Article Text

Abstract
Sport-related concussion has garnered increasing scientific attention and research over the last decade. Collegiate student-athletes represent an important cohort in this field. As such, the Pac-12 CARE-Affiliated Program (CAP) was formed in 2017 as a regional hub of the Concussion Assessment, Research and Education (CARE) consortium. CAP is multisite, prospective, longitudinal study that aims to improve student-athlete health by identifying factors associated with concussion incidence and recovery and using this knowledge to inform best clinical practices and policy decisions. CAP employed a staggered rollout across the Pac-12, with the first four institutions enrolling in fall 2018. After receiving institutional review board (IRB) approval, these institutions began consenting student-athletes to share clinical concussion and baseline data for research purposes. Athletes completed baseline testing that included a medical questionnaire, concussion history and a battery for clinical concussion assessments. Concussed student-athletes were given the same battery of assessments in addition to full injury and return to play reports. Clinicians at each university worked with a data coordinator to ensure appropriate reporting, and the Pac-12 Concussion Coordinating Unit at the University of Colorado Boulder provided oversight for quality control of the data study wide. During year 1, CAP consented 2181 student-athletes and tracked 140 concussions. All research was conducted with the appropriate IRB approval across the participating Pac-12 institutions. Data security and dissemination are managed by the Presagia Sports Athlete Electronic Health Record software (Montreal, Quebec, Canada) and QuesGen Systems (San Francisco, California, USA).
- concussion
- injury
- sport
Data availability statement
Data are available upon reasonable request. Data security and dissemination are managed by the Presagia Sports Athlete Electronic Health Record software (Montreal, Quebec, Canada) and QuesGen Systems (San Francisco, California, USA).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known
Sport-related concussion is common among collegiate student-athletes, with the highest burden of concussion in wrestling, men’s and women’s hockey and football.
What are the new findings
Are there sport, sex or injury circumstance differences in initial symptomology and symptom recovery from concussion?
What patient characteristics are predictive of recovery time from concussion in collegiate student-athletes?
Are there novel concussion assessments that can aid in the diagnosis of concussion?
Introduction
Over the past decade, there has been a growing scientific interest and public concern over sport-related concussion (SRC) across the world. SRC is a relatively common injury associated with organised sports and recreational activities.1 2 Among National Collegiate Athletic Association (NCAA) student-athletes, the overall incidence rate of concussion is estimated to be 4.47 per 10 000 athlete-exposures (AEs) with a slight majority (~53%) occurring during competitions.3 Concussion rates vary by sport with the highest rates (per AE) found in men’s wrestling, men’s and women’s ice hockey, and men’s football.3 While substantial progress has been made over the past 20–30 years in the elucidation of factors underlying the mechanisms of SRC and recovery from SRC, there remain critical gaps in our knowledge and evidence base to guide future policy decisions and clinical best practices.
To address some of these gaps, in 2014 the NCAA in collaboration with Department of Defense (DoD) established the NCAA-DoD Concussion Assessment, Research and Education Consortium (NCAA-DoD CARE Consortium).4 This large-scale effort includes over 30 universities and US service academies with the goal of defining the natural history of concussion by collecting core common data elements across sites. Indiana University serves as the Administrative and Operations Core, and the University of Michigan leads the Longitudinal Clinical Study Core.
Also in 2014, the Pac-12 Conference (http://www.pac12.com) established the Student-Athlete Health and Well-Being Initiative (SAHWBI) (https://pac-12.com/conference/sahwbgp) uniting all Pac-12 universities in an organised, structured scientific collaboration. The Pac-12 Conference is comprised of the University of Arizona (UA; Tuscon, Arizona), Arizona State University (ASU; Tempe, Arizona), University of California, Berkeley (UCB or ‘Cal’; Berkeley, California), University of Colorado Boulder (CU; Boulder, Colorado), University of Oregon (UO; Eugene, Oregon), Oregon State University (OSU; Corvallis, Oregon), Stanford University (Stanford; Palo Alto, California), University of California (UCLA; Los Angeles, California), University of Southern California (USC; Los Angeles, California), University of Utah (UU; Salt Lake City, Utah), University of Washington (UW, Seattle, Washington) and Washington State University (WSU, Pullman, Washington). The Pac-12 SAHWBI, funded by mutual contributions from each of the Pac-12 universities, serves as the primary platform for all research activities involving Pac-12 student-athletes. In the first year of this initiative, the Pac-12 established the Health Analytics Program (HAP; formerly SIRMAP) that serves as the primary sports injury registry and database for the conference.
