Article Text

Abstract
Aim To estimate the incidence of injury in adult elite women’s football and to characterise the nature and anatomical location of injuries.
Design Systematic review and meta-analysis.
Data sources Combinations of the key terms were entered into the following electronic databases (PubMed, SPORTDiscus, Science Direct and Discover) from inception to May 2021.
Eligibility criteria for selecting studies (1) Used a prospective cohort design; (2) captured data on elite adult women players; (3) reported injury incidence by anatomical site; (4) captured data of at least one season or national team tournament; (5) included a definition of injury; and (6) written in English.
Results The search identified 1378 records. Twelve studies published between 1991 and 2018 were included in our review and sampled 129 teams. In domestic club football, injury incidence rate was estimated to be 5.7/1000 hours (total), 19.5/1000 hours (match) and 3.1/1000 hours (training). In tournament, football match incidence was estimated to be 55.7/1000 hours. The knee (22.8%; 368/1822) was the most common site of injury in domestic club football. The ankle (23.7%, 105/443) was the most common site of injury in tournament football. Ligament sprains were the most common type of injury (27.8%), followed by muscle strains (19.1%). Severn studies (58%) had a high risk of bias associated with exposure definition and measurement and considerable heterogeneity exists between the included studies (I2=49.7%–95%).
Summary/conclusion Ligament sprains occur more frequently in adult elite women football players. We advise caution in interpretating point estimates of the incidence of injury due to high statistical heterogeneity. Standardising injury reporting and the accurate recording of match and training exposure will overcome such limitations.
PROSPERO registration number CRD42019130407.su
- soccer
- female
- epidemiology
- injury
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
What is already known?
The expansion of domestic leagues and tournament competitions allows players the opportunity to train and compete within an elite environment.
Elevated levels of fitness, training intensity and regular competitive matches inherently increases the risk of injury.
A recent meta-analysis including amateur and collegiate level female players estimated the injury incidence rate to be 6.1 injuries/1000 hours of exposure.
What are the new findings?
The estimated incidence rate for adult elite women players in domestic club football is 5.7/1000 hours (total), 19.5/1000 hours (match) and 3.1/1000 hours (training).
The estimated match incidence rate in tournament football is 55.7/1000 hours.
Seven studies (58%) had a high risk of bias associated with exposure definition and measurement.
Significant heterogeneity exists between the studies available (I2= 49.7 to 95%).
Standardising injury and illness definitions, medical reporting of injuries and accurate recording of match and training exposure in women’s football is needed.
Introduction
Women’s football is played in more than 100 countries and the Fédération Internationale de Football Association 2019 Women’s Football Strategy aspires to double participation rates to 60 million by 2026.1 A recent scoping review in 2021 revealed that sports medicine research including studies relating to injury (451 studies) and illness (29 studies) was the most common theme in women’s football research to date.2 A recent meta-analysis including amateur and collegiate level female players estimated the injury incidence rate to be 6.1 injuries/1000 hours of exposure.3
In 2017, it was estimated that there were 1790 professional and 1782 semiprofessional registered adult women players in Europe.4 Up-to-date participation rates are difficult to obtain as they rely on retrospective survey data collated from participating football associations from the preceding season. A useful proxy measure of increased participation is the expansion of elite domestic leagues and international competitions which allows players the opportunity to train and compete within an elite environment.5 6
An initial search of published literature did not find any systematic reviews with meta-analyses of pooled observational cohort data estimating the incidence of injury in adult elite women’s domestic league football and tournament football. The primary aim of our systematic review was to estimate the incidence of injury (overall, match and training) in elite adult women’s football. A secondary aim was to characterise the nature and anatomical location of injuries.
Method
This review was prepared and conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.7 The Condition, Context, Population framework8 for reviews addressing a question relevant to incidence or prevalence was considered when eligibility criteria was established and agreed on by authors.
Inclusion and exclusion criteria
Inclusion criteria were reports of studies that: (1) used a prospective cohort design; (2) captured data on elite level or national team female/women players; (3) reported injury incidence by anatomical site; (4) captured data of at least one season or team tournament; (5) included a definition of injury and (6) were written in English. Elite-level participation was considered as the two highest national football league divisions within the country of publication, providing the level of participation (of participants) included in the review.9
The following articles were excluded: (1) expert opinions, case reports/series, case–control studies, cross-sectional studies, self-report or retrospective studies; (2) studies conducted in male football only; (3) studies conducted on samples aged <18 years; (4) studies conducted on amateur players only and (5) studies conducted on alternative versions of football including; five-a-side, futsal, indoor football (six-a-side), Paralympic football, powerchair football, beach football, street football, three-sided football or walking football.
Literature search
Two authors (LM and AA) carried out a search of the electronic databases (from inception to May 2021 PubMed, SPORTDiscus, Science Direct and Discover). For full-text publications of cohort studies that reported incidence of injury in adult elite women’s football (online supplemental appendix S1: Search string). All citations were imported to EndNote X7 (Thomson Reuters, USA) and duplicates were removed by LM.
Supplemental material
Literature screening
Two reviewers (LM and AA) independently screened title and abstracts of records and obtained full texts of potentially eligible studies. Full texts were screened independently (LM and AA) against the inclusion criteria and any disagreements were resolved via consensus with a third reviewer (GJ) acting as arbiter. Handsearching the reference list of a recent systematic review3 was conducted. No handsearch of specific sports medicine journals was performed.
