Article Text

Abstract
Objectives To determine the intensity, barriers and correlates of physical activity (PA) in Iranian pregnant women.
Methods This cross-sectional study was carried out with 300 eligible pregnant women referred to the Ilam health centres and bases using stratified random sampling with proportional allocation. Data collection tools included a demographic and obstetrical history questionnaire, the Pregnancy Physical Activity Questionnaire and the Exercise Benefits/Barriers Scale. The association between demographic and obstetrical characteristics and PA intensity and barriers were studied using multiple linear regression models.
Results The mean and SD of the total score of PA intensity were 47.15 and 26.25 metabolic equivalent of task (MET)-hour/week, respectively. The highest and the lowest barriers were related to the time expenditure (42.77±18.04) and family discouragement (50.72±24.99) constructs, respectively. The PA intensity was significantly associated with prepregnancy or early pregnancy body mass index (B=25.6), ethnicity (B=16.94), level of education (B=−8.77), number of children (B=5.95), gestational age (B=0.81), participation in childbirth preparation classes (B=−11.27), habitual exercise before pregnancy (B=6.09), income (B=−9.22). The PA barriers were significantly associated with ethnicity (B=−4.96), income (B=2.23) and habitual exercise before pregnancy (B =−1.35).
Conclusion PA intensity may be enhanced by encouraging individuals to be more physically active before pregnancy. Additionally, strategies to enhance support from friends and family to engage in PA throughout pregnancy and PA interventions focused on women with lower levels of income and education are required.
- physical activity
- pregnancy
- quantitative
Data availability statement
Data may be obtained from a third party and are not publicly available. no comment.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key messages
What is already known?
Despite all the known benefits of physical activity (PA), many pregnant women do not participate in regular PA.
Previous studies have cited different barriers and facilitators to PA during pregnancy, including personal, environmental, organisational and political factors.
Iranian women’s very low engagement in moderate to vigorous-intensity exercise during pregnancy, there are likely several context-specific barriers to PA.
No study has addressed such barriers among Iranian pregnant women specifically for whom PA is considered highly important.
What are the new findings?
In the present sample of Iranian pregnant women, the highest weekly energy expenditure was attributed to light-intensity PA.
The highest and the lowest barrier scores were related to the time expenditure and family discouragement constructs, respectively.
To increase PA’s intensity, it is best to encourage individuals to be more physically active before pregnancy and improve family and friends’ support to encourage women to exercise during pregnancy.
Interventions should be developed that focus on pregnant women with low education and low income in improving the intensity of PA.
Background
Pregnancy is a life-changing event that can alter individuals’ physical activity (PA).1 Yet, despite all the known benefits of PA, many pregnant women do not participate in regular PA.2 The US Department of Health and Human Services (2018) has recommended that all pregnant women who do not have specific contraindications participate in regular aerobic and strength-training exercises during pregnancy.3 PA during pregnancy is associated with reduced gestational diabetes, preterm labour and risk of pre-eclampsia2 and decreased postpartum depression.4–6 Moreover, exercise in the second and third trimesters lowers the risk of caesarean birth.7 Thus, improved strategies to engage pregnant women in PA would be welcomed.