Recognising the substantial overlap in common goals of both the NCAA-DoD CARE Consortium and the Pac-12 SAHWBI, including the potential for significant future collaboration through concussion research-advances, in August 2017 the Pac-12 collectively became a CARE-Affiliated Program (CAP)—effectively serving as a ‘regional hub’ for the CARE Consortium. The Pac-12 CAP shares many of the elements of the parent CARE Consortium—it is a multisite, prospective, longitudinal initiative to study the natural history of concussion with a focus on clinical and neurobiological recovery. The aims of the Pac-12 CAP are therefore aligned with the NCAA-DoD CARE Consortium. These aims include the identification of factors associated with concussion incidence and recovery with a fundamental goal of establishing a framework for evidence-based policy decisions and best practices. Most importantly, the Pac-12 CAP aims to improve the health and well-being of its student-athletes. Finally, the Pac-12 CAP could serve as a model for other conference-wide concussion surveillance programmes. Here, we describe the structure, organisation and methods of the Pac-12 CAP in addition to providing descriptive results of the study from year 1 of data collection (1 July 2018–30 June 2019).
Methods and analysis
Organisational structure
The Pac-12 CAP operates under the scientific and clinical oversight of the Pac-12 Brain Trauma Task Force (BTTF), which is comprised of six physicians and one head athletic trainer from across the Pac-12 and is currently chaired by SKP (CU). In addition to providing oversight to CAP, the BTTF advises the Pac-12 Student-Athlete Health and Well-Being Board on issues related to brain health, injury risk, injury trends, and emerging technologies. Data collection, quality assurance, and quality control activities as well as establishing best practices among the research institutions are implemented by the Pac-12 Concussion Coordinating Unit (PCCU) which is currently housed at the CU under the direction of MBM.
The Pac-12 CAP has adopted a staggered rollout for onboarding institutions into the study (see table 1). Over a 3-year period, four institutions are enrolled corresponding to the following data collection cycles: (1) Year 1: 1 July 2018–30 June 2019, (2) Year 2: 1 July 2019–30 June 2020, (3) Year 3: 1 July 2020–30 June 2021. During the initial enrollment year, institutions are requested to enroll student-athletes from a minimum of seven NCAA sports. During the second year of participation in the study, institutions are requested to expand enrolment to at least 14 NCAA sports, and eventually up to all NCAA sports by the third year of participation.
Data collection schedule for Pac-12 institutions
Upon on-boarding into the study, each institution hires an on-site data coordinator and identifies the initial seven NCAA sports to be enrolled. All data coordinators have extensive experience in either research or athletic training. During the on-boarding process, data coordinators receive training in the EYE-SYNC application, the Presagia Sports Athlete Electronic Health Record software (Montreal, Quebec, Canada), and the CAP protocol. In addition, data coordinators receive assistance in drafting both their site internal review board protocol and informed consent from the PCCU. Finally, data coordinators are required to complete Collaborative Institutional Training Initiative (CITI) Human Subjects Research training. On-site data coordinators are responsible for: (1) working with the principal investigators at the PCCU to coordinate and obtain study approval from their institutional review board (IRB), (2) coordinating with athletic trainers and team physicians to obtain informed consent from student-athletes, (3) overseeing the collection of baseline assessment, demographic and medical history data from athletes on all enrolled teams, (4) coordinating the collection of data on incident concussions and follow-up assessments and (5) working with the project coordinator at the PCCU on ensuring data quality and completeness.
Common data elements: baseline measures
Baseline assessments are collected during a time period outside of organised participation in NCAA sport (ie, summer, off-season). During baseline data collection, participants complete questionnaires on demographic information, medical history, and concussion history for previous sport-related concussions. The concussion history form includes questions on the cause of the concussion (sport vs non-sport), if the concussion was diagnosed, whether the student-athlete suffered loss of consciousness or post-traumatic amnesia and for how long, and the number of days the student-athlete experienced symptoms. Participants also complete the Sport Concussion Assessment Tool 5 (SCAT5) Symptom Evaluation,5 the Standard Assessment of Concussion (SAC),6 the modified Balance Error Scoring System (mBESS),7 8 the Brief Symptom Inventory 18 (BSI-18),9 the EYE-SYNC Smooth Pursuit test,10 11 and a cognitive assessment such as the Immediate Post-Concussion Assessment and Cognitive Test.12 13 The SAC assessments use the 5-word list for consistency with CARE. However, at time of publication, sites have the option of using the 5-word or 10-word list. The SAC assessment does not include the exertional component. The BESS assessment measures firm surface only. See table 2 for details on baseline assessments.