Quality and risk of bias assessment
Two authors (LM and AA) independently assessed the methodological quality of included studies using a modified version of the Newcastle-Ottawa Scale (NOS). The version replicated the scale used in a previous systematic review and meta-analysis of injury in women’s football.3 The criteria descriptors were adjusted for the purpose of this review (online supplemental appendix S2). One star could be awarded for each criterion if methodological detail was clearly reported. Eight stars could be awarded for a given study and were categorised into low-quality ‘≤3 stars’, moderate-quality ‘≥4 to ≤6 stars’ and high-quality studies ‘≥7 stars’.10 Reporting quality was assessed using a tool adapted from Strengthening The Reporting of Observational Studies in Epidemiology statement (STROBE)11 that had been used in a previous systematic review of injury epidemiology in football.12 The tool had five items: (1) study setting, location and study period; (2) eligibility criteria and sources and methods of participant selection; (3) exposure definition and measurement; (4) study outcome definition and measurement and (5) main result and precision. Summary of the quality of evidence were presented with items judged as low risk of bias were awarded 1 point, high-risk items were awarded 0 points, resulting in a possible range of 0–5 in total for every included study (online supplemental appendix S3, S6 and S7).
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Data extraction
The following study information was extracted and recorded on a data extraction proforma by one reviewer (LM) and checked for accuracy by a second reviewer (GJ): study characteristics (authors, publication year, country of origin); characteristics of the study population; study design; injury definition and football exposure (study period, number of teams and seasons, total, match and training exposure), (1) incidence of injuries/1000 hours, (2) total, training and match exposure, (3) injury tally counts and percentages of injuries, (4) injury severity and (5) sites and types of injuries. Where it was not possible to extract elite player data from studies containing amateur data, contact with authors was made and the extracted data forwarded to LM.
Data management and analysis
Injury count data, exposure time and injury incidence rates per 1000 hours were extracted from the included studies with the reported 95% CI. Where an incidence rate was presented with a SD, it was transformed to a 95% CI using a standardised equation.13
No attempts were made to artificially generate an injury incidence rate by estimating team level exposure to avoid overestimating or underestimating exposure time.14 Data were being extracted from a series of studies that were conducted independently of each other, it is unlikely that studies would be functionally equivalent (eg, difference in exposure hours, number of matches played and training sessions completed, total number of injuries) and this could introduce unobserved heterogeneity. Therefore, a random effects model was used to provide a pooled estimate of the total incidence of injury and for match and training incidence.15
Visual inspection of results and forest plots was performed and heterogeneity was quantified using the I2 statistic, which represents the percentage of total variation across all studies due to between-study heterogeneity. Thresholds for heterogeneity (low, 0%–40%; moderate, 30%–60%; substantial, 50%–90%; considerable heterogeneity, 75%–100%), recommended by Cochrane were used.16 Data analysis was conducted using Comprehensive Meta Analysis (V.3.0) software package.17
Results
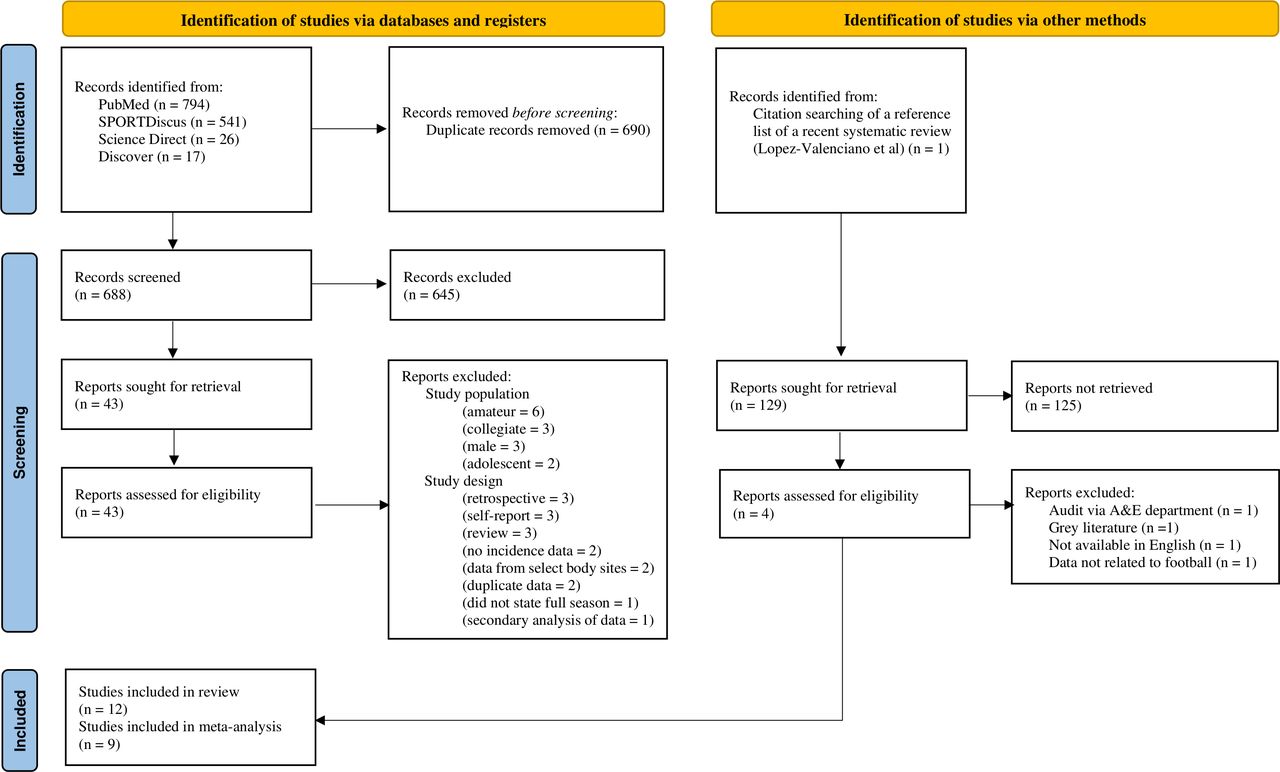
The search identified 1378 records of which 690 records were removed as duplicates and a further 645 records were excluded for not meeting our eligibility criteria on screening of title and abstract (figure 1). The reference list of a recent systematic review3 was screened which revealed four reports that required full text screening. Thus, full-text reports were obtained for 47 records of which 14 were excluded due to the population not being described as adult elite women football players. Twenty-one records were excluded because they did not meet our criteria for either prospective medical reporting of injuries, were review articles, where data were reported via secondary analysis or was not available in English. There were 12 studies included in our review and we were able to extract and pool data from nine studies for meta-analysis. A description of the excluded studies is available in online supplemental appendix S4.
