among athletes and patients of all ages and abilities. Sport and Exercise Physicians are well placed to deliver physical activity recommendations and exercise prescription, as a result of specialist training with curriculum components focused on exercise intervention.15 19 20 However, our study revealed that 97% of patients presenting to Sport and Exercise Physicians were for musculoskeletal-related problems. This infers that less than 3% of patients were referred to Sport and Exercise Physicians specifically for lifestyle, physical activity and exercise-related interventions for patients with NCD. This may be due to limited awareness and acknowledgement of the role of specialist Sport and Exercise Physicians in promoting physical activity and prescribing exercises for chronic medical conditions and NCD. This knowledge gap may have prevented general practitioners, medical specialists (primarily those managing patients with NCDs) and other health professionals referring patients for this purpose. Policy decisions at government and institutional levels recognising evidenced-based care, would assist Sport and Exercise Physicians to promote services targeting modifiable risks associated with NCDs primarily through education, physical activity promotion and exercise interventions.
Patient characteristics highlight the complexity of the conditions seen by Sport and Exercise Physicians in clinical practice. Over 60% of patients had had symptoms for more than 6 months and 42% did not have a diagnosis at presentation, reflecting the long and complex histories in this patient population. Adding to the complexity, the results showed the involvement of other healthcare providers in the management. Over 80% of patients had seen more than one allied health practitioner including physiotherapists, osteopaths, chiropractors, podiatrists and exercise physiologists and the majority had also seen other specialist medical practitioners including orthopaedic surgeons, rheumatologists, neurologists, endocrinologists and other specialists. Overall, this shows how complex and challenging these patients can be at the time they present to Sport and Exercise Physicians. This may also delay patients presenting to Sport and Exercise Physicians. Therefore, it is important that all medical and allied healthcare providers have a better understanding of the role and scope of Sport and Exercise Physicians, so appropriate and timely referrals can be made.21 22
Musculoskeletal-related conditions are the most common reason for accessing healthcare services in Australia, costing around $A4 billion that contribute to 7.5% of total health expenditure.11 23 The present study provides an overview of the cost involved for patients, before presenting to Sport and Exercise Physicians. We observed a large number of previous allied health and medical consultations, radiological investigations and treatments that resulted in considerable financial burden on patients. An early referral to Sport and Exercise Physicians may help to minimise unnecessary radiological investigations and potential delays in treatment, which can be both time and cost-effective for patients. Seventy-five per cent of patients in this study had undergone a radiological investigation prior to referral including a high proportion of MRI scans (40.1%) and CT scans (11.2%). More recent literature suggest, MRI and CT scans are not required in majority of patients with low back pain,24 and MRI should not be used in a clinical setting for diagnosis of osteoarthritis.25 Further, appropriateness and rationale of requesting MRI have been evaluated in previous studies and suggested that specialist-ordered MRIs influence clinical management significantly more often than primary care physicians.26 27 The importance of collaborative effort among clinicians and policymakers has been highlighted in the Australian context, to prioritise clinical research and funding to minimise the burden associated with musculoskeletal conditions.28
Managing athletic injuries and chronic musculoskeletal conditions frequently requires a patient-centred multidisciplinary team approach.29 In line with this, study results showed physicians initiated 271 referrals to 26 different allied health and medical specialities. Diversity of patient care and referrals were not limited to allied health specialities such as physiotherapists (including hand physiotherapists), osteopaths, podiatrists, but also to psychologists and dieticians. This also extended to medical specialists, who included referrals to orthopaedic surgeons, pain physicians and other physician specialty groups. Interestingly, mental health is a crucial aspect of health and well-being of athletes and physically active individuals, and Sport and Exercise Physicians demonstrated appropriate referrals for psychological input.30 While this collaborative network is key for effective patient management and care,31 this study highlights the central role of Sport and Exercise Physicians in the multidisciplinary team and how they lead in this network to deliver fully integrated sport and exercise medicine services to patients.32
A recent systematic review identified 11 recommendations for best practice care for managing musculoskeletal-related pain.33 Our study showed how Sport and Exercise Physicians align with these 11 recommendations through their clinical practice and management of patients. The study also highlighted the complexity of different treatment modalities and other treatment interventions specific to sports physician practice, which are different to allied health interventions in managing musculoskeletal conditions.
One of the limitations of this study was the small sample of Sport and Exercise Physicians, which represent about 10% of Sport and Exercise Physicians cohort in Australia. However, the physicians were representative and distributed across Australia.
Conclusion
Sport and Exercise Physicians represent one of the newer medical specialities. This paper identifies their role in the community in Australia. Our work reveals the patients seen in sport and exercise medicine practice are complex and predominantly musculoskeletal in nature. Management delivered by Sport and Exercise Physicians included diagnostic expertise, multidisciplinary patient care and physician specific management strategies. This is the first objective assessment of Sport and Exercise Physicians role in the Australasian region. Our findings will assist sport and exercise medicine stakeholders and government policy makers in developing appropriate programmes to support patients and create integrated sport and exercise medicine services to the community.
Data availability statement
Data are available in a public, open access repository. Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
This study has been approved by the Human Research Ethics Committee of the University of Melbourne (Ethics ID number: 2057341).
Acknowledgments
The authors wish to acknowledge the effort of the Sport and Exercise Physicians those took part in this study and taking their time to complete patient data, and the patients who consented and completed the surveys. The authors also thank reception and management staff of the physician clinics assisting with coordinating data collection process.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @kyliefitz01, @sportsdocaus
Contributors JF and DH led the study design, and other authors (JO, KF, PJG and SS) contributed to it. PJG and SS led data collection and management, analysis and interpretation of data, and drafting the initial manuscript. The manuscript was reviewed and edited by JF, DH, JO and KF, and all authors approved the final version for submission. JF is the guarantor.
Funding JO was supported by a Postdoctoral Fellowship (Award Reference No. 104809) from the National Heart Foundation of Australia.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.