Article Text

Abstract
Objectives To determine and compare the health status of hip joints of individuals undertaking various lengths of long-distance running and of those who are not running.
Methods Fifty-two asymptomatic volunteers underwent bilateral hip 3.0 Tesla MRI: (1) 8 inactive non-runners; (2) 28 moderately active runners (average half a marathon (21 km)/week) and (3) 16 highly active runners (≥ marathon (42 km)/week). Two musculoskeletal radiologists reported the hip MRI findings using validated scoring systems. Study participants completed a Hip disability and Osteoarthritis Outcome Score (HOOS) questionnaire to indicate their perceived hip function.
Results The MRI findings show that there were no significant differences among inactive non-runners, moderately active runners and highly active runners in the amount of labral abnormalities (p=0.327), articular cartilage lesions (p=0.270), tendon abnormalities (p=0.141), ligament abnormalities (p=0.519). Bone marrow oedema was significantly more common in moderately active runners than in non-runners and highly active runners (p=0.025), while small subchondral cysts were more common in runners than in non-runners (p=0.017), but these were minor/of small size, asymptomatic and did not indicate specific exercise-related strain. Articular cartilage lesions and bone marrow oedema were not found in highly active runners. HOOS scores indicate no hip symptoms or functional problems among the three groups.
Conclusion The imaging findings were not significantly different among inactive non-runners, moderately active runners and highly active runners, in most hip structures, suggesting that long-distance running may not add further damage to the hip joints.
- hip
- MRI
- marathon
- running
- radiology
Data availability statement
Data are available upon reasonable request. Requests for access to data from the study should be addressed to the corresponding author at laura.horga.17@ucl.ac.uk. All proposals requesting data access will need to specify how it is planned to use the data, and all proposals will need approval of the study co-investigator team before data release.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings
The number of hip joint MRI abnormalities was not significantly different among inactive non-runners, moderately active runners and highly active runners in most structures, including the labrum, articular cartilage, ligaments, tendons. This is the first study on runners’ hips of this kind.
No chondral defects or bone marrow oedema were found in highly active runners.
Only minor non-specific bone marrow abnormalities were more common in runners than in non-runners.
How might it impact clinical practice in the future
The findings help correct popular misconceptions that long-distance running damages the hip joints, and therefore should be taken into account when making health recommendations.
The findings could help reassure individuals who are interested in getting into long-distance running that running is proven to be non-detrimental to hip joints.
Introduction
Running races longer than 21 km, including marathons (42 km) and ultramarathons (>42 km), have steadily grown in popularity over the last three decades.1 2 Both recreational and competitive running has been on the rise, with the average age of runners being over mid-30 years old and >40% women.3 Despite its multiple cardiorespiratory benefits, long-distance running has been reportedly linked with a concerning risk of lower extremity injuries, ranging from 19% to 80%.4 However, this wide range is controversial, considering that scientific evidence remains very limited.4
While the knee has received more research attention in the past, as a presumably common site of running-related injuries,4–12 very little is known about the health status of runners’ hips.7 Moreover, it is yet unclear what is the optimal dose of exercise and which running intensity is appropriate to the hip joints. Hip injury rate varies from 3% to 12%,4 13–15 due to differences in the definition of injury, type of study population, diagnosis tools.
Historically, specific diagnostic criteria and management tools with regards to hip injuries in athletes have been limited.16 17 Recent developments in MRI and hip arthroscopic surgery have resulted in increasing progress in the diagnosis and treatment of non-arthritic hips.16 In particular, the high resolution 3.0 Tesla (T) MRI technology offers clinical benefits in comparison to 1.5 T18 19 due to the high sensitivity and specificity in detecting early signs of pathologies.20–23
So far, only a few studies used MRI to document the prevalence of hip abnormalities in asymptomatic individuals24–28; only one study did MRI analysis of runners’ hips; however, this focused primarily on MRI changes after a marathon run, included small cohort (n=8), all professional and semi-professional long-distance runners, and used low-resolution unilateral MRI.7
The objective of this study was to assess and compare, for the first time, between the hip joint findings of inactive non-runners, moderately active runners and highly active runners on 3.0 T MRI scans. We believe that this assessment will provide a better understanding of whether undertaking various lengths of long-distance running is detrimental to the hips in comparison to inactive non-runners.