Supplemental material
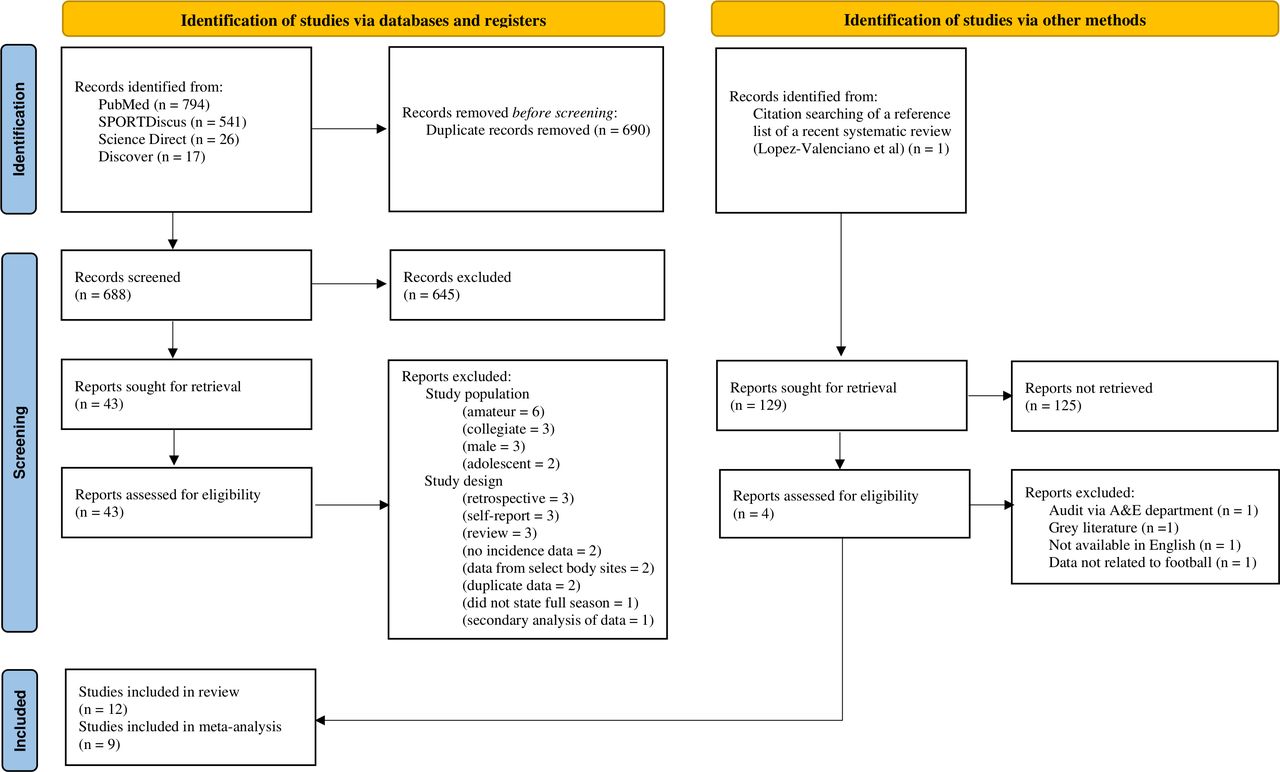
PRIMSA 2020 flow chart of study selection. Adpated from Page et al.7 A&E, Accident and Emergency; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of included studies
There were 12 studies included for review which were published between 1991 and 2018 sampling a total of 129 teams. Ten studies sampled teams from domestic club football (71 teams) which took place between 1988 to 2015 (table 1)18–27 and two studies sampled teams from five national team tournaments (58 teams) taking place between 1999 and 2005 (table 2).28 29
Characteristics of included studies related to club football
Characteristics of included studies related to tournament football
Studies using samples from club football
Of the 10 studies that included participants sampled from domestic football leagues, four were conducted using multiple teams from Sweden,19 23 24 26 two from Germany20 21 and one from each of the following countries: Netherlands,18 Norway,27 Spain25 and USA.22 Eight (80%) studies reported data from multiple teams over one season,18–21 23 24 26 27 one study reported data from multiple teams over two seasons22 and a further study captured data from one team over five seasons.25 The total number of participants from all study samples was 1411. The maximum number of participants in a study was 25421 and the minimum number of participants in a study was 35.25 The maximum duration of data collection (including preseason) was 12 months, and the minimum duration was 7 months (table 1).
A time loss injury definition was used in all studies in domestic club football and more frequently used than a medical attention injury definition. Illnesses were not reported in any studies (online supplemental appendix table S5).
Supplemental material
There was inconsistency in how studies classified injury severity. Five studies19–21 26 27 applied ‘minor, moderate, major’ time-loss (days lost) categories, three studies23–25 reported ‘minimal, mild, moderate and severe’ categories and one study18 applied ‘minimal, slight, mild, moderate and major’ time-loss injury categories. Only two studies28 29 reported a ‘career ending’ time-loss category. While all studies assigned a temporal measure of time (days lost) within each time-loss category, these were inconsistent across studies.
Studies using samples from tournament football
Two studies sampled five national team football tournaments; two Olympic Games, two World Cups28 and one European championship.29 There was a total of 58 national teams included in the two studies. The maximum number of national teams in a tournament was 1628 and the minimum number of teams in a tournament was 8.29 A medical attention injury definition was applied in one study28 (Olympic Games and World Cups), with a further study29 (one European championship) applying a time-loss definition. These studies utilised similar injury severity categories (table 2).