Common data elements at baseline and post-injury
Common data elements: concussion incident
Concussion diagnoses are made by a team of medical practitioners through the standard clinical care at each institution. Student-athletes (irrespective of study participation) presenting with symptoms consistent with a concussion are evaluated using a series of standardised assessments focused on reported symptoms, neurological status, postural stability, and oculomotor and vestibular domains. Additionally, following a concussion, athletic trainers and data coordinators complete a concussion incident form describing various elements of the injury, including the mechanism of injury, impact location, what the athlete collided with, if the injury occurred during practice or competition, the playing surface, loss of consciousness or post-traumatic amnesia, and if the athlete was immediately removed and eventually returned to play. Within 48 hours of the athlete sustaining the concussion, the injured athlete completes the SCAT5 symptom evaluation, mBESS, SAC, and Smooth Pursuit. The athlete then completes the SCAT5 symptom evaluation daily until asymptomatic. Within 24 hours of being cleared to the Return to Play (RTP) protocol, the athlete completes the SCAT5 symptom evaluation, mBESS, SAC, Smooth Pursuit, and a cognitive assessment. Within 24 hours of completing the RTP protocol, the athlete completes the Smooth Pursuit and BSI-18. Finally, a report is completed by the primary clinician that includes general clinical impressions of diagnosis, recovery trajectory, and the student-athlete’s return to academic and athletic activities. All follow-up assessments followed the same structure of baseline assessments with the exception of changing the specific word list used for SAC at each of the time points. See table 2 for details on the timing of post-injury assessments.
Participant (patient) involvement
Though all student-athletes receive the same clinical care at their respective institutions during the course of the study whether they agree to participate in the Pac-12 CAP or not, only those that consent to have their clinical information shared for research purposes are enrolled in the Pac-12 CAP study. IRB-approved consenting methods include paper consents by a CITI-trained data coordinator, athletic trainer, or other clinical provider as well as electronically deployed consent via the study data were collected and managed using REDCap electronic data capture tools hosted at the CU.14 15 REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources. Student-athletes are typically recruited to participate in the study during a baseline period which may include freshman athletic orientation events, pre-participation physicals and team meetings. Participation in the Pac-12 CAP is entirely voluntary, and student-athletes are not compensated for their participation.
