Article Text

Abstract
Objective To assess the diagnostic accuracy of antigen compared with reverse transcriptase (RT)-PCR testing in an asymptomatic athlete screening programme and to monitor infection in college athletes.
Methods Quidel Sofia-2 SARS-CoV-2 Antigen Tests were performed daily before sports participation for football, basketball, wrestling and water polo from 29 September 2020 to 28 February 2021. Paired RT-PCR and antigen tests were performed at least once a week. Positive antigen tests were confirmed with RT-PCR.
Results 81 175 antigen and 42 187 RT-PCR tests were performed, including 23 462 weekly paired antigen/RT-PCR screening tests in 1931 athletes. One hundred and seventy-two athletes had a positive screening RT-PCR (0.4%), of which 83 (48%) occurred on paired testing days. The sensitivity of antigen tests varied with the frequency of RT-PCR testing and prevalence of COVID-19. The sensitivity of antigen testing was 35.7% (95% CI: 17% to 60%) and specificity 99.8% (95% CI: 99.7% to 99.9%) with once-a-week RT-PCR testing after adjusting for school prevalence. Daily antigen testing was similar to RT-PCR testing two to three times a week in identifying infection. Antigen testing identified infection before the next scheduled PCR on 89 occasions and resulted in 234 days where potentially infectious athletes were isolated before they would have been isolated with RT-PCR testing alone. Two athletic-related outbreaks occurred; 86% of total infections were community acquired.
Conclusion Antigen testing has high specificity with a short turnaround time but is not as sensitive as RT-PCR. Daily antigen testing or RT-PCR testing two to three times a week is similar. There are benefits and drawbacks to each testing approach.
- athlete
- COVID-19
- infection
Data availability statement
Data are available upon reasonable request. Data is from the Pac-12 Health Analytics Program and is subject to the terms of the data use agreement. Reasonable request to the authors will be accommodated as allowed.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known?
Reverse transcriptase (RT)-PCR is more sensitive than antigen testing for the detection of SARS-CoV-2.
Antigen testing can return a rapid result, leading to immediate isolation of an infected individual.
There is debate regarding the most effective surveillance testing strategy and the trade-off between sensitivity and the turnaround time of the test.
What are the new findings?
Antigen testing is highly specific, even in an asymptomatic low-risk population.
The sensitivity of antigen testing compared with RT-PCR is 35.7%. However, there were 234 days when athletes were isolated before they would have been with scheduled RT-PCR alone.
Daily screening tests alone did not prevent outbreaks, indicating the need for continued physical distancing and mitigation measures.
Introduction
SARS-CoV-2, the aetiologic agent of COVID-19, spread globally, causing widespread disruption to society. Maintaining physical distance from others and the use of masks are critical to combat the spread of COVID-19. However, this is often impossible in sport. A strategy that employs frequent testing for COVID-19 in asymptomatic populations has been proposed to detect and remove potentially infectious persons from environments where transmission may occur.1 2 These include occupational settings, schools and sport, especially those sports where there is close physical contact, face-to-face interactions and those which occur indoors.
Reverse transcriptase (RT)-PCR is the reference standard for testing for SARS-CoV-2 and can detect low levels of the virus. However, the tests are expensive and must be performed in a high-complexity laboratory with turnaround times typically 1–2 days (or longer). When test results are pending in a clinical setting, a patient with COVID-19 symptoms is isolated and high-risk contacts are quarantined until results return. When screening an asymptomatic population, such as occurs in sport, the individual continues to participate and is isolated only when a test result is returned positive. In such a scenario, if an RT-PCR test result is positive, that individual may have been infectious while awaiting test results and may have exposed others during that time.
Antigen tests have been proposed as screening tests in asymptomatic persons who will undertake activities that pose a high risk of transmission (HROT) for SARS-CoV-2. Antigen tests are less sensitive than RT-PCR tests but have a rapid turnaround time (15 min to hours) to isolate the infected person immediately. Antigen tests are less expensive than RT-PCR and do not require a high-complexity laboratory, making it possible to test more frequently. The trade-off between the test’s sensitivity and turnaround time of results has caused debate regarding the optimal type and frequency of testing in an asymptomatic population.
The Centers for Disease Control and Prevention (CDC) estimates that up to 90% of infections are spread before the development of symptoms.3 One mathematical model forecasts a decrease in infectiousness based on the test’s sensitivity and turnaround time and estimates that nearly 100% of infectious individuals will be immediately identified and isolated with daily antigen testing.1 The purpose of this study was to follow a large population of athletes in HROT sports participating in a screening programme and describe patterns of infection and the screening programme results.