Quality assessment and risk of bias
The average number of stars awarded for study quality (NOS) was 6 (range: 5–8 stars). All studies provided a definition of injury (criteria 2). All studies provided details on assessment outcome (criteria 6) where injuries were recorded via a Diagnostic Coding System (eg, Orchard Sports Injury Illness Classification System. All studies provided sufficient detail that met criteria 7 as the injury surveillance period lasted for at least one football season and/or complete football tournament.
Three studies19 25 26 (25%) provided insufficient evidence that participants were representative of the average football player at the time the study was conducted (criteria 3). Nine studies (75%)18 19 21–25 28 29 provided insufficient evidence that participants were injury free at the start of the study (criteria 5) and two studies (17%)20 24 reported participant loss to follow-up of greater than 20% (criteria 8) (online supplemental appendix S6). The STROBE assessment revealed 11 studies (92%) were assessed as having a low risk of bias for study setting, location and study period (item 1) and 10 studies (83%) had low risk of bias for unclear or biased selection of participants (item 2). Four studies18 23 25 29 (33%) had a low risk of bias across all five items and three studies21 27 28 had a low risk of bias across four items (online supplemental appendix S7). It was noteworthy that seven studies19–22 24 26 28 (58%) had a high risk of bias associated with exposure definition and measurement (item 3) where exposure was not clearly reported or was approximated through a team-level estimate calculation (eg, number of players on the field, multiplied by the number of games and by the factor 1.5 (equivalent to a 90 min match)). There were seven studies19–22 24 26 27 (58%) that had a high risk of bias associated with imprecision of results (item 5) where incidence data were presented without an SD or 95% CI. Any discrepancies between the reviewers during the process of assessing risk of bias were resolved via consensus discussion with an arbitrator (online supplemental appendix S8). Table 5 displays the summary of findings obtained.
Supplemental material
Incidence rate of injury in domestic Club football
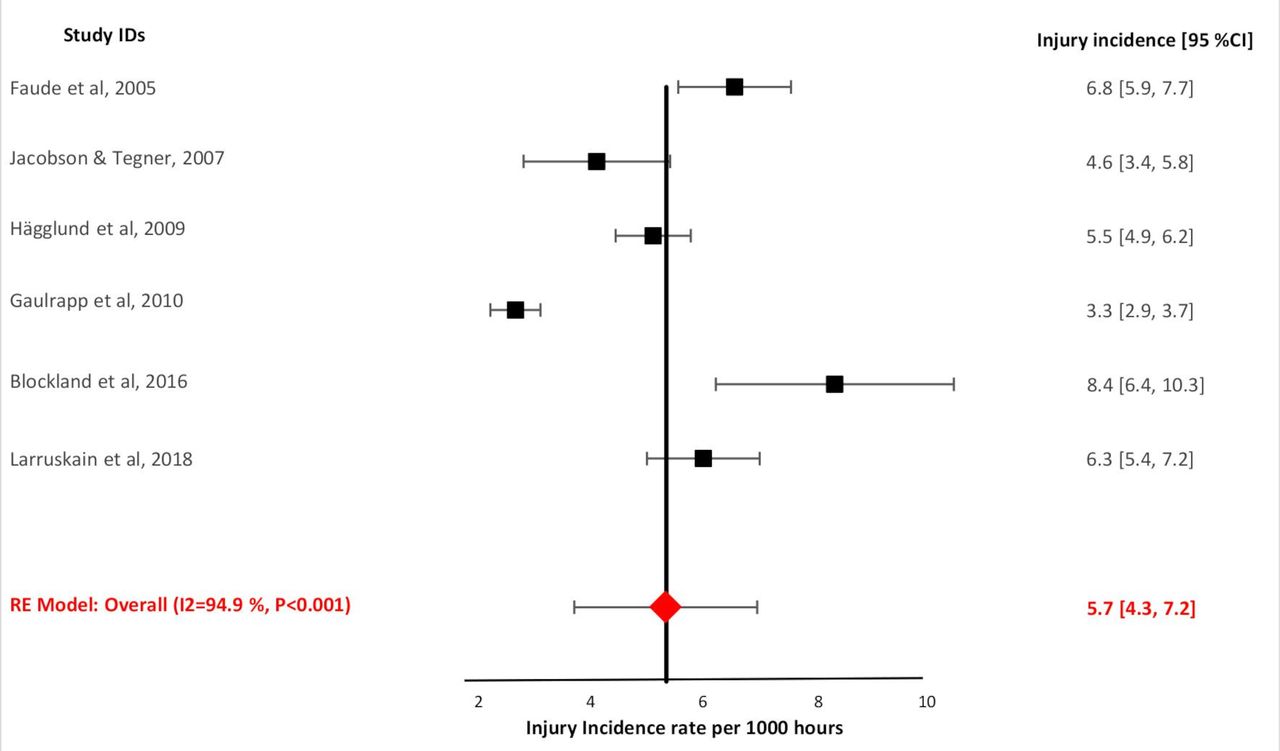
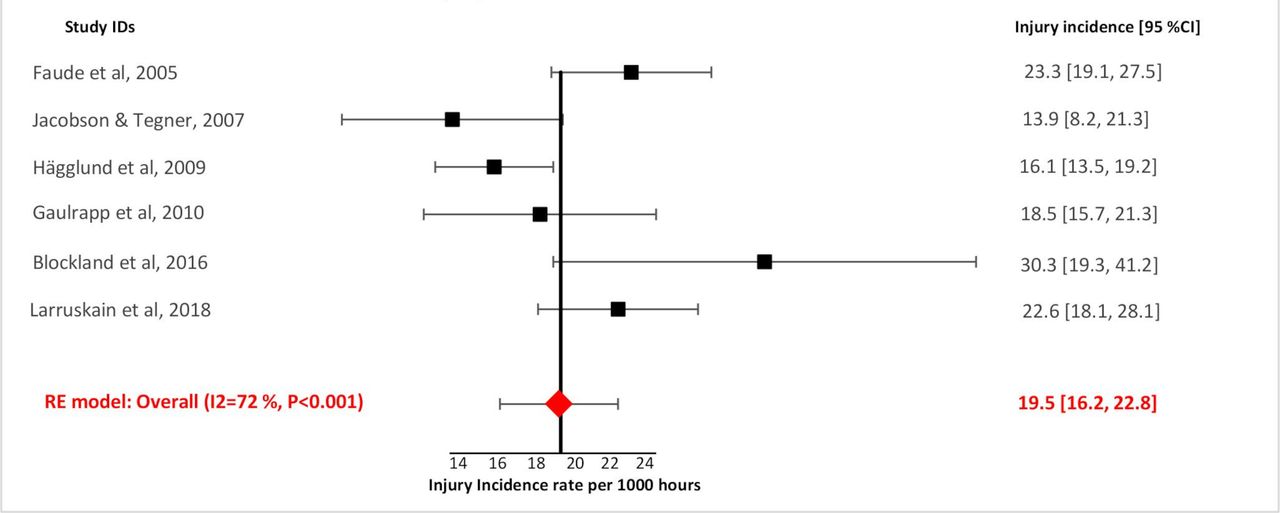
The highest total injury incidence rate was 8.4 injuries/1000 hours, and the lowest rate was 1.93 injuries/1000 hours (table 3). Match injury incidence rate was 30.3/1000 hours (highest) and 12.6/1000 hours (lowest) of exposure. Training incidence rate was 5.2/1000 hours (highest) and 1.2/1000 hours (lowest) of exposure.