One study conducted in the USA identified that 31% of pregnant women included as participants reported engaging in mild-intensity activities, 38% in moderate-intensity and 32% in vigorous-intensity PA.4 In contrast, a survey conducted with pregnant women in Isfahan (a city in Iran) indicated that 98.7% of pregnant women engaged in mild-intensity PA, while only 1.3% reached moderate-intensity levels.5 Previous studies have cited different barriers and facilitators to PA during pregnancy, including personal, environmental, organisational and political factors.8–10 However, given Iranian womens’ very low engagement in moderate to vigorous-intensity exercise during pregnancy, there are likely several context-specific barriers to PA. The low levels of PA noted are not necessarily caused by a lack of interest,11 and many of the barriers towards PA in general in this region may relate to religion and culture. For example, due to wearing a hijab outdoors, many Muslim women in the warmer climates of Iran may prefer to exercise indoors, which is not always available.12 Most Iranian women identify as housewives, have no income and thus depend on their partners to pay for PA.13 This lack of financial independence may also be an important barrier to undertaking PA. Conversely, while limited entertainment is available for women in Iran, a high desire to watch television series is considered another obstacle towards PA.14 Finally, a lack of awareness and/or knowledge on how exercise can be incorporated into everyday life without additional cost has also been identified as a barrier to engaging in exercise among individuals in this context.15 16
While the number of studies outlined here relate to barriers towards PA for Iranian women, no study has addressed such barriers among Iranian pregnant women specifically for whom PA is considered highly important. Thus, a cross-sectional study to identify the most important PA-associated factors for pregnant Iranian women was considered essential for designing future interventional studies to increase PA and improve maternal health. Accordingly, this study determined the intensity, barriers and correlates of PA among Iranian pregnant women.
Methods
Study design
The present cross-sectional study included pregnant women referred to perinatal clinics and health centres in Ilam, a province of Iran (see online supplemental material 1). The Health centre base is a subset of the comprehensive urban health centres located in the city’s suburbs. Informed written consent was obtained from all participants after providing information on the study purpose and procedures. Participants were assured of the confidentiality of their information.
Supplemental material
Study sample
We used G * power software to determine the required sample size. The sample size calculation yielded a required number of 300 participants, based on a 95% confidence level, a power of 0.8, an effect size of 0.06 and the consideration of 12 predictor variables.
Sampling was conducted continuously from September to December 2018 using stratified sampling from women referred to perinatal clinics by the proportional allocation of comprehensive urban health centre floors and bases. The inclusion criteria were Iranian, aged between 18 and 45 years, gestational age between 10 and 37 weeks, no contraindication to exercise during pregnancy,17 no movement restrictions, the ability to read and write, and informed written consent to participate in the study.
Outcome measures and measurements
Data collection tools comprised a demographic and obstetrical history questionnaire (independent variables), the Pregnancy Physical Activity Questionnaire (PPAQ) and the Exercise Benefits/Barriers Scale (EBBS) (dependent variables).
The demographic and obstetrical history questionnaire consisted of variables such as age, prepregnancy or early pregnancy body mass index (BMI), ethnicity, level of education, occupation, income (reported based on individual’s perception of income and to what extent it meets individual’s living needs), number of previous pregnancies, number of children, gestational age, participation in childbirth preparation classes and the presence of habitual exercise before pregnancy.
The PPAQ designed by Chasan-Taber et al. assesses PA levels during pregnancy. This questionnaire asks respondents to select the category that best approximates the amount of time spent in 32 activities, including household/caregiving, occupational, sports/exercise and inactivity during the current trimester. At the end of the PPAQ, an open-ended section allows the respondent to add additional activities not listed. The duration of time spent in each activity is multiplied by its intensity to measure average weekly energy expenditure (MET-hour/week) attributable to each activity. Finally, the activities are divided into seven categories: sedentary activity, light-intensity, moderate-intensity, vigorous-intensity, household/caregiving, occupational and sports/exercise. The questionnaire′s reliability was confirmed with a Cronbach’s alpha of 0.78 for the total score and 0.87–0.93 for questionnaire categories.18 The validity and reliability of the Persian version of PPAQ were confirmed by Fathnezhad Kazemi et al19
The EBBS assesses the benefits and barriers of exercise. The English version of the EBBS consists of 43 items: 29 items of the benefits subscale and 14 of the barriers subscale. The scales are designed based on a 4-point Likert scale: strongly agree,4 agree,3 disagree,2 strongly disagree.1 The barrier scale is composed of four constructs: time expenditure (three items with total score 3–12), exercise milieu (six items with total score 6–24), physical exertion (three items with total score 3–12) and family discouragement (two items with total score 2–8). The minimum score for the barrier subscale is 14, while the maximum score is 56. In this scoring system, a higher score represents a greater perception of barriers. The internal reliability of the EBBS scale was confirmed with the Cronbach’s alpha coefficient of 0.952, and the benefits and barriers subscales were 0.953 and 0.886, respectively.20 The validity of the Persian version of the questionnaire was confirmed, and the reliability of the barriers subscale was validated with Cronbach’s alpha coefficient of 0.82 and Spearman Brown’s coefficient of 0.74.21 In this study, to examine the face validity of the PA barrier items, the questionnaire was completed by 20 eligible women of the study, according to whose opinions items 6 and 19 were repetitive. Therefore, due to the high correlation between these two items (r=0.87), item 6 (exercise makes me tired) was removed.
