Article Text

Abstract
Introduction Shoulder instability injuries are common in sports involving collisions and overhead movements. Arthroscopic Bankart repair and the open Latarjet are two commonly used surgical stabilisation procedures. There is a lack of knowledge surrounding movement strategies, joint loading and muscle strength after each of these procedures. This study will compare: (1) shoulder joint neuromechanics during activities of daily living and an overhead sporting task; (2) shoulder range of motion; (3) shoulder strength; and (4) self-reported shoulder function and health status, between individuals who have undergone an arthroscopic Bankart repair versus open Latarjet.
Methods and analysis This is a prospective cohort, single-centre, non-randomised parallel arm study of surgical interventions for athletic shoulder instability injuries. Thirty participants will be recruited. Of these, 20 will have experienced one or more traumatic shoulder instability injuries requiring surgical stabilisation—and will undergo an arthroscopic Bankart repair or open Latarjet procedure. The remaining 10 participants will have no history of shoulder instability injury and act as controls. Participants will undergo baseline testing and be followed up at 3, 6 and 12 months. A two-way (group×time) analysis of variance with repeated measures on one factor (ie, time) will compare each outcome measure between groups across time points.
Ethics and dissemination This study was approved by the Barwon Health and Deakin University Human Research Ethics Committees. Outcomes will be disseminated through publications in peer-reviewed journals and presentations at relevant scientific conferences.
Trial registration number Australian and New Zealand Clinical Trials Registry (ACTRN12620000016932).
- shoulder
- surgery
- orthopaedics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Traumatic anterior shoulder instability is common in sports involving collisions and overhead movements, such as Australian rules football, American football and rugby union.1–3 These injuries occur when the humeral head is forced out of the shoulder joint socket (ie, subluxation or dislocation).4 Avulsion of the labral attachment of the antero-inferior glenohumeral ligament between the 3 and 5 o’clock positions (ie, Bankart lesion) is the most commonly observed pathology in traumatic anterior shoulder instability.5 Glenoid bone loss or defects, along with humeral bone defects (ie, Hill-Sachs lesions) can also occur.6–8 The incidence of shoulder instability is increasing,9 recurrent injuries are common,10 and patients can experience arm pain and weakness with a shoulder that easily dislocates with minimal movement or force.4 These symptoms can lead to repeated hospital admissions, decreased ability to participate in activity or sport, fewer employment opportunities and a reduction in overall health.11
Effective clinical care and rehabilitation is vital to avoid recurrent injuries, reduced shoulder function and joint degradation later in life.4 Surgery is commonly used to address intra-articular pathology, restore shoulder function and correct stability following shoulder instability injuries. Arthroscopic procedures are typically preferred due to their minimally invasive and conservative nature.12 Arthroscopic Bankart repair (ie, anatomic repair of Bankart lesion) is commonly used13 and aims to restore the labrum and re-establish appropriate tension in the joint capsule and ligaments.14 In certain cases, open (ie, surgery via a large incision) procedures are preferred.14 The Latarjet procedure is a non-anatomical, open shoulder reconstruction surgery involving a bone block via transfer of the inferior surface of the coracoid process to the anterior glenoid with the attached conjoint tendon.15 The Latarjet procedure is more commonly used in cases with significant glenoid bone loss, large Hill-Sachs lesions, or combined glenoid and humeral bone defects14 —but is emerging as a preferred option for operative shoulder stabilisation in contact sport settings.16
A proposed benefit of the Latarjet procedure is the reduced risk of recurrent instability, with studies reporting a reduced number or rate of recurrent subluxations and dislocations in comparison with other (eg, arthroscopic Bankart repair, up to 10% at up to 8 years17) reconstruction procedures.18 19 Neyton et al20 found no recurrent subluxations or dislocations over a mean follow-up time of 12 years in a group of rugby union players who underwent the Latarjet procedure. In addition, while arthroscopic repair can restore shoulder stability and function, not all athletes who undergo this procedure return to the same level of sport.21 While the Latarjet procedure may reduce the risk of recurrent instability and promote return to sport, bone block procedures incur higher complication rates (ie, 7.2%–13.6% vs 0.5%–6.2% for non-bone block procedures)22 and may also contribute to postoperative osteoarthritis due to impingement on articular cartilage.23 The Latarjet procedure requires high precision and subtle variations in surgical technique (eg, coracoid bone graft placement and orientation, graft fixation, subscapularis reattachment location) may impact graft strength, the loads experienced at the shoulder and the likelihood of degenerative changes arising.24–26 These surgical choices can impact on the structure and function of the shoulder joint following reconstruction, and subsequently affect glenohumeral joint loads during movement. There is, however, an absence of studies investigating the joint loads experienced during movement following shoulder stabilisation procedures. Knowledge of how shoulder stabilisation procedures impact joint loading during movement can aid in understanding the risk and for joint instability and degenerative changes following procedures, and provide an adequate target for rehabilitation efforts. Three-dimensional analyses, combined with musculoskeletal modelling and simulation, afford the opportunity to examine muscle function, and joint loading and stability during movement.