Injury incidence data: domestic club football
Incidence rate of injury in tournament football
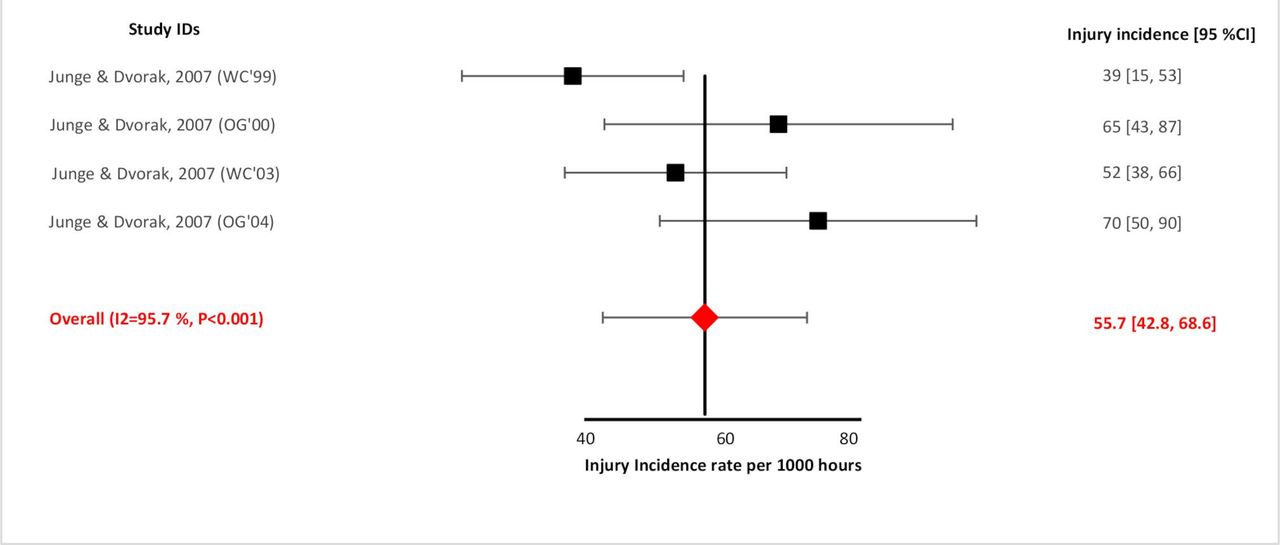
The total injury incidence rate was 70.0/1000 hours (highest) and 39.0/1000 hours of exposure (lowest) when a medical attention injury definition was utilised. The total injury incidence rate was 11.6/1000 hours when a time-loss injury definition was used (table 4).
Injury incidence data: tournament football
Site of injury
In domestic club football, lower limb injuries accounted for 85% of all injuries (1373/1615). The knee (23%; 368/1615) was the most common site of injury; the thigh region (21%, 333/1615) was the second most common site of injury; and the ankle (18%, 290/1615) was the third most common site of injury where discrete injury tallies (by injury site) in studies were available.18–26 (online supplemental appendix S9).
Supplemental material
In football tournaments,28 using a medical attention injury definition, lower limb injuries accounted for 66% (248/380) of all injuries. The ankle (24%, 93/380) was the most common site of injury; the head, face and neck (grouped as one anatomical site) (17%, 68/380) was the second most common site of injury; and the thigh region (13%, 50/380) was the third most common site of injury. One study29 of tournament football utilised a time-loss injury definition where lower limb injuries accounted for 89% (16/18) of all injuries (knee; 22%, 4/16, lower leg; 22%, 4/16, thigh; 17%, 3/16, ankle; 17%, 3/16) (online supplemental appendix S9).
Type of injury
Ligament sprains were the most common type of injury in elite adult women’s football (34%, 617/1810), followed by muscle strains (27%, 482/1810) and blunt soft tissue trauma (contusions & haematomas) (21%, 387/1810). In domestic club football, ligament sprains (37%, 517/1413) were the most common type of injury, followed by muscle strains (31%, 441/1413) and blunt soft tissue trauma (contusions and haematomas) (15%, 214/1413). (online supplemental appendix S9).