Methods
Eleven of twelve Pac-12 schools participated in the study. The school not participating did not have its medical record integrated with the Pac-12 Health Analytics Program (HAP) at the time of data acquisition. All athletes included in the study provided consent for their data to be included in the HAP. All tests for SARS-CoV-2 were recorded, including those done for reasons other than screening. Reasons for testing included tests done when athletes returned to campus after a time away (initial or re-entry screening), tests of high-risk contacts (contact tracing), tests done if an athlete had symptoms (symptomatic) and screening tests (screening).
Pac-12 athletes engaging in HROT sports (football, basketball, water polo and wrestling) had daily screening tests using the Quidel SARS-CoV-2 Antigen Test (Quidel, San Diego, California, USA) on days where HROT activities occurred. HROT activities typically occurred 6 days a week; the National Collegiate Athletic Association (NCAA) requires at least 1 day a week without athletic-related activity. Athletes were also tested at least once a week with a screening RT-PCR paired with the daily antigen test. Institutions could elect to use screening test more frequently with RT-PCR but were required to continue the antigen testing protocol. A positive antigen test triggered confirmatory RT-PCR testing and removal of that athlete from all team activities pending PCR test results. If an athlete had a positive test, contact tracing was performed. High-risk contacts were determined by local public health authorities using case interview, and in some cases, review of practice or game film or proximity monitors. Test results were recorded prospectively and included in the Pac-12 HAP, a deidentified research database if the athlete had previously provided consent. Data were collected from 29 September 2020 to 28 February 2021. The study was considered exempt by the University of Washington Institutional Review Board. Data sharing agreements for data in the Pac-12 HAP were in place for all institutions.
COVID-19 testing procedures and definitions
The Quidel SARS-CoV-2 Antigen Test was performed using dry anterior nasal swabs as per the manufacturer’s instructions after standardised training by certified personnel at each institution. The institution’s reference laboratory performed RT-PCR tests. The institution used local collection protocols for RT-PCR tests, including nasopharyngeal swabs, anterior nasal swabs, nasal/oral swabs and/or saliva. If cycle threshold (Ct) values were available, these were entered into the record for positive tests. The RT-PCR test was considered as the reference test and the antigen test as the index test. The results of the index test were not known by those performing the reference test. In some cases, serial RT-PCRs or antigen tests were performed to confirm a positive. The repeat tests were removed from the database.
The days of infectiousness removed were calculated by counting the days from a positive antigen test to the day after the next screening RT-PCR test for a team (assuming 24 hours turnaround for RT-PCR). Finally, the number of athletic-related outbreaks was obtained from each school for each sport. An athletic-related outbreak was defined as at least three athletes on one team from different households testing positive due to athletic-related activity, which led to a halt in activity. Athletic-related activity encompasses all team activities, including time spent in the athletic facility for any reason (team meetings, team meals, locker room, athletic training room), team travel, conditioning, practices or games. The number of occasions of one team transmitting the virus to an opponent’s team during the competition was also obtained. In all cases, schools were subject to their local public health authority regulations, and activity may have been suspended because of contact tracing or to prevent spread.
Statistical approach
Standard descriptive statistics were used, specifically frequencies, percentage, means and SD, to describe the athlete population and diagnostic testing results. As RT-PCR tests are currently considered the gold standard,4 overall and group-specific prevalence was estimated as the percentage of athletes with a positive RT-PCR test during the study period. Sensitivity and specificity were estimated on the subgroup of antigen and PCR tests conducted on the same day (paired) to minimise time bias in the detection of SARS-CoV-2. To account for multiple tests being conducted on the same athletes, generalised estimating equations (GEE) were used to account for correlated observations. Moreover, because sensitivity and specificity are affected by prevalence in the population, estimates were adjusted for prevalence by the school in the GEE model. Adjusted estimates and 95% CIs are reported. Blank, invalid, inconclusive and repeat tests on the same day were excluded from the final data analysis. SAS V.9.4 (SAS Institutes) was used for all analyses.
Patient and public involvement
There was no patient or public involvement in this study.
Data sharing
The data used for this study are contained in the Pac-12 HAP. They are accessible to Pac-12-affiliated investigators for research projects, pending the submission and approval of the Pac-12 data request application.