Various differences in self-reported (ie, Rowe scores) and objective measures (ie, range of motion) of shoulder function have been reported between arthroscopic and Latarjet procedures. A systematic review and meta-analysis by An et al27 found a weighted mean difference of 3.29 (95% CI 2.37 to 4.20) in favour of the Latarjet procedure over Bankart repairs in self-reported Rowe scores (ie, a scoring system assessing shoulder stability, motion and function). This value does, however, fall below the recommended minimal clinically important difference (ie, 9.7) for the Rowe score.28 The review also found external rotation range of motion loss was less in Latarjet procedures compared with Bankart repairs (11.9° vs 20.9°; weighted mean difference=5.75, 95% CI 4.73 to 6.77).27 However, these data encompassed studies that examined both arthroscopic and open Bankart repairs, as well as studies that examined traditional and variants (ie, Bristow-Latarjet, open Bristow) of the Latarjet procedure. To our knowledge, only one study19 has compared outcomes between arthroscopic Bankart repair and the traditional open Latarjet procedure. In this retrospective study, the recurrent instability rate was lower and Rowe scores were higher in the open Latarjet group, with no data on range of motion reported.19 There appears to be a lack of prospective evaluation comparing relevant measures of shoulder function between arthroscopic Bankart repairs and traditional open Latarjet procedures. Further, none of the aforementioned studies have examined shoulder strength—an important aspect of shoulder function and stability, which has implications for rehabilitation for glenohumeral instability.29 There is also no indication across this literature regarding how variations in measures of shoulder joint function (self-reported or objective) impact on shoulder joint neuromechanics (ie, kinematics and kinetics, joint loading, muscle activation and forces) during movement tasks.
The aim of this study is to compare outcomes between individuals who have undergone an arthroscopic Bankart repair versus a traditional open Latarjet procedure (herein referred to simply as a Latarjet procedure), while also referencing these outcomes to healthy uninjured controls. The outcomes that will be examined in this study are: (1) shoulder joint neuromechanics (ie, shoulder joint loads, kinematics, kinetics, and muscle activation and forces) during activities of daily living and an overhead sporting task; (2) shoulder range of motion; (3) shoulder strength; and (4) self-reported shoulder function and health status. A metric of glenohumeral joint stability will be derived from calculated shoulder joint loads during movement tasks and used as the primary neuromechanical outcome measure between the two procedures. Knowledge of how the two procedures impact shoulder joint neuromechanics and glenohumeral stability during relevant movement tasks involving the shoulder may provide evidence for the use of a surgical procedure in restoring movement capacity, reducing the potential for future instability and minimising joint degradation over time. Further, understanding how shoulder joint function and the relationship of these to joint loading and stability during movement varies between procedures can assist in designing more targeted and specific rehabilitation strategies following shoulder stabilisation.