Methods
Study design and participants
This was a prospective cohort study of long-distance runners. The volunteers were recruited from the community of runners in the Greater London area. The study was a collaboration with the organisers of the Richmond Running Festival (Richmond Runfest), who advertised our study on their regular newsletters and included a contact email address for our study. Non-runners were recruited from University College London (UCL) by word of mouth and digital advertising channels. The study was advertised among UCL students and staff through regular newsletters and social media groups. All volunteers were screened with a questionnaire of our inclusion criteria: adults (aged ≥18 years old), with neither health nor hip problems and specifically absence of hip pain, hip injury, hip surgery or MRI contraindications. Exclusion criteria were: pregnancy or breast feeding, individuals aged <18 years, claustrophobia, history of anxiety, panic attacks or known hip problems. All volunteers provided written informed consent before participation.
Fifty-two volunteers met the inclusion criteria and were recruited to the study to undergo a hip MRI. The volunteers ranged from non-runners to ultra-distance runners. The volunteers were divided into three groups: (1) ‘inactive non-runners’: <1 hour physical activity, maximum 2 km walking/week; (2) ‘moderately active runners’: average running activity of half a marathon (21 km)/week; and (3) ‘highly active runners: running activity ≥a marathon (42 km)/week.
The final cohort included 8 inactive non-runners, 28 moderately active runners and 16 highly active runners. Moderately active runners reported a running activity of an average of 21 km/week (varying from 17 to 36 km/week), for a total of 3–4 hours of running/week, and never ran a marathon. Highly active runners reported a running activity ≥42 km/week (varying from 50 to 85 km/week), for a total amount of median 6 hours of running per week (range: 4–10 hours).
Volunteer characteristics were summarised in table 1.
Baseline characteristics of study participants
Participant self-assessment questionnaire
The Hip disability and Osteoarthritis Outcome Score (HOOS) questionnaire29 was completed by volunteers to self-assess their perceived hip joint condition and associated injuries that can result in osteoarthritis at study recruitment. The questionnaire is divided into five sets of questions based on key hip outcomes: pain, other symptoms, function in daily living, hip-related quality of life and function in sport and recreation.
MRI protocol
All volunteers underwent hip 3.0 T non-contrast MRI scans of both hips (Siemens Magnetom Vida Healthineers, Erlangen, Germany) with a dedicated 18 channel ultraflex coil. The imaging protocol was the following: proton density-weighted fat-suppressed (FS) sequences in coronal (repetition time (TR): 4190 ms/echo time (TE): 44 ms; image size/acquisition matrix: 512×512 pixels) and sagittal bilateral planes proton density (FS turbo spin-echo (TSE) TR: 4420/TE: 35 (320×320 pixels)); axial (T1 TSE TR: 27/TE: 10); coronal proton density TSE (TR: 3290/TE: 39); axial proton density (FS TSE TR: 4400/TE: 36 (384×384 pixels)) and Dixon axial four phases TR: 4220/TE: 45; T1 VIBE 3D coronal: TR: 0.1/TE: 4.92. The optimised protocol included Dixon sequences in four phases: in-phase, out-of-phase, water phase and fat phase. The thickness of all slices was 3 mm, and the total acquisition time per scan was 30 min (for both hips).
Imaging analysis
The bilateral MRI scans were evaluated and reported by a senior musculoskeletal radiologist using a picture archiving and communications system workstation. The MR images of a subset of volunteers, that is, 20% of the cohort, were randomly selected for an additional independent evaluation by a second senior musculoskeletal radiologist to assess the reproducibility of the readings. Previous imaging studies included a 10% subset of the total number of participants in double-reporting30; we doubled this to a 20% subset to increase reliability.