Results
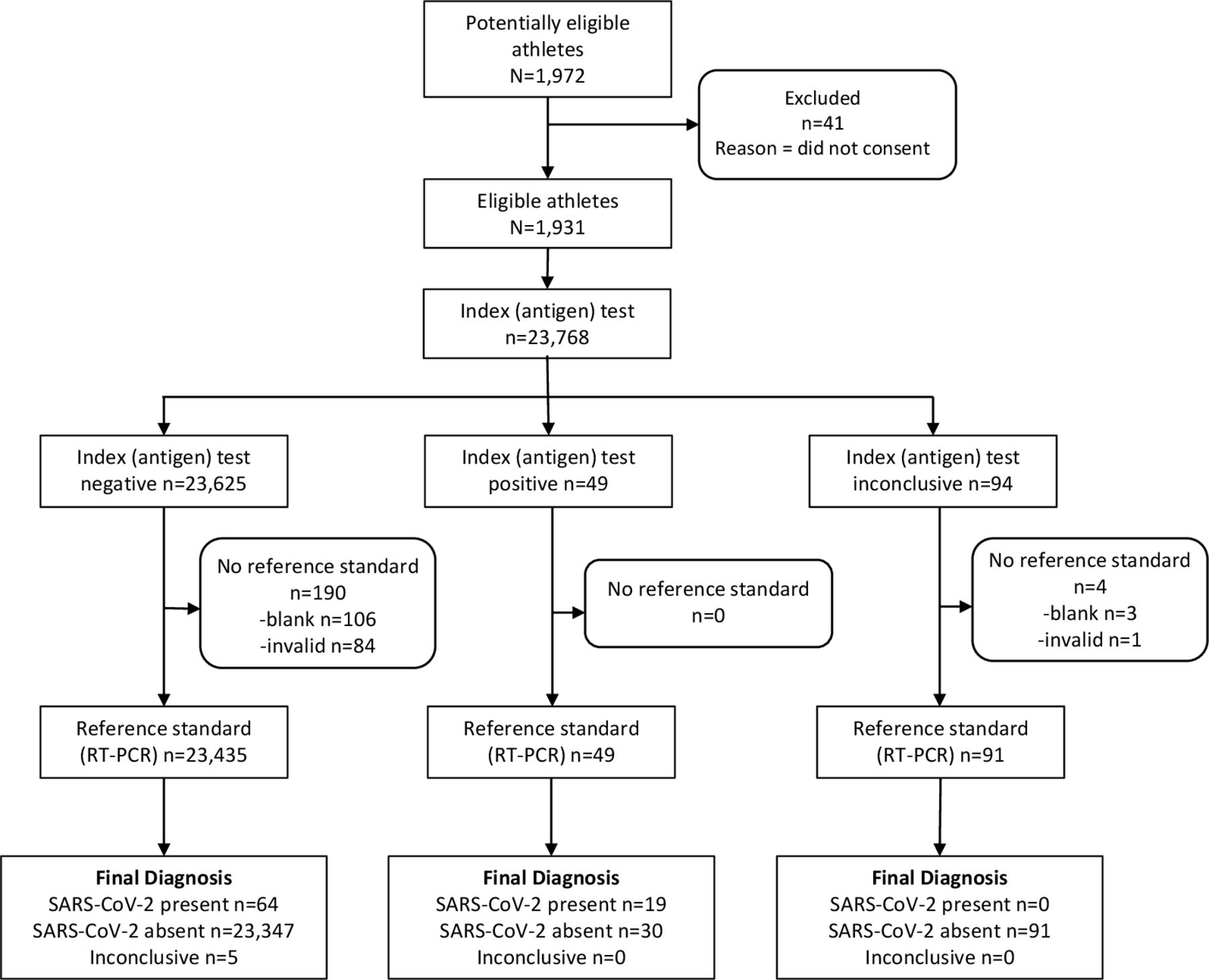
There were 1972 athletes potentially eligible for the study, and 1931 (97.9%) participated (figure 1). HROT sports included football, women’s basketball, men’s basketball, women’s water polo, men’s water polo and wrestling (table 1).
Demographics and percent positivity of reverse transcriptase-PCR of study population

{kind=link}
Study flow chart. RT, reverse transcriptase.
There were 42 187 PCR tests performed. PCR tests were performed for initial/re-entry screening (when returning from non-team-related time away from athletics), contact tracing (on an athlete who was deemed to be a high-risk contact as defined by local public health authorities) if an athlete was symptomatic, or for screening (table 2).