Data flow
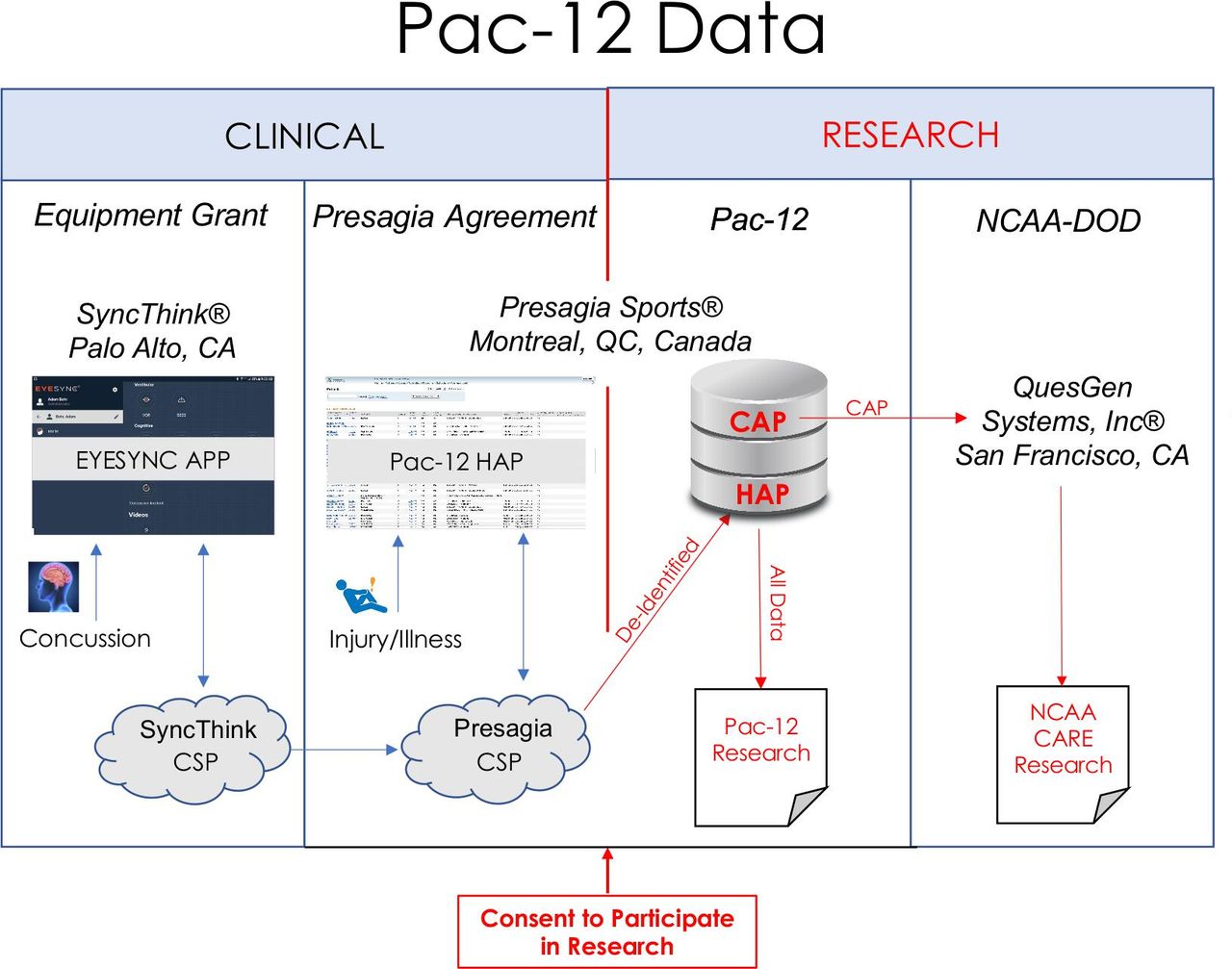
During the first 3 years of the Pac-12 CAP, all baseline, incident and follow-up data are entered into a tablet-based EYE-SYNC application designed by SyncThink to capture the common data elements in addition to oculomotor and vestibular measures (ie, Smooth Pursuit) through a virtual-reality headset that is able to capture individual eye movements and is linked to the tablet. All data are then pulled from SyncThink by Presagia Sports where it is integrated with the Pac-12’s injury registry platform (Pac-12 HAP) stored at Amazon Web Services (AWS, Virginia, USA). The data at Presagia are then further filtered to ensure that data from only student-athletes who consented to participate in the Pac-12 CAP are pushed to the Presagia Sports ‘research portal’. At the level of the research portal, the data are accessible by approved Pac-12 affiliated researchers as well as the PCCU investigators. The data are continuously audited by the PCCU project coordinator for completeness, data anomalies, missingness, and duplicate entries. This iterative process involves the project coordinator working with data coordinators to correct issues identified. The quality control processes for data presented here were completed in April 2020, at which time the data were uploaded into secure REDCap projects where they may be accessed by authorised Pac-12 researchers. The final data process involves QuesGen Systems (San Francisco, California) where data are sent from Presagia Sports to QuesGen where the broader NCAA-DoD CARE Consortium data reside. Figure 1 provides an overview of the data flow for the Pac-12 CAP from clinical collection to research data.
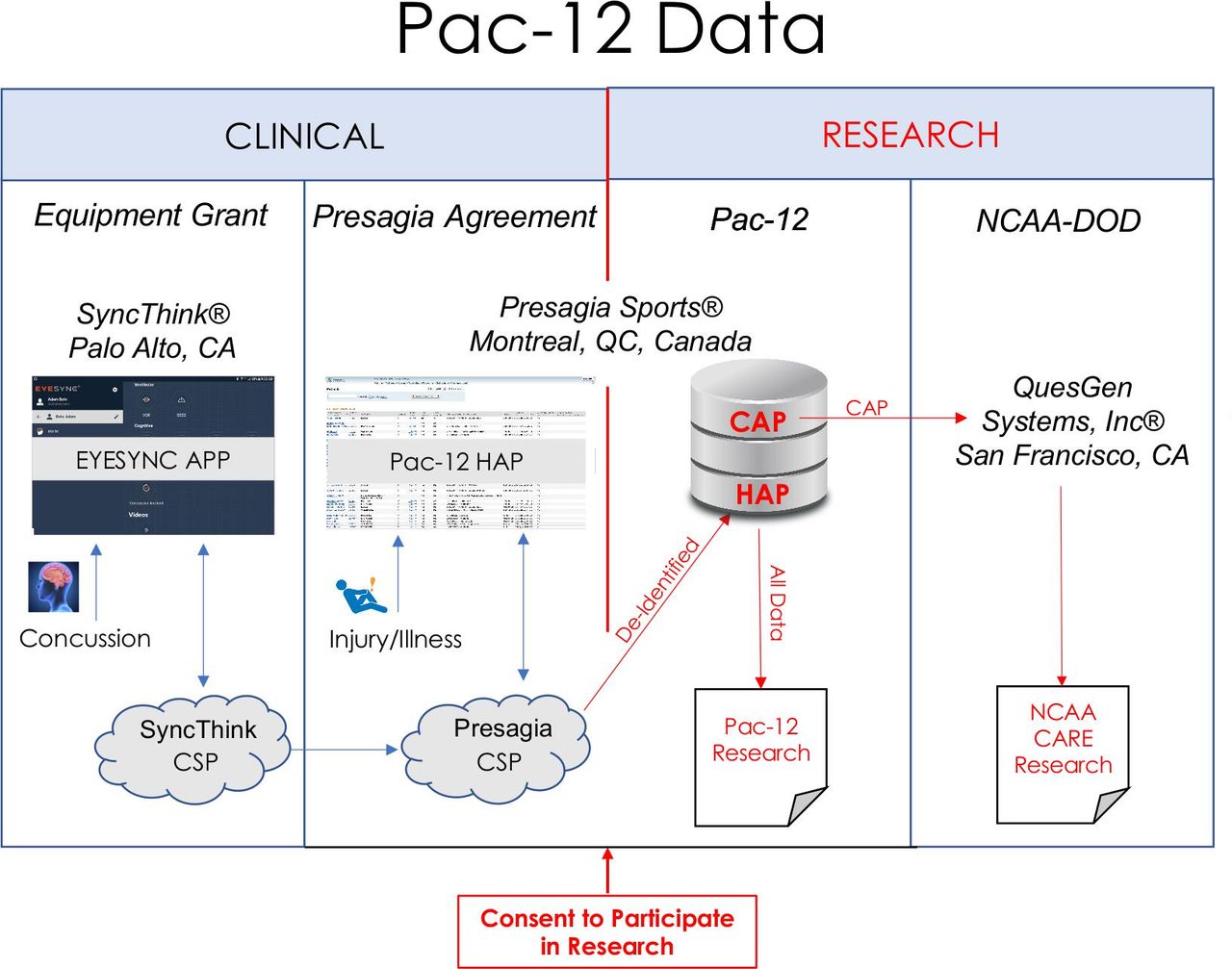
Clinical and research data flow for the Pac-12 CARE-Affiliated Program (CAP). DoD, Department of Defense; CSP, Cloud Service Provider (Computing); HAP, Health Analytics Program; NCAA, National Collegiate Athletic Association.
Data analysis