In cases of disagreement between the radiologists’ reports, the final score (agreement score) was achieved with consensus reading in a second MRI reporting session.
Validated scoring systems were used for MRI reporting, indicating the presence of lesions of different grades/sizes for a number of hip joint structures: labrum, articular cartilage, bone marrow, tendons, ligaments (table 2).31 32 Any other findings, such as trochanteric bursitis or effusion, were specified.
Grading systems
Statistical analysis
Comparisons between the groups of volunteers were made using the unpaired t-test or Mann-Whitney U test (when two groups were compared) and analysis of variance test or Kruskal-Wallis (when more than two subgroups were compared). A χ2 test was used for gender comparisons between groups. Correlations between baseline demographics (age, gender or body mass index (BMI)) and each type of MRI abnormality were assessed using a χ2 test, respectively. Possible associations were checked by making calculations of ORs with 95% CIs. Inter-reader agreement was calculated based on kappa statistics: kappa values between 0.610 and 0.800 indicate substantial agreement, while values between 0.810 and 1 indicate almost perfect agreement.33 Statistical significance was considered for p values <0.05 (GraphPad Prism, V.6.0c).
Patient and public involvement
This research would not have been possible without the contribution of our study participants, including runners and non-runners who agreed to volunteer as subjects in our study. The participants were not involved in the design or conduct of the study, but they were involved in the dissemination of our study findings across social media and conference presentations. They were informed about the use of their data through consent sheets. Also, a summary report was given to the participants informing them about their results and any health implications.
Results
Participant characteristics
There were no significant differences among inactive non-runners, moderately active runners and highly active runners in terms of baseline demographics: age (p=0.069), gender (p=0.269), BMI (p=0.409).
Mean HOOS scores were ≥90/100 in inactive non-runners (98.8±2), moderately active runners (96.2±5.7) and highly active runners (97.9±3.2).
Also, mean HOOS scores for each individual item were ≥90/100 in inactive non-runners: symptoms (95.6±6.8); pain (100); function in daily living (100); function in sport and recreation (98.4±2.9) and knee-related quality of life (97.7±3.2); in moderately active runners: symptoms (92.6±9.9); pain (97.5±4.5); function in daily living (98.7±2.7); function in sport and recreation (96.1±7.3) and knee-related quality of life (94.3±11.5); in highly active runners: symptoms (92.5±11.2); pain (97.3±4.8); function in daily living (99.3±2.3); function in sport and recreation (98.8±2.6) and knee-related quality of life (96.9±7.6).
MRI findings
Our analysis of MRI findings was done per all hips of study participants. The agreement between the scores assigned by the two radiologists for the double-reported scans was very good (kappa 0.850).
Labrum
Labrum abnormalities were found in one (6%) hip of a non-runner, 12 (21%) hips of moderately active runners, 5 (16%) hips of highly active runners (table 3; figure 1). There were no significant differences among groups (p=0.327).