Percent positivity of reverse transcriptase (RT)-PCR testing for different indications
Diagnostic accuracy
There were 81 175 antigen tests performed, and 23 462 antigen tests had corresponding RT-PCR screening tests performed on the same day (paired). Eighty-three positive RT-PCRs were reported on paired testing days. The clinical sensitivity of antigen tests varied with the frequency of RT-PCR testing. Overall clinical sensitivity and specificity estimates, adjusted for school prevalence, were 22.9% (95% CI: 15.1% to 33.2%) and 99.87% (95% CI: 99.81% to 99.91%), respectively. When considering only those athletes undergoing PCR testing once a week (in addition to daily antigen testing), the clinical sensitivity was 35.7% (95% CI: 22.8% to 51.1%) and specificity 99.83% (95% CI: 99.73% to 99.89%) after adjusting for prevalence. There were 5086 (21.7%) paired antigen/RT-PCR tests where RT-PCR testing was performed at least four times a week. There were no true-positive antigen tests in this group. (table 3).
Diagnostic accuracy of same-day antigen and reverse transcriptase (RT)-PCR testing based on the frequency of PCR testing.
Only 2 of the 19 true-positive antigen tests had Ct values for the corresponding PCR (16.1 and 23.1). Twenty-four of the sixty-four false-negative antigen tests (37.5%) had corresponding RT-PCR tests with Ct values. The average Ct value for the false-negative antigen tests was 30.0 (SD: 5.66, range 20.0–38.1).
Screening tests
A total of 172 athletes with SARS-CoV-2 infection were identified by the screening testing programme, including tests occurring on paired and antigen-only testing days. Overall, 89 of the 172 athletes (52%) were detected by antigen testing on non-paired testing days and isolated before when they would have been identified by RT-PCR alone. True-positive antigen screening tests on non-paired days prevented 234 athlete days of potential infectiousness. Antigen testing generally halted once a positive diagnosis was made. However, there were seven instances where an RT-PCR test was positive and the antigen negative, but the RT-PCR result was not available before the next day’s antigen testing. The next-day antigen testing was positive in these cases, suggesting that antigen testing positivity lags about a day behind PCR. During the same period, there were 98 false-positive antigen tests. Those athletes were isolated and then allowed to return to activity if no symptoms had developed and subsequent RT-PCR test/s were negative. Despite the aggressive testing programme, there were two athletic-related outbreaks at two different schools among the 11 participating Pac-12 schools during the study period. Both outbreaks occurred in football were related to not following COVID-19 protocols, and resulted in 48 (13.8%) of the 346 cases that occurred during the study period. There were no known cases of team to opponent team spread during competition. There were nine schools that did not have an outbreak in any sport.
Discussion
We describe the results of a massive, largely successful testing programme in an asymptomatic population of division I collegiate athletes. Several conclusions may be drawn from this experience. First, the Quidel Sophia-2 SARS-CoV-2 Antigen Test is highly specific. Second, daily antigen testing is roughly equivalent to testing with RT-PCR two to three times a week in the ability to identify athletes infected with SARS-CoV-2. Whether two or three times a week RT-PCR testing is equivalent depends on the local prevalence of SARS-CoV-2. Third, If RT-PCR testing four times a week or more, there is no added value in antigen testing. Fourth, as expected, antigen tests detect the SARS-CoV-2 virus at a higher viral load (lower Ct value). From limited evidence, it appears antigen positivity lags a day behind RT-PCR positivity. Finally, there were a few outbreaks among schools, emphasising the continued need for masks, physical distancing and contact tracing after a positive case, even with a rigorous screening testing programme.
This study is consistent with others that show antigen testing to be highly specific.5–8 In a low-prevalence setting, false positives (n=98) occurred at a similar frequency as true positives (n=83) but did not cause significant disruption to programmes. The exception was antigen testing on game day and the concern of a false positive removing players or causing event cancellation. When possible, rapid RT-PCR was available for confirmation on game days. Although the sensitivity may appear low at first glance, this is not unexpected given our population and the nature of a serial testing programme. The performance of a test is dependent on pretest probability. Even once a week, RT-PCR removes individuals with lower viral loads than can be detected by antigen tests from the testing pool. This effect was more pronounced with more frequent RT-PCR testing. There were no positive antigen tests when testing with RT-PCR four times a week or more. It is notable that with antigen testing, athletes were isolated before the next PCR test on 89 occasions, resulting in at least 234 days where infectious athletes were restricted from HROT activities due to isolation, preventing potential spread. This calculation assumed 48 hours turnaround of the confirmatory RT-PCR and if turnaround times were more prolonged the number would be higher.