Methods and analysis
Study design
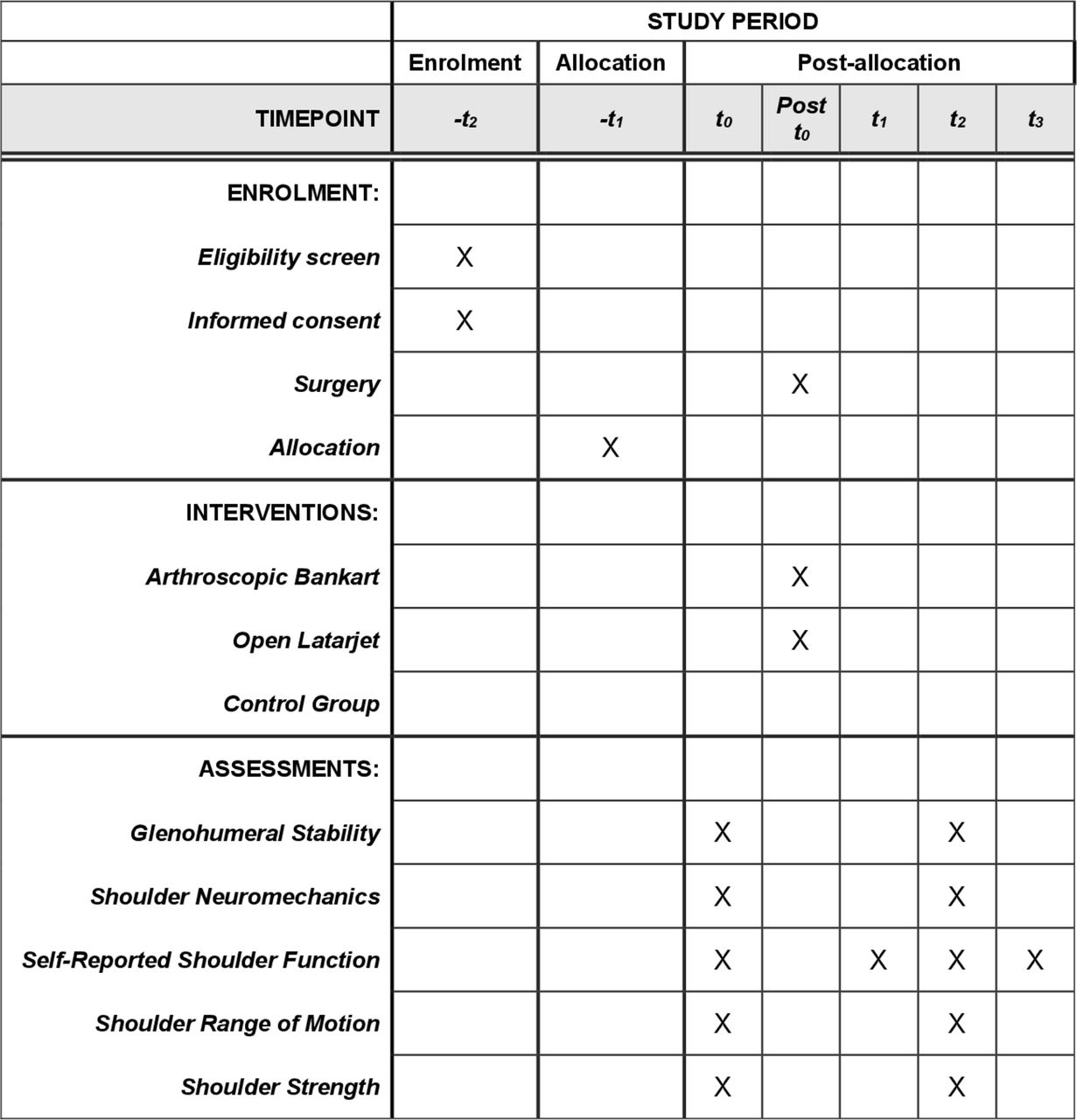
This study is a prospective, single-centre, non-randomised parallel-arm trial. The study will be conducted at a large regional health service in Victoria, Australia. The study will include baseline testing, and follow-up testing at 3, 6 and 12 months (see study design in figure 1). Over the 12-month study period, two or four measurement points are included across the various outcomes (see figures 1 and 2). At baseline (ie, t0), participants will attend a testing session where all outcome measures will be assessed. At 3 months (ie, t1), participants will be invited to complete the questionnaires pertaining to self-reported shoulder function and health status. At 6 months (ie, t2), participants will be invited to attend the follow-up testing session where all outcome measures will be measured. At 12 months (ie, t3), participants will again be invited to complete the questionnaires pertaining to self-reported shoulder function and health status. The study conforms to the Standard Protocol Items: Recommendations for Intervention Trials.

Schematic of participant flow through study protocol. MISS, Melbourne Instability Shoulder Scale; OIS, Oxford Instability Score.

Time points of procedures and data collection during study period.
Study population
Participants in this study will be men and women, between the ages of 18 and 40 years, currently or recently (ie, within the past 12 months) engaged in an overhead contact sport. Overhead contact sports included, but not limited to, in this study will be Australian rules football, rugby league or union, and lacrosse. Those referred to the Geelong Orthopaedic Group or Barwon Health Outpatient clinics who are designated to undergo shoulder stabilisation surgery will be invited to participate and act as the experimental groups. All patients attending the study site for preoperative assessment of shoulder stabilisation surgery will be assessed for eligibility by the surgeon, orthopaedic registrar or research coordinator (see table 1). Athletes with no history of shoulder instability or upper limb surgery will also be recruited through local sporting leagues and act as the control group, and be assessed against the same eligibility criteria. Eligible participants will be invited to participate in the study and informed written consent will be obtained. Participation in the study is voluntary. Recruitment is expected to occur over an 18-month period.