Prevalence of MRI findings in the hips of inactive non-runners, moderately active runners and highly active runners
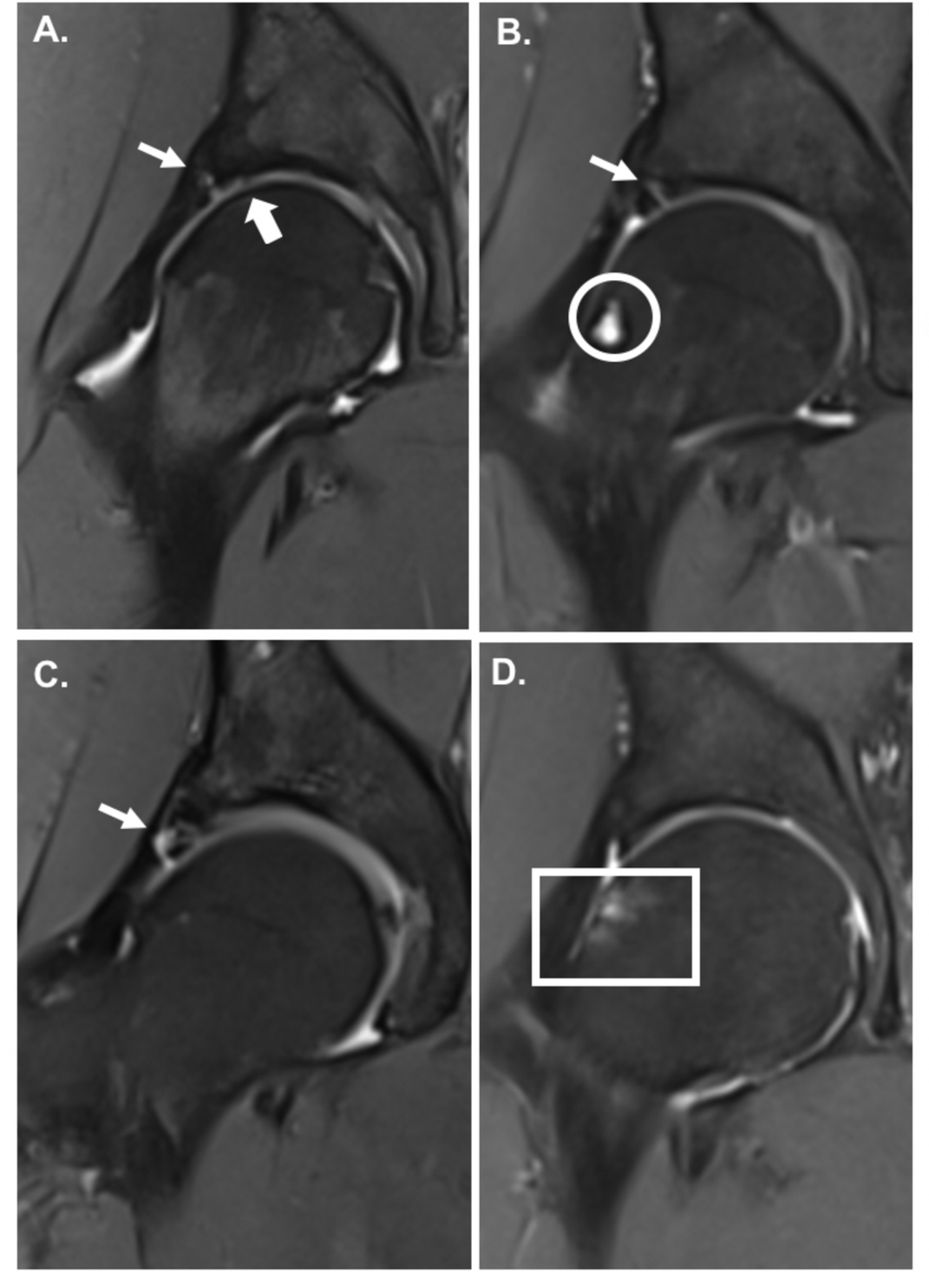
Coronal Dixon MR images showing intra-articular abnormalities in four volunteers, in ‘in-phase’ MRI sequences: (A) Moderately active runner 1 with labrocartilage separation (small arrow) and full thickness cartilage defect (big arrow); (B) moderately active runner 2 with simple labral tear (small arrow) and subcortical cyst (circle); (C) highly active runner 1 with complex labral tear (small arrow); (D) moderately active runner 3 with subchondral bone marrow oedema (square); SHOMRI grading system was used in the assessment of labrum, cartilage and bone marrow (see table 2); SHOMRI, scoring hip osteoarthritis with MRI.
The non-runner’s labrum signal was found in the anterior side. In the moderately active runners’ group, abnormalities of the labrum were found most frequently in the anterosuperior location, followed by superior, anterior and superior locations. In the highly active runners’ group, the majority of labral findings were also detected in the anterosuperior and superior subregions, but no MRI signal was detected in other locations.