Other studies in asymptomatic populations show similar results. In one study on a college campus screening programme using 871 paired swabs in asymptomatic persons, Quidel Sophia SARS CoV-2 Antigen testing had a sensitivity of 41.2% and specificity of 98.4%.7 That study did not control how many times a week an individual was being screened or if individuals had repeated observations. It would be expected that those presenting to a community testing site, even if asymptomatic, would have a higher pretest probability of a positive test compared with those in a serial testing programme, as many will be seeking a test because of specific concern for infection such as a high-risk contact. A study at a community testing site in Arizona using BinaxNOW estimated the sensitivity to be 35.8% in asymptomatic individuals. A similar study at a community testing programme in Massachusetts demonstrated a sensitivity of 70.7% in asymptomatic persons.6 BinaxNOW has a limit of detection of 40 000–80 000 copies/swab, which corresponds to a Ct value of 29–30, which is similar to laboratory-based studies of the Quidel Sophia-2 SARS-CoV-2 Antigen Test.9
This study demonstrates that there are several reasonable options for a screening testing programme depending on available resources. In areas where the cost or access to RT-PCR is prohibitive, antigen testing is a good alternative. In addition, there were several cases where next-day antigen testing results were positive before the previous day RT-PCR results were available. If the turnaround time for RT-PCR testing is more than 24 hours, antigen testing could result in earlier isolation of asymptomatic infectious individuals. As infection rates decline and vaccination rates increase, the utility of screening tests should be re-evaluated. Only 0.4% of the screening testing were positive in this study during the height of the pandemic. Future screening should be dependent on local prevalence, vaccination status of the school and community and should vaccine resistant variants arise.
Despite aggressive testing programmes, outbreaks did occur. Eighty-six percent of COVID-19 cases in the student-athlete population were community-acquired (outside the athletic footprint). However, outbreaks within the footprint did occur even in a school that was testing up to six times a week with RT-PCR and daily antigen testing. This illustrates that even the most rigorous testing programme will not catch all cases before they are infectious and demonstrates the need for continued masking and social distancing when possible and contact tracing when there is a positive result. In some cases, there may have been a perception that daily testing assured non-infectiousness, which may have led to breaches in COVID-19 protocols. This is consistent with the experience of other conferences where daily testing (antigen or RT-PCR) alone did not prevent outbreaks.10 11 There were several limitations to this study. We considered the RT-PCR test to be the gold-standard test, but false-negative and false-positive RT-PCR tests can occur.12 In addition, there were multiple RT-PCR assays in use at the different sites, which have different limits of detection.13 The samples for the RT-PCR tests were collected in various ways, although nasal, nasopharyngeal and saliva collection methods are roughly equivalent in studies.14 Although we present the available Ct values for true-positive and false-negative antigen tests, Ct values differ from assay to assay and by specimen type and should be considered in a qualitative context. Finally, the testing programme required a considerable effort on the part of the medical staff at each institution and may not be reproducible in other settings with fewer resources.
Conclusion
College athletes can engage in HROT sports safely with robust testing programmes. Outbreaks were limited, and there was no evidence of viral spread from an athlete on one team to an athlete on another team. This large-scale study demonstrates that several different screening testing strategies can be effective, but none alleviate the need for COVID-19 mitigation measures. There is a trade-off between sensitivity and turnaround time with currently available testing options for SARS-CoV-2. Daily antigen testing is comparable to RT-PCR testing two to three times a week in identifying SARS-CoV-2 infection in athletes depending on local prevalence. Although antigen testing is less sensitive than RT-PCR, it enabled isolation of potentially infectious athletes before when they would have been identified with RT-PCR in 89 cases accounting for 234 days. Antigen testing may be considered when RT-PCR testing has >24-hour turnaround time. This study demonstrates the real-world outcomes of proposed screening testing strategies and can inform decision-making in other settings.
Data availability statement
Data are available upon reasonable request. Data is from the Pac-12 Health Analytics Program and is subject to the terms of the data use agreement. Reasonable request to the authors will be accommodated as allowed.
Ethics statements
Acknowledgments
This publication contains material created, compiled or produced by the Pac-12 Health Analytics Program (HAP). We thank the many athletic department staff, most importantly the athletic trainers who have submitted data to the HAP.
Footnotes
Twitter @DrKimHarmon
Collaborators Kevin Robell; Michael L Dillon, Heather Elkington, John Swartzberg.
Contributors All authors contributed to the design of the study, collection of data, and review and revision of the manuscript. In addition, KH, DFA and SAK were responsible for data analysis and manuscript preparation.
Funding This study was funded by a research grant from Quidel. The funder agreed to the objectives of the study but had no role in study design, collection, analysis, or interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Competing interests KH has stock options in 98point6 which are not relevant to this paper.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.