Inclusion and exclusion criteria
Intervention
Three surgeons perform surgical shoulder stabilisation procedures at the centre, all of whom will be involved in the study. All surgeons involved in this study are fellowship trained (Royal Australasian College of Surgeons), have greater than 10 years of experience performing upper limb surgical reconstructions, and are currently active members of the Shoulder and Elbow Society of Australia.
Participants in the experimental groups will undergo shoulder stabilisation either via an arthroscopic Bankart repair or an open Latarjet procedure. For the arthroscopic Bankart procedure, individuals will be evaluated under anaesthetic (both a peripheral block and general anaesthesia) to determine the stability pattern of the glenohumeral joint, with clinical findings considered alongside preoperative medical images.30 The joint space will be accessed with arthroscopic portals.30 The glenohumeral labral tear will be prepared with liberator probes and shaver, and capsulolabral reduction and fixation anteriorly and/or posteriorly will occur with anchors according to the injury pattern.30
For the open Latarjet procedure, an oblique 3–5 cm incision will be made under anaesthesia below the tip of the coracoid process and extending inferiorly down the deltopectoral groove to the superior portion of the axillary fold.24 A 22–27 mm bone graft will be harvested from the tip of the coracoid process, with harvesting and preparation of the graft performed according to standardised procedures and ensuring that the graft is shaped to be flush with the prepared anterior face of the glenoid.24 The anterior portion of the shoulder will be exposed by dividing the subscapularis in line with the muscle fibres,24 maintaining a 50–50 split of the upper and lower portions of the muscle. A T-shaped incision will be made in the labrum at the apex of the bony deformity in preparation to set the coracoid bone graft in place. The coracoid bone graft will be positioned so that it serves as an extension of the inherent articular arc of the glenoid.24 Once the desired graft position is identified, fixation of the bone graft to the anterior glenoid will be achieved via two surgical screws under compression.24 Anchors will be placed in the native glenoid and the joint capsule repaired.24 The subscapularis will be repaired over the coracoid bone graft, with the conjoint tendon exiting anteriorly through the previously split segments of the subscapularis muscle.24
Postoperative care of both experimental groups (ie, arthroscopic Bankart and open Latarjet) will follow the clinic’s standardised protocols and care pathways.30 Participants will use an immobiliser sling for at least 4 weeks post-surgery and then commence a rehabilitation programme to improve active shoulder stability.30 Progressive increases to range of movement exercises, strengthening and functional restoration will be incorporated into each participant’s individualised programme.30 Rehabilitation will be monitored by the clinic for at least 3 months postoperatively. Participants will undergo standard clinical practices for follow-up medical imaging. Participants receiving the open Latarjet treatment will undergo a CT scan at 4 months post-procedure; while participants in both experimental groups will undergo an X-ray 12 months post-procedure. In addition to standard clinical practices, the number of training sessions (both with clinic staff and home-based sessions) the individual completes during the 6-month period following surgery will be monitored via an online survey. Specifically, participants will be prompted to complete an online survey detailing the number and type (ie, range of motion, strength or functional movement) of training sessions they have completed over the past 2 weeks. Return to sport will be assessed after 6 months by the operating surgeon, pending the participant’s recovery.30 Participants in the control group will be instructed to continue their regular training over the study period.
Assignment of interventions
The decision as to what stabilisation procedure participants in the experimental group undergoes will be determined by consultation between the individual and the acting surgeon. The primary factor guiding the choice of reconstruction procedure will be the extent of glenoid bone loss and the presence of humeral bone defects, whereby the Latarjet procedure will be more likely in the presence of greater bone loss and/or defects (ie, >20% anterior glenoid bone loss).31 All participants in the experimental groups will undergo MRI, and where a bone defect is identified be referred for a CT scan. A sagittal view of the glenoid face will be used to fit a circle to the 3–9 o’clock inferior contour of the glenoid. The missing area of this circle (ie, defect) will be determined and presented as a proportion of the total circle area as a means to quantify the bone defect. A secondary factor