Preliminary data analysis began in March of 2020. Descriptive statistics were generated describing the sex, age, sport, injury circumstance and prior concussion status of participants that suffered a concussion during the 2018–2019 athletic year. This paper presents findings for four outcome variables from year 1: (1) SCAT5 symptom score, (2) SCAT5 symptom severity, (3) days to asymptomatic and (4) days to completing the RTP protocol. As there were multiple SCAT5 symptom evaluations per injury, for purposes of calculating symptom score, a particular symptom was counted for an athlete if he or she had endorsed it at any time during injury follow-up. The symptom score was the total number of symptoms that were endorsed at least once during the post-injury SCAT5 symptom evaluations. Symptom severity measures were taken from the initial post-injury SCAT5 symptom evaluation. Wilcoxon rank-sum tests were used to compare the symptom score and symptom severity between men and women. Cox proportional hazards models were used to compare both days to asymptomatic and days to completing the RTP protocol by sex, prior concussion history, symptom score >11 and symptom severity >27. These thresholds were the median symptom score and severity among concussed athletes during the initial post-concussion symptom evaluation. All statistical analyses and figures were done using R through RStudio V.1.1.447.16
Preliminary results
IRB processes, including participant recruitment and consent and baseline data collection began early 2018. A total of 2181 student-athletes consented to participate from the first four Pac-12 onboarded institutions during year 1 (1 July 2018–30 June 2019) of data collection: CU, OSU, UU and UW. In year two (1 July 2019–30 June 2020), ASU, USC, Stanford and UO, were onboarded while UA, Cal, UCLA and WSU are onboarding in year 3 (1 July 2020–30 June 2021). See table 1 for a depiction of the onboarding and data collection schedule.
As of April 2020, 2143 of the 2181 consented athletes had baseline assessment data available through the research portal. During year 1, the Pac-12 CAP captured data from 140 concussions sustained by 129 unique participants. Descriptive statistics on these concussions are presented in table 3. During year 1, among Pac-12 CAP participants, a greater percentage of concussions were sustained by men than women (55.7% vs 44.3%, respectively). The majority of concussions were sustained by individuals with no prior reported concussion history (62.9%). In addition, nearly half of the concussions (48.6%) occurred during practice which exceeded those that occurred during competition. Non-sport-related concussions were also common in this sample, with 27 concussions occurring outside of sport. The most common reason was an object hit to the head, followed by motor vehicle accidents, falls, bicycle or skateboard accidents, fights or assaults, and other collisions.