Articular cartilage
Abnormalities of the acetabular cartilage were identified in three (5%) hips of moderately active runners, while in highly active runners and inactive non-runners no lesions were detected (p=0.270).
All were found in the acetabular region; none was detected in the femoral region (see table 3; figure 1).
Bone marrow
Bone marrow oedema was detected in seven (13%) hips of moderately active runners only (see table 3; figure 1). No lesions were detected in highly active runners nor inactive non-runners, and significant differences among the three groups were identified (p=0.025)
Structurally, four were found in the femoral region and three in the acetabular region.
Additionally, both hips of one moderately active runner (4% hips) and six (19%) hips of highly active runners had subchondral cysts, while inactive non-runners had no cysts. Non-runners had a significantly lower prevalence than the other groups (p=0.017).
They were all minor MRI abnormalities.
Tendons
Moderately active runners presented with small MRI signal in tendons (tendinosis) in nine (16%) hips (table 3). Highly active runners had tendinosis in nine (28%) hips. No signal was detected in inactive non-runners; however, differences between groups were not significant (p=0.141).
Tendinosis was characteristic to the following tendons: gluteus medius, minimus; tensor fascia latae, psoas and hamstring (figure 2).
{kind=link}
{kind=link}
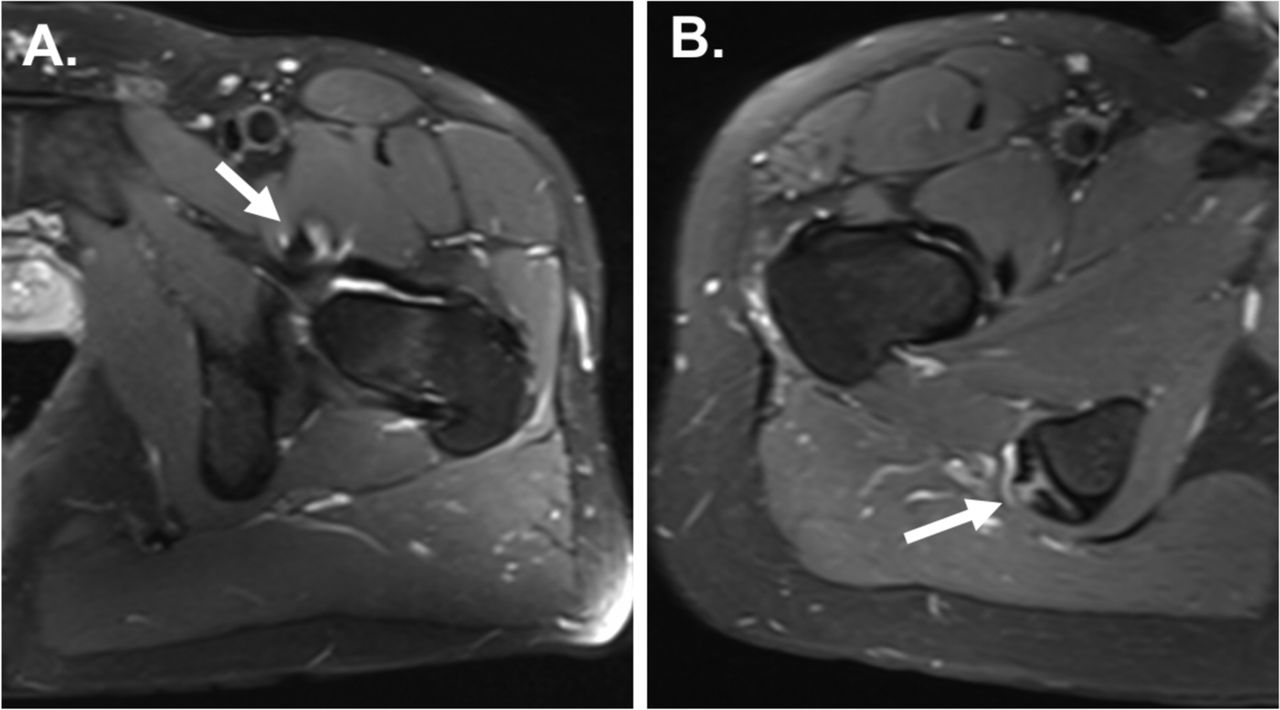
Axial Dixon MR images showing tendinosis, in ‘water phase’ sequences in two volunteers, respectively; (A) moderately active runner 1 with psoas tendinosis (arrow); (B) highly active runner with hamstring tendinosis (arrow). Arrows indicated the specific MRI findings. Grading systems developed by Chi et al were used in the assessment of tendons. Tendinosis is low-grade abnormality (see table 2).