Analyses
The data were analysed using SPSS V.21 (SPSS). Following the assessment of skewness and kurtosis, the quantitative data were considered to be normally distributed. Descriptive statistics, including frequencies and percentages, mean and SD, were used for describing demographic and obstetrical history variables, barriers to PA and intensity of PA. To compare the constructs of PA barriers, the obtained scores were normalised to a maximum score of 100. Higher scores indicate a higher number of barriers. To calculate each construct’s normalised score, its score was subtracted from the minimum score of that construct and divided by the difference of maximum and a minimum score of that construct. Finally, the answer of the obtained was multiplied by 100.
To compare the intensity and barriers of PA (quantitative variables) among demographic and obstetrical history variables (categorical variables), an independent t-test and ANOVA were used. Pearson’s correlation coefficient test was used to determine the relationship between the intensity and barriers of PA with demographic and obstetrical history variables that were considered quantitative variables.
To determine the relationship of each one of the independent variables (demographic and obstetrical history variables) on the dependent variable (intensity and barriers to PA separately as both were reported as quantitative variables), those variables that confirmed significance in the bivariate test (p<0.05) were entered into a multiple linear regression model using a backward strategy. Before the multivariate analysis, regression assumptions, including normality of residuals, homogeneity of residual changes, alignment of outliers and residuals independence, were examined and confirmed. Results from the linear regression analysis are presented as beta coefficients with associated 95% CIs. The level of statistical significance was set at p<0.05.