Descriptive information of year 1 Pac-12 CARE-Affiliated Program participants
Table 4 displays the number of concussions and injury burden (measured in days between injury and return to play) by sport. As expected, football accounted for the largest raw number of concussions (n=47) followed by women’s soccer (n=14). The cumulative incidence of concussion (number of cumulative incident concussion diagnoses divided by the total number of participants) was highest for women’s basketball (15.3%), women’s lacrosse (13.9%), men’s soccer (13.6%), women’s skiing (11.1%), women’s soccer (10.7%) and football (8.9%). The highest injury burden (days lost to sport) was football, with 360 days lost, followed by women’s soccer (208 days).
Cumulative incidence and injury burden of concussion by sport
The SCAT5 symptom score did not differ (p=0.69) between women (median=11.5; IQR: 7–17) and men (median=11; IQR: 8–17). Similarly, SCAT5 symptom severity at the initial post-injury symptom evaluation did not differ significantly (p=0.46) between women (median=29; IQR: 13–49) and men (median=25; IQR: 15–43). The most common symptom endorsements in both men and women were ‘headache’, ‘pressure in head’ and ‘don’t feel right’.
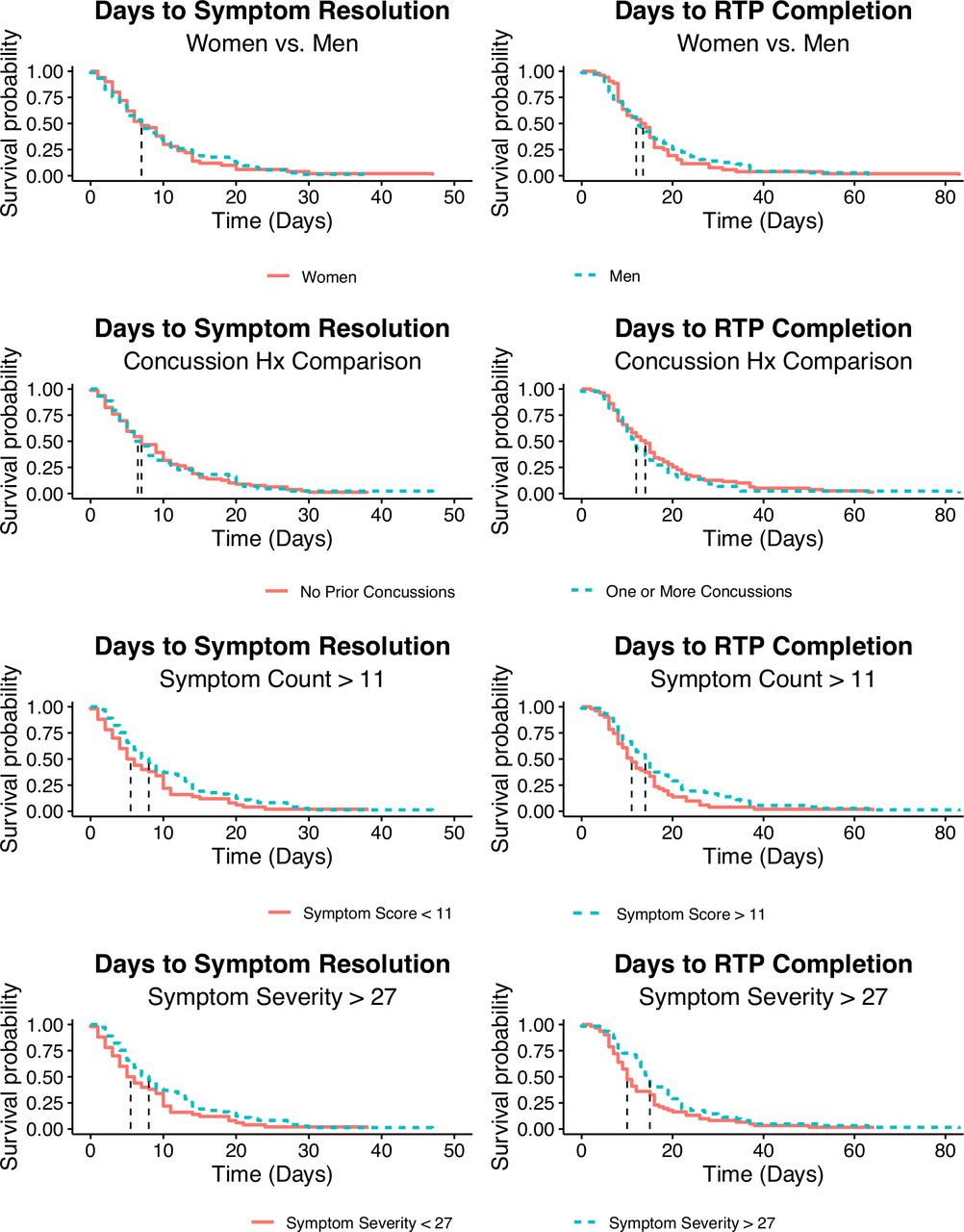
Survival curves (figure 2) were generated comparing both days to asymptomatic and days to completing the RTP protocol across sex, prior concussion history, initial SCAT5 symptom score and initial SCAT5 symptom severity. Among all concussions, the median number of days to asymptomatic and completing the RTP protocol were 7 and 12 days, respectively. Median SCAT5 symptom score and symptom severity at the initial evaluation were 11 and 27, respectively. Neither days to asymptomatic nor days to completing the RTP protocol differed between men and women or individuals with a concussion history and those without a concussion history. There were notable differences in days to asymptomatic and days to completing the RTP protocol among individuals above both the median initial symptom score of 11 and symptom severity score of 27. These individuals had longer recovery periods although the difference was not statistically significant.
{kind=link}
{kind=link}
Comparison of days to asymptomatic and days to completing the RTP protocol by sex, prior concussion history, initial SCAT5 symptom score and initial SCAT5 symptom severity. Hx, history; RTP, Return to Play, SCAT5, Sport Concussion Assessment Tool 5.
Discussion
The Pac-12 CAP has tracked 140 concussions from a sample of 2143 student-athletes across four Pac-12 institutions over the 2018–2019 initial period, documenting the specific circumstances of injury, follow-up clinical care assessments, and circumstances of the athlete’s return to full sport participation. The structure and findings of CAP can most appropriately be considered in the context of the design and results from two similar studies, the CARE Consortium4 from which CAP is derived and the Ivy League-Big Ten Epidemiology of Concussion Study (ILBT).17