Ligaments
Abnormal ligament signal on MRI was found in six (11%) hips of moderately active runners and in two (6%) hips of highly active runners (table 3). There was no MRI signal in inactive non-runners’ hips, and differences between groups were not statistically significant (p=0.519).
Other findings
Small joint effusion was present in three (9%) hips of highly active runners. Trochanteric bursitis was found in seven (13%) hips of moderately active runners, five (16%) hips of highly active runners and one (6%) hip of an inactive non-runner.
Associations between MRI findings and demographics
There were no statistically significant differences between men and women for any type of lesion.
The BMI of volunteers presenting with MRI abnormalities was not significantly different from those without abnormalities, except for tendinosis (p=0.053) in moderately active runners; this was not the case in highly active runners or inactive non-runners. A moderately active runner with BMI ≥25 kg/m2 (overweight) was 5.7 more likely to present with tendinosis (95% CI, 0.9 to 36.1).
The prevalence of lesions was generally not associated with age. Only in moderately active runners, the mean age for those with tendinosis was slightly higher than those without it (37.7±12.1 years (n=7) vs 30.6±6.5 (n=21)). Moderate dose runners aged ≥40 years old were 7.1 times more likely to have tendinosis (95% CI, 0.9 to 57.6; p=0.046).
There were no statistically significant associations between the presence of labral tears and other findings or other associations between the presence of different types of MRI abnormalities.
Discussion
Summary of findings
Generally, significant differences were not found among inactive non-runners, moderately active runners and highly active runners for most hip structures. Only bone marrow oedema was significantly more common in moderately active runners than in inactive non-runners and highly active runners (p=0.025), while subchondral cysts were significantly more common in runners than non-runners (p=0.017)—however, these were minor/small in size and all asymptomatic, non-specific, thus not indicating specific exercise-related strain. No clinical correlations could be made with HOOS self-reported questionnaire scores, which suggested no hip symptoms or functional limitations. No cartilage defects or bone marrow oedema were detected in highly active runners.
Comparison with previous studies
Other studies have already analysed asymptomatic hips of adults to look at incidental findings/potential clinically (in)significant ones at their early stages, using high-resolution MRI equipment, which is highly sensitive in detecting subtle early signs of lesions.24–28 However, this has not been done in asymptomatic runners, and it is yet not fully understood whether running is good or bad for the hips.
Literature on MRI-based running research on hip joints is extremely limited. No direct comparisons with other previous studies can be made. So far, only one study assessed the hip joints of runners on MRI7; however, it was focused on monitoring the impact of a single marathon run on their hips and knees instead of a comprehensive analysis of the general prevalence of asymptomatic hip MRI findings. Contrary to our findings, no abnormalities were found before or after the marathon; however, limitations of the study include a small sample size (n=8), the inclusion of professional and semi-professional runners only (achieving 60–150 km/week) unilateral scans, low-resolution MRI.
Also, there is no clear evidence to suggest that BMI is a key factor associated with running-related injuries. In our study, we found that participants with BMI ≥25 kg/m2 (overweight) were more likely to have tendinosis on MRI, although they were asymptomatic. Long-term monitoring is required to assess the clinical significance of these findings.