Results
Participants
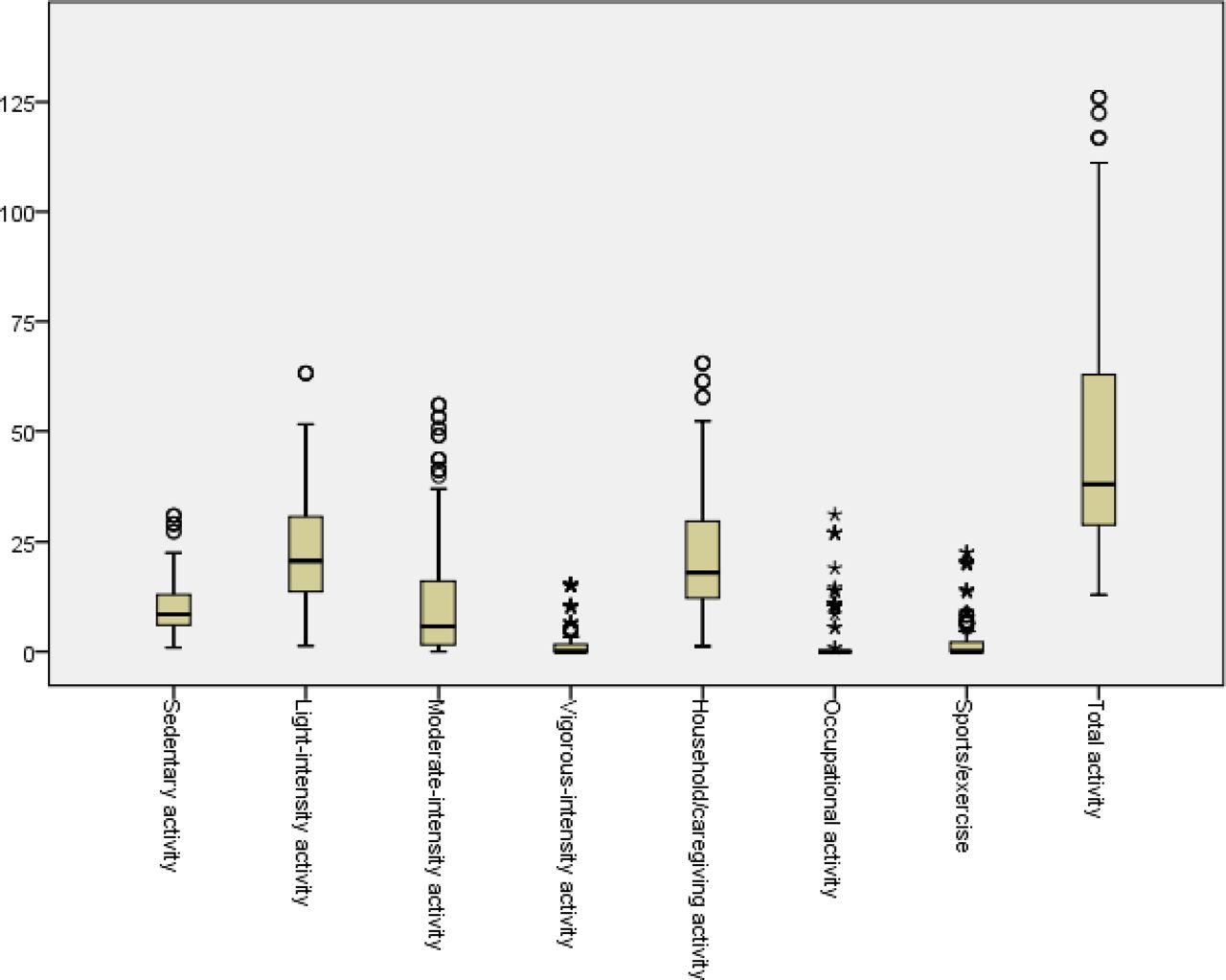
Participants had a mean age of 27.52 (SD ±5.28) years. The mean prepregnancy or early pregnancy BMI was 26.03 (SD ±4.28) kg/ m2, and the gestational age was 23.77 (SD ±8.61) weeks. Most participants (n=181; 60.33%) had a university education and a favourable economic status (n=150; 50%). Box plot of scores of pregnant women’s PA intensity based on energy expenditure (MET-hour/week) and its categories are reported in figure 1.
{kind=link}
Box plot of scores of pregnant women’s PA intensity based on energy expenditure (MET-hour/week) and its categories (n=300). MET, metabolic equivalent of task; PA, physical activity.
PA levels
The average total score of PA intensity in women was 47.15 (SD=26.25) MET-hour/week. The lowest amount of PA based on energy expenditure was attributed to vigorous-intensity PA. The highest amount of PA based on energy expenditure was attributed to light-intensity PA. The activities reported were mostly light-intensity and related to household/caregiving activities, while sports/exercise, vigorous-intensity activity and occupational activity were reportedly low (figure 1). Based on the activity type, household activities had the highest, while occupational activities had the lowest energy expenditure.
PA barriers
The average total score in relation to PA barriers in this population was 30.72 (SD=5.81). Table 1 shows constructs of PA barriers, where the highest barrier scores were related to family discouragement and the lowest barrier scores with time expenditure constructs based on average % of the total score.
Scores of pregnant women’s PA barriers and its constructs (n=300)
Online supplemental materials 2 and 3, respectively, present the numerical indices total PA intensity, PA intensity and PA barriers regarding demographic and obstetrical history variables of the studied samples.