The Pac-12 CAP recruits subjects from a multisite, collegiate population of student-athletes enrolled at universities in the Pac-12 Conference across multiple sports during the ‘baseline’ (offseason) time point. The Pac-12 CAP was largely modelled after the CARE consortium, with the noted exception that the CARE consortium does not have an athletic conference affiliation and also includes cadets enrolled through the US service academies. Of note, two Pac-12 institutions are original members of the CARE consortium (UCLA and UW). The ILBT recruits student-athletes from multiple Ivy League and Big Ten institutions with some institutional overlap between ILBT and CARE.
All three studies have ambitious targeted participation rates. Both CARE and the ILBT study estimated participation to be greater than 90%. Similarly, participation rates among the seven sports required for year 1 site enrolment in CAP were estimated to be greater than 90%. An emphasis was placed to have sports with high burden of concussion enrolled in year 1 of the study. Specifically, year 1 schools were encouraged to enrol men’s football, men’s and women’s soccer, men’s and women’s lacrosse and women’s volleyball. All three studies cover a breadth of collision, contact, and non-contact sports. Several sports, such as soccer, basketball and lacrosse, include both men’s and women’s varsity competition and are ideal for interesting gender comparisons.
The Pac-12 CAP clinical assessments and time points overlap entirely with the CARE study, though CARE collects more expansive assessments and measures in addition to more advanced research cores. The Pac-12 CAP shares several clinical outcomes with the ILBT study. Here, we focus on share of concussions attributable to each sport and circumstance, proportion of women versus men that sustain concussions, similarities in recovery time for women versus men, how initial symptomology is associated with recovery, and if history of concussion is associated with longer recovery periods.
In general, the results of the three studies are quite similar. We reported 140 concussions at four institutions during the first year of study (~35/site). CARE reported 1174 among 21 institutions during the first 2 years of study (~28/site/year), and the ILBT study reported 2241 among 15 institutions during the first 5 years of study (~30/site/year). The share of concussions sustained by female student-athletes (44.3%) was also slightly higher in our study than CARE (36.1%) and the ILBT study (39.6%).