Previous studies have not monitored the asymptomatic hips of participants over a long period of time. Existing long-term studies only assessed recovery levels or long-term consequences of patients with hip pathologies or hip surgeries, respectively.34–36
Clinical significance and future research
First, our study provides a better understanding of the potential impact of varying levels of exercise beyond small amounts on hip joint health. Second, the findings may help in improving management and physicians’ decision-making in patients with symptomatic hips, given the asymptomatic nature of intra-articular pathologies.24 37 Currently, indications for hip arthroscopy include labral tears, articular cartilage and bone marrow lesions, ligamentum teres disorders.38–41 However, symptoms of hip pain in an individual cannot immediately be associated with a labral tear or other related findings on MRI. The decision to conduct hip arthroscopy should not be based solely on the presence of a labral pathology on MRI but also on symptoms and further investigations.27
Future studies are needed to clarify how much exercise is optimal in the long-term, whether symptoms develop over time or whether MRI findings progress further in inactive non-runners, moderately active runners and highly active runners.
Strengths and weaknesses
The main study strengths are the large sample size, the use of high-resolution MRI technology (3.0 T MRI and multichannel coil) and optimised MRI protocol (including Dixon sequences42) for good visualisation and comprehensive analysis of all hip joint structures. This is the first study assessing specifically the prevalence of baseline findings in the hip joints of runners using 3.0 T MRI and the first one to compare between the outcomes of inactive non-runners, moderately active runners and highly active runners.
We acknowledge a number of limitations: (1) Radiological assessment may involve a certain degree of bias; however, to reduce this, two senior musculoskeletal radiologists were involved in reporting the scans: one radiologist reported all images, then a subset of images was co-reported by a second radiologist; (2) The male to female ratio between groups is different (including lower number of female participants than male participants in the highly active runners than in non-runners). Moreover, women are known to be more prone to degenerative joint disease. Therefore having equal gender distribution would have improved the analysis; (3) The BMI and age ranges are wide, and the distribution of ages included in a small number of subjects varies between groups. Also, the majority of participants were young, aged <40 years old and only a few older individuals were included in the study. Inactive non-runners were younger than runners; therefore, despite non-runners’ low physical activity levels, their young age might have played in their favour when it comes to their hip joint MRI outcomes. Therefore this needs to be considered when interpreting their MRI findings in comparison to slightly older cohorts of runners; (4) The study population is quite heterogeneous for a study with a relatively small number of subjects; (5) The sample size is relatively small (and not equal between groups), and further studies are required to confirm the findings; (6) Other confounding factors may need to be considered, that is, running surface, biomechanics, leg alignment; (7) Follow-up studies are required to assess the clinical relevance of the results over time, including potential progression/regression of current findings along with monitoring changes in symptoms over time.
Data availability statement
Data are available upon reasonable request. Requests for access to data from the study should be addressed to the corresponding author at laura.horga.17@ucl.ac.uk. All proposals requesting data access will need to specify how it is planned to use the data, and all proposals will need approval of the study co-investigator team before data release.
Ethics statements
Ethics approval
The study was approved by University College London Research Ethics Committee (UCL REC Reference Number 13823/001). All participants gave informed consent before taking part.
Acknowledgments
We thank all study participants who allowed their clinical details to be used for research and educational purposes.
References
Footnotes
Contributors LMH, JH, AF, ADL, AHir and AHar developed the study concept and design. LMH, JH, AF, ADL and AHar contributed to the acquisition of data. LMH, JH, AF, ADL, AHir and AHar contributed to the analysis of data. LMH, JH, AF, AHir and AHar contributed to the interpretation of data. LMH conducted the statistical analysis. All authors were involved in writing the manuscript. AHar obtained the funding for the study data and analysis. LMH, JH and ADL provided administrative, technical and material support for the study analysis. AHar is the study supervisor. All authors had full access to the data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. All scans were conducted at The London Clinic. AHar is the guarantor. The corresponding author LMH attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This research study was funded by patient donations, Trustees of The London Clinic Charity, the Maurice Hatter Foundation, the Rosetrees & Stoneygate Trusts, the RNOH Charity and supported by researchers at the National Institute for Health Research University College London Hospitals Biomedical Research Centre.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.