In football tournaments, using a medical attention injury definition,28 blunt soft tissue trauma (contusions and haematomas) was the most common type of injury (44%, 165/378) followed by ligament sprains (25%, 96/378) and muscle strains (10%, 38/378) (online supplemental appendix S9). Blunt soft tissue trauma (42%, 8/19), ligament sprains (21%, 4/19) and muscle strains (16%, 3/19) were the most common types of injury in tournament football utilising a time-loss injury definition.29
Ankle ligament sprains (43%, 131/308) was the most common injury diagnosis, followed by quadriceps muscle strains (16%, 48/308) and knee ligament sprains (12%, 38/308) where available injury diagnosis data was gleaned from the following studies.20 22 25 28
Severity of injury
In domestic club football,18–21 23–27 moderate time loss injuries were most common (8–28 days, 34%, 559/1645), followed by mild injuries (3–7 days, 33%, 544/1645); severe injuries (>28 days, 18%, 298/1645); minimal injuries (1–3 days, 12%, 204/1645); slight injuries (zero days, 2%, 28/1645) and career ending injuries (0.7%, 12/1645) (online supplemental appendix S9).
In tournament football using a medical attention injury definition,28 78% (116/149) of injuries prevented participation in match or training for up to 1 week, followed by moderate injuries (8–28 days; 10%, 15/149) and severe injuries (>28 days; 6%, 9/149). Tournament football utilising a time-loss injury definition,29 minimal injuries (1–3 days; 10/18, 56%) were most common, followed by moderate injuries (>7, <28 days, 4/18, 22%) and slight (0 days, 3/18, 17%) and severe injuries (>28 days; 3/18, 22%). (online supplemental appendix S9)
Incidence proportion (first injury)
Eight studies18–21 23 24 27 30 related to domestic club football reported the number of players sustaining at least one injury. The incidence proportion ranged between 0.32 and 0.81. Thus, the estimated risk of sustaining at least one injury in a season ranged from 32% to 81%. Incidence proportion data for repeat, multiple injuries or injuries sustained during tournament football were not available within studies.
Meta-analysis
Incidence of injury: total, match and training
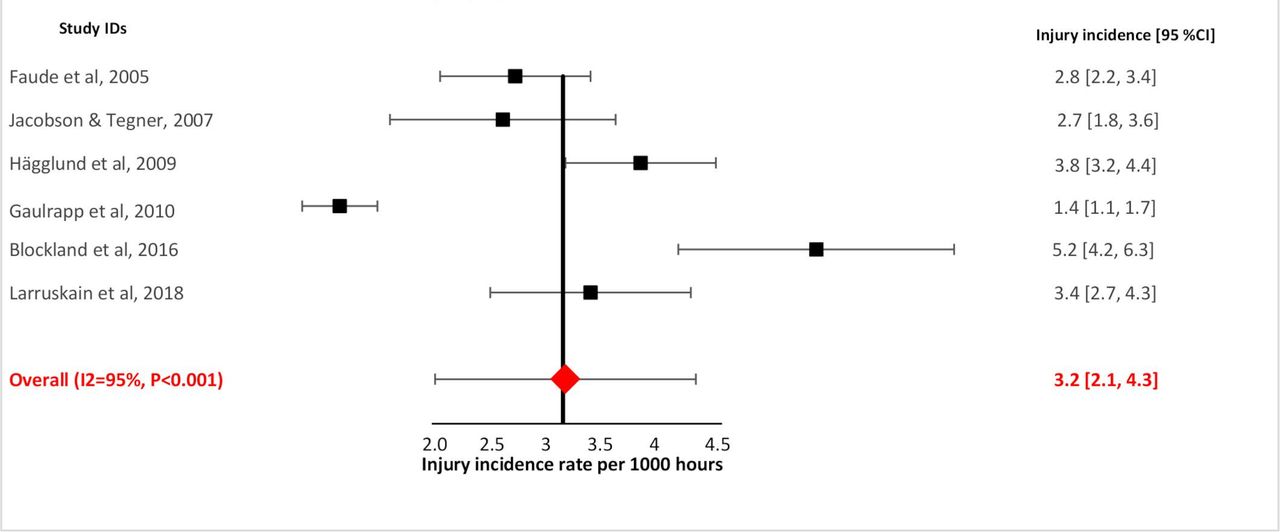
In domestic club football, the total incidence was estimated to be 5.7 injuries/1000 hours of exposure (95% CI 4.3 to 7.2, I2=95%) (figure 2),18 20 21 23–25 match incidence was 19.5 injuries/1000 hours (95% CI 16.2 to 22.8, I2=72%) (figure 3)18 20 21 23–25 and training incidence was 3.2 injuries/1000 hours of exposure (95% CI 2.1 to 4.3, I2=95%) (figure 4)18 20 21 23–25

Overall injury incidence rate: domestic club football.

Match injury incidence rate: domestic club football.
Training injury incidence rate: domestic club football.