Concussion burden by sport was also quite similar in the Pac-12 CAP and the ILBT study. In both initial studies, men’s football, men’s soccer and women’s soccer were among the sports with the greatest concussion counts. However, the ILBT also reported concussion among ice hockey and rugby participants, sports that were not represented during the first year of the Pac-12 CAP. Also, it should be noted that rates of concussion among sports in the Pac-12 CAP in this report are influenced by the emphasis placed on certain sports for year 1 enrolment. As such, the distribution of concussion among sports will likely change in subsequent years of study when full sport enrolment for all institutions is reached. Finally, in both studies concussion was common during both practice and competition. From 2016–2018, the ILBT reported an average of 112 concussions occurring during practice (58.9%) and 78 during competition (41.1%) among sports with exposure data. The Pac-12 CAP results for all sports were similar: 68 concussions during practice (60.7%) and 44 during competition (39.3%). It is likely, however, that this is attributed to the athletes spending more time in practice than competition as the rates of concussion per exposure were lower in practice than competition in the ILBT.17
We also noted 27 of the 140 concussions occurred outside of sport. Though this may seem like a high number relative to sport-related concussions, it has been shown previously that non-sport-related concussion in this age group is actually quite common.1 It is also important to note that non-sport-related concussion contributed significantly to the overall burden of concussion at the participant institutions. Both time to symptom resolution (median=10 days) and RTP (median=16 days) were greater than these metrics for the sport-related concussions.
Both the Pac-12 CAP and the ILBT study use the Sport Concussion Assessment Tool allowing for interesting comparisons. Both studies report ‘headache’, ‘pressure in head’ and ‘don’t feel right’ as the most common symptoms reported. Across all sports, we did not observe a difference in symptom endorsement between men and women. However, we did not have sufficient representation of all sports in which both men and women compete that have similar rules to perform a more meaningful comparison. The ILBT study was able to compare symptom reporting among women and men in basketball, soccer, rugby and water polo. The ILBT observed similar symptom reporting when comparing women’s and men’s basketball and rugby but reported greater symptom endorsement among men for both water polo and soccer. Similarly, men were more likely than women to report greater than the median of seven symptoms in these four sports. This analysis will be replicated by the Pac-12 CAP as the study reaches full enrolment and has more representation from sports with both women’s and men’s competition.
We reported a median time to symptom resolution and RTP of 7 and 12 days, respectively, among all concussions. For comparison, McCrea et al18 reported a median of 5.92 days (IQR=3.02–9.98 days) for symptom resolution and 12.23 days (IQR=8.04–18.92 days) for RTP among football players in the CARE study. Among football players in the CAP study, days to symptom resolution (median=6.5, IQR=4.0–11.0) and days to RTP (median=12.0, IQR=7.0–15.25) approximate these results.
To conclude, the Pac-12 CAP contributes a valuable ‘regional hub’ based on a unique conference model of the larger CARE consortium and aligns with the broader mission of conducting prospective longitudinal research and surveillance on sport-related concussion. While it shares many of the same features as the CARE consortium and ILBT study, the Pac-12 CAP is also well positioned to serve as a research and surveillance platform to integrate other physical and mental health domains related to concussion to further our understanding of the relationship of concussion on student-athlete health and well-being.
Data availability statement
Data are available upon reasonable request. Data security and dissemination are managed by the Presagia Sports Athlete Electronic Health Record software (Montreal, Quebec, Canada) and QuesGen Systems (San Francisco, California, USA).
Ethics statements
Ethics approval
All research was conducted with the appropriate institutional review board (IRB) approval (IRB Protocol 18-0068) across the participating Pac-12 institutions. Data security and dissemination are managed by the Presagia Sports Athlete Electronic Health Record software (Montreal, Quebec, Canada) and QuesGen Systems (San Francisco, California, USA).
References
Footnotes
Contributors ADB, MBM, NK, TDH: Directed the Pac-12 Concussion Coordinating Unit and lead the analysis and writing of the manuscript. DFA, KH, RR, DJP, JG, CG, SKP: Provided scientific overview, clinical expertise and manuscript review and edits.
Funding This project was supported, in part, with support from the Pac-12 Conference’s Student-Athlete Health and Well-Being Initiative and the Grand Alliance Concussion Assessment, Research and Education (CARE) Consortium, funded, in part by the National Collegiate Athletic Association (NCAA) and the Department of Defense (DOD). The US Army Medical Research Acquisition Activity, 820 Chandler Street, Fort Detrick, MD 21702-5014, is the awarding and administering acquisition office. This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs through the Psychological Health and Traumatic Brain Injury Program under Award NO W81XWH-14-2-0151. Opinions, interpretations, conclusions and recommendations are those of the author and are not necessarily endorsed by the Department of Defense (DHP funds). In addition, the content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the Pac-12 Conference, or its members, or the NCAA.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.