PA correlates
To estimate the effect of demographic and obstetrical history variables on PA’s intensity and barriers, all variables with p<0.05 based on the results of online supplemental materials 2 and 3 were entered into the linear regression model using the backward method. According to the results in table 2, the relationship of demographic and obstetrical history variables on the intensity of PA, among the variables that entered into the model including prepregnancy or early pregnancy BMI, ethnicity, education, income, number of children, gestational age, participation in childbirth preparation classes and habitual exercising before pregnancy remained in the model. For one score increase in the prepregnancy or early pregnancy BMI in the obese category and increasing gestational age, the intensity of the PA increased by 25.6 and 0.81 units, respectively. The intensity score of PA in women who habitually exercised before pregnancy increased by 6.09 units. In women from the Fars ethnic grouping compared with those from the Kurdish grouping, there was a 16.94 score increase in the intensity score of PA and a 5.95 score increase for the addition of each child. At the same time, women with a high school diploma were reported to have an 8.77 lower score than those with a university education. Women who participated in childbirth preparation classes had an 11.27 lower score than those who did not. Women with 20–40 million rials income compared with those earning 40–100 million rials had a 9.22 lower score in the intensity of their PA. Consequently, 26.1% of the variations in the dependent variable (intensity of PA) was justified by the independent variables.
Relationship of pregnant women’s demographic and obstetrical history characteristics with the PA intensity based on the results of multiple linear regression analysis
According to the obtained results displayed in table 3, the relationship of demographic and obstetrical history variables on the barriers of PA, among the variables entered in the model including ethnicity, income, number of pregnancies, and habitual exercise; the number of pregnancies was the only variable that did not remain in the model. Women within the Lur ethnic grouping compared with those within the Kurdish ethnic grouping scored 2.52 more units, while women with an income of 20–40 million rials compared with women earning 20–40 million rials scored 2.23 more units in relation to the barriers to PA. Women who habitually exercised before pregnancy scored 1.35 fewer units in relation to the barriers to PA than women who did not. Overall, 8.3% of variations in the barriers to PA have been explained by independent variables, ethnicity, income and habitually exercising before pregnancy.
Relationship of pregnant women’s demographic and obstetrical history characteristics with the PA barriers based on the results of multiple linear regression analysis
Discussion
Our findings outline the intensity, barriers and correlates of PA in Iranian pregnant women. Here, the mean total score of PA intensity based on MET-hour/week and the SD were 47.15 and 26.25, respectively. The highest intensity PA was attributed to light-intensity activity. In contrast, the lowest intensity PA was attributed to vigorous-intensity activity. In relation to activity type, household activities had the highest, while occupational activities had the lowest energy expenditure overall.
The findings presented here are comparable to those of Nascimento et al22 except for the lowest activity level, which is related to exercising rather than occupational activity. Yet interestingly, in Nascimento et al22’s study, sampling was conducted during the postpartum period when it seems unlikely that women would engage in any exercise activity. Additionally, the number of employed women in the sample was estimated at 54.15%, indicating a sample experiencing increased occupational activities. While conversely, in this study, only 13.66% of participants were employed as physicians (7.3%), other employees (53.65%) and teachers (39.02%), respectively. Given that these jobs are generally associated with less energy expenditure, they may lower the level of occupational activity and energy expenditure. According to further studies, with increasing gestational age and increased participation in leisure time, PA also persists in decreasing well into the postpartum period.23 24 Such findings may point to the need for PA promotion in the workplace and throughout the postnatal period.
In another study, the lowest activity level was related to sport/exercise,25 while the lowest activity level was related to occupational activity in this study. Yet in Antosiak-Cyrak and Demuth’s study, one out of three women were urban residents, and the rest lived in rural regions,25 while in this study, all participants lived in the city. This suggests that PA promotion may need tailoring to address the needs of women living in both rural and urban settings, particularly as women living in urban areas can have greater access to sports facilities (such as clubs) than women living in rural areas, and therefore, engage in less exercise overall.26 Yet, these women may be more physically active in other ways. So it will also be important for future studies to capture qualitative data to offer richer context in this regard.
According to the results presented in this study, family discouragement was perceived as the greatest barrier to PA, while time expenditure was perceived as the least important barrier. Factors such as not having a sexual partner and family support have previously been associated with poor PA in women.27 Also, having an active spouse before pregnancy has been identified as the strongest predictor of performing moderate-intensity to vigorous-intensity PA during pregnancy.28 In another study, pregnant women also describe the value of social support from family, friends, and health professionals as facilitators to PA.29 Such findings indicate the need to engage families and spouses in future interventions designed to enhance PA in pregnancy.
Demographic and obstetrical history characteristics, prepregnancy or early pregnancy BMI, ethnicity, level of education, income, number of children, gestational age, participation in childbirth preparation classes and having exercise habits before pregnancy had a significant relationship with the total PA intensity. Accordingly, these characteristics will also be important to consider in the development of any future interventions. Specifically, women with a BMI above 30 kg/m2 before or at the beginning of their pregnancy had a higher mean energy expenditure intensity. Despite this finding, Haakstad et al30 have previously reported no significant relationship between the prepregnancy or early pregnancy BMI of women who exercise in the third trimester and women who did not. Other studies have similarly shown no significant relationship between prepregnancy BMI and exercise during pregnancy.22 31 This discrepancy may be explained by the fact that many of the participants in this study with a BMI above 30 kg/m2 had experienced more pregnancies than those with a lower BMI. Nevertheless, larger sample sizes in future may explain this phenomenon in greater clarity.
Although the intensity of energy expenditure in this study was higher in women who had a high BMI before or early pregnancy, this energy was predominantly spent on low-intensity activities. Consistent with these results, an earlier study also identified a statistically significant relationship between prepregnancy BMI in women who exercised in the third trimester and women who did not.30 Yet alternative studies have reported no significant relationships between prepregnancy BMI and exercise during pregnancy.22 31 Nevertheless, there remains an opportunity to promote higher intensity PA in this group, both before and after pregnancy.
In this study, the highest to lowest total energy expenditure belonged to the following ethnic groupings, respectively; Fars, Lak, Kurdish and Lur. This may be explained by the fact that Persian women may be more accustomed to exercise before pregnancy. For example, in our sample, 7 out of 11 Persian women (63.6%) were accustomed to exercising before pregnancy, while out of a population of 289 non-Persian women, only 103 (35.6%) of them exercised before pregnancy. Indeed, other research has established that habitually exercising before pregnancy increases the chance of exercising during pregnancy,22 and a lack of PA before pregnancy has been identified to be the strongest predictor of reduced exercise during the third trimester of pregnancy.22 23 30 More research is required to understand any links between ethnicity and PA more comprehensively. Nevertheless, there remains an opportunity for future interventions to promote PA before pregnancy in all populations, given the number of women from various ethnic groups not engaged in habitual PA during this time.
Notably, women with a university education experienced a higher intensity of PA. Lack of university education has previously been associated with physical inactivity in pregnant women elsewhere.22 23 32 Yet conversely, in Portuguese women, no statistically significant relationship between education and PA in pregnancy was found.5 26 Such findings suggest that targeted PA toward those with lower levels of education may be useful and that further evidence is required in this area. According to the current study, a higher income was also associated with increased energy expenditure. In two other studies, lower-income levels have similarly been associated with decreased PA.4 33 This suggests that those with lower incomes may also be usefully targeted in the future promotion of PA during pregnancy.
Those with a higher number of children endured a higher level of energy expenditure through carrying out light and moderate household/caregiving. At the same time, childless pregnant women had a higher energy expenditure for carrying out occupational, sport and vigorous activities. The findings of Chasan-Taber et al31 corroborate those presented here in this regard. Such findings may usefully inform the development of interventions promoting PA during pregnancy as women both begin and grow their families.
In our study, gestational age also had a significant correlation with energy expenditure. Indeed, previous studies suggest that participation in PA can increase significantly in the first trimester of pregnancy compared with the second and third trimesters of pregnancy.33 These findings may be useful in tailoring the promotion of PA throughout the entire duration of pregnancy. Consistent with this study’s results, no statistically significant correlation was found between age and PA.4 26 While in other studies, there has been a significant, positive correlation between age and exercise identified.23 34 These discrepancies indicate the need for larger samples and more nuanced mixed-methods explorations of PA, age and pregnancy overall.
This study found that women who did not attend childbirth preparation classes consumed more energy. In interpreting this relationship and perhaps contrary to expectations, childbirth preparation classes offered to pregnant women in Iran do not provide training on the importance of PA in pregnancy and its safety. As such, opportunities remain in integrating PA promotion in childbirth preparation classes in this context, particularly in relation to higher intensity PA. Yet, it is of note that the 85.29% of participants who did not attend childbirth preparation classes had a university education, as this may somewhat account for the higher levels of PA noted in this sample.
The total score of barriers to PA was significantly correlated with individual and obstetrical histories and certain characteristics, including ethnicity, income, number of pregnancies and the presence of habitual exercise before pregnancy. Having a lower income was also significantly correlated with the total score of barriers to PA. Other studies also reported low income as an important barrier,35 while others found no significant relationship.26 Such discrepancies may be explained by the inclusion of different study populations and suggest a need to achieve clarity through mixed-methods triangulation in this regard.
In our study, the number of pregnancies was significantly correlated with PA barriers. For example, women experiencing their third and fourth pregnancies reported greater barriers than those experiencing their first and second pregnancies. Contrary to the results of other studies,23 36 women pregnant for the first time with lower levels of education were more likely at risk of experiencing barriers to PA. This suggests that barriers to PA in all pregnancies could be usefully identified and addressed.
Not being used to exercise before pregnancy also had a significant correlation with barriers to PA. In line with the current study, pregnant women who had been inactive before pregnancy gained a higher barrier score elsewhere.37 38 As compulsory occupational activities can increase daily PA,26 habitual PA could usefully be promoted for women devoid of these before, during and after pregnancy.
A key strength of this study is that it has included multicentre populations and has evaluated the intensity and barriers of PA in all three trimesters of pregnancy. As it was undertaken with women experiencing low-risk pregnancies in urban areas, results cannot be generalised to wider populations. Future studies may usefully be conducted with women experiencing low-risk pregnancies or/and women experiencing high-risk pregnancies living in rural areas who can safely engage in PA. The Barriers to Physical Activity in Pregnancy Scale39 may usefully identify barriers to PA in pregnancy for all groups in future.
Conclusion
This study has determined the intensity, barriers and correlates of PA in Iranian pregnant women. Encouraging individuals to be more physically active before pregnancy and enhanced support from family and spouses who incites women to exercise during and after pregnancy may increase the intensity of PA most effectively. PA interventions could usefully target pregnant women with lower levels of education and income specifically.
Data availability statement
Data may be obtained from a third party and are not publicly available. no comment.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.REC.1397.244).
Acknowledgments
This article results from a master's thesis, funded by the Vice-Chancellor for Research of Iran University of Medical Sciences. I would like to express my sincere gratitude and appreciation from the honourable Vice Chancellor for Research of Iran and Ilam University of Medical Sciences, the sincere cooperation of pregnant women who participated in the research and referred to Ilam health centres and bases, and the honourable midwifery professors of Iran University of Medical Sciences.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KA, SBHA-A and LAF designed the study. KA, LAF and SAH analysed and interpreted the data. Moreover, KA, SP and LAF wrote and revised the paper.
Funding The present article is extracted from a master thesis funded by the Research Deputy of Iran University of Medical Sciences, Tehran, Iran.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.