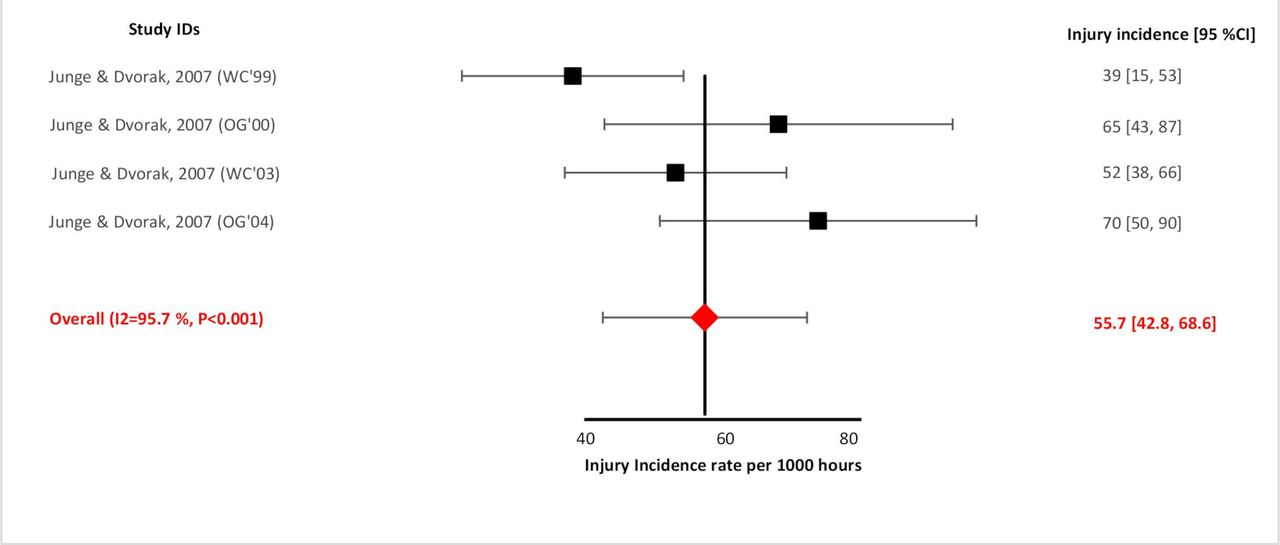
In football tournaments using a medical attention injury definition the match incidence was estimated to be 55.7 injuries/1000 hours of exposure (95% CI 42.8 to 68.6, I2=49.7%) (figure 5).28 There was insufficient data to provide a pooled estimate of match incidence from studies in tournament football utilising a time loss injury definition29 (table 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Match Injury Incidence: tournament football (using a medical attention injury definition).
Summary of findings table
Incidence proportion (first injury)
The average probability of any player sustaining at least one injury in a domestic club football season (incidence proportion) was 55% (95% CI 47% to 63%, I2=89%).18–24 27 There were insufficient data to provide incidence proportion estimates for repeat injuries, multiple injuries or injuries sustained during tournament football.
Discussion
This aim of our review was to provide a pooled estimate of the incidence of injury (overall, match and training) across adult elite women’s club football and tournament football and ascribe the nature and anatomical location of these injuries.
Injury incidence rate
In domestic club football, the total incidence rate found in our review (5.7/1000 hours, 95% CI 4.3 to 7.2, I2=95%) implies that elite adult women players have a rate of injury lower than that found in elite adult male football players (8.1/1000 hours, 95% CI 7.2 to 9.0, I2=99.1%).31 However, we remain cautious of point estimates presented due to high heterogeneity values found in both reviews. Furthermore, our review and a recent publication3 have not performed a direct comparison of pooled data extracted for men vs women, to prove the existence or otherwise, that any difference exists.
The injury incidence rate during tournament matches (55.7/1000 hours, 95% CI 42.8 to 68.6, I2=49.7%) was higher than that found in domestic club football matches (19.5/1000 hours, 16.2 to 22.8, I2=72%), followed by domestic club football training injury incidence (3.2/1000 hours, 95% CI 2.1 to 4.3, I2=95%). This descending injury incidence order reflects the same trend found in male elite football and reaffirms that in line with team sports (football,3 31 basketball,32 male handball,33 rugby34) match injury incidence rates are higher than training injury incidence rates in adult elite women’s football. Fatigue, physical demands and frequency of contact and collisions experienced during a competitive match are suggested to contribute towards the higher incidence found in male players.35–37 However, this might also be due to normal variation in the number of injuries reported due to chance and further investigations into how such variables affect the incidence of injury and illness in elite women’s players is warranted.
Our pooled incidence rate and 95% CI’s overlap with estimated rates found in a recent systematic review of injury profiling in women’s football (total, 6.1, 95% CI 4.6 to 7.7, I2=98.8%; training, 3.5, 95% CI 2.4 to 7.7, I2 97.7%; match, 19.2 95% CI 16.0 to 22.4, I2=94.2%).3 Differences in point estimates may be due to the sampling methods used in both reviews. For example, we contacted authors where data in studies was known to contain both amateur and elite-level data so we could exclude amateur rates and injuries tallies from our analysis. We excluded university and amateur level cohorts as well as grey literature (online supplemental appendix S4) while a previous review3 included them. The reference list of the review3 revealed two further studies; citation 553 was excluded as it was conducted via an accident and emergency hospital audit, and citation 573 was excluded as the incidence rate cited in the study referred to a non-footballing amateur cohort.
Recurrent injuries in sport are common and it is widely accepted that subsequent injury is strongly associated with previous injury occurrence. Our estimate of injury risk (incidence proportion) revealed that 55% of players sustained at least one injury in a season. However, it was unclear in studies whether injuries were specifically first injuries and how many were categorised as reinjuries or multiple reinjuries of the same or different anatomical site.
In domestic club football, the majority of injuries were of moderate severity (34%) (8–28 days), followed by mild (33%) (3–7 days), whereas in a recent systematic review and meta-analysis in elite male football players,31 minimal injuries (1–3 days) were most frequent, followed by mild injuries (3–7 days). A recent single site cohort study25 found elite women players experienced a greater number of moderate and severe injuries than their male counterparts with 21% more days lost in women than men. However, reinjury and multiple reinjury data were either not clearly presented or not available from studies to extract which limits the extent to which injury burden and injury severity (including the specific types of injuries) can be currently presented in adult elite women’s football.
I2 values exceeded 75% in our review and in a recent review of women’s football injury profiling3 and thus significant heterogeneity exists between the studies available. Consequently, in our review no further meta analytical pooling of data was conducted.38 39 Climatic playing conditions (cooler and warmer climates),40 match fixture congestion,41 42 frequency of matches played, mid-season breaks43 and levels of professionalism44 are factors that have been reported as potential sources of methodological heterogeneity found in male elite football literature. Whether incidence rates are moderated by these factors through meta-analysis currently remains unknown as this data was not readily extractable from the studies available. We wish to be judicious in interpreting the results from this review and highlight areas of inconsistencies in injury terminology, data collection procedures and calculations of exposure which might explain the high heterogeneity found and furthermore, make recommendations for future work.
Evaluating injury terminology
In our review studies applied either a time loss definition, an ‘any physical complaint’ or medical attention injury definition (online supplemental table S5), where the choice of vocabulary used in these injury definition statements varied. Differences might stem from the specific context from which statements were developed45 or, is a result of the diverse vocabulary and/or grammatical variation that exists.46 Adopting illness and injury definitions that embrace a broad array of injury-related and illness related health problems45 that may affect a player is worthy of consideration in future epidemiological research in women’s football.
An update on the consensus statement of injury and illness definitions currently used in football47 is required so that it can acknowledge specific urogenital/gynaecological female/women injury and illness symptom clusters. Specifically, these might include; loss of normal menstruation, irregular or infrequent menstruation, menstrual cramps/pain and excessively long periods recently highlighted in the 2020 International Olympic Committee Consensus Statement45 as required women-specific medical issues for recording and reporting of epidemiological data on injury and illness in sport.
Previous meta-analyses34 48 have attributed heterogeneous estimates of injury incidence to the inconsistencies in injury definitions and severity descriptors applied within studies. Studies in this review used inconsistent injury severity classification descriptors. Some studies19–21 26 27 applied three severity categories (mild, moderate, severe) and others applied four23–25 (minimal, mild, moderate, severe) or five18 severity categories (minimal, slight, mild, moderate, major). Subgroup meta-analyses on injury site and injury type data was not possible in adult elite women cohorts (without threating contaminating data) as the temporal measure assigned (time/days lost) within each descriptor was inconsistent across studies.
It is recommended that future studies adopt a consistent and clear categorisation of a first injury, reinjury and multiple reinjury of the same or different type, identify the underlying mechanisms as well as ensuring consistent terminology is used before subsequent estimates of injury burden can be made.
Data collection and evaluating data processing
To provide estimates of the extent of injury burden, capturing and evaluating training and match exposure consistently and accurately within sport is fundament to quantifying injury risk. The athletes at risk (AAR) method14 has been recommended within injury consensus statements (football,47 rugby union49) when individual level exposure is not possible or is deemed to be over cumbersome.14 The AAR method recommends the multiplication of the number of players on the field (football=11 players) by the number of games or game-hours the team has played (football=90 min=1.5 hours), divided by the number of injuries sustained in a given period (match / season).
Recent systematic reviews and meta-analyses3 31 34 48 50 have employed this method to provide estimates of injury incidence (prior to meta-analysis) when rates and precision estimates are not reported within individual studies. It is recommended that when estimating injury incidence using this method, events which reduce the number of players on a team (eg, red card) for part of a game (this would over-estimate exposure time), and, events which would underestimate exposure time if games exceeded 90 min (eg, injury time, extratime, penalty kicks) are taken into account.14
While the findings of these reviews3 31 34 48 50 provide current estimates of injury burden, they do not provide an explanation or the methodological steps taken to mitigate against errors in reporting of exposure using this approach. This method only replicates results of individual-level exposure time calculations when training and games are played with a consistent number of players under consistent exposure conditions.14 Injury rate estimates that have been calculated in this way, without due consideration or notification of such exposure-time reporting errors lead to bias in incidence reporting.51 The International Olympic Committee consensus statement on reporting epidemiological data on illness and injury in sport currently recommend injury rates to calculated by using individual level data for injuries and exposure rather than team-level estimates.45
Limitations
The full extent of injury burden could not be obtained from our meta-analysis which we feel was due to several methodological inconsistencies of available studies. We chose not to undertake subgroup meta-analyses of incidence of injury by anatomical site or tissue and so the findings (to this degree) cannot be compared with findings from a meta-analysis in male elite football.31 Some studies reported multiple seasons or tournaments and while we were prudent in removing duplicate data sets to avoid double counts, we could only extract the incidence data that was available. If studies have not reported or accounted for all individual injury counts, double counting of injuries may have occurred. Our aim was to retrieve data from adult elite players aged eighteen years and older and while we were diligent in data extraction, there is a small risk that players under eighteen may have been sampled. We amended our PROSPERO registration to include a definition of ‘elite’ football, replacing the term ‘soccer’ with ‘football’ and the addition of the NOS for risk of bias assessment.
We chose not to employ ARR methods to estimate injury incidence at a team level. This may have resulted in us not capturing all available data sets and studies. This limits the ability for us to provide full evaluations of injury burden. However, we feel this decision was justifiable as we wanted to remain cautious of limiting the ecological fallacy that arises when aggregate or team-level data fails to properly reflect individual level exposure data.52 Furthermore, due to the considerable heterogeneity, recommendations are that further pooling of data should be avoided and definitive conclusions drawn when more studies become available.39
Conclusions
This meta-analysis found that the rate of injury in adult elite women’s football is lower to that found in elite male football. Caution is needed when interpreting these estimates due to the high heterogeneity values. We have greater confidence in the findings relating to injury site and type, where the lower extremities including the knee, thigh and ankle were commonly injured. Our injury tallies identify ligament injuries occur more frequently in adult elite women football players, followed by muscle injuries. Future studies must make a concerted effort to standardise injury and illness definitions, medical reporting and clear and accurate recording of match and training exposure in women’s football is needed.
Ethics statements
Ethics approval
Research Ethics Committee of Leeds Beckett University.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @mayhewlawrence
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests In the previous 5 years MIJ’s institution has received research and consultancy funding for work that he has undertaken for GlaxoSmithKline, Medi-Direct International and TENScare.
Provenance and peer review Not commissioned; externally peer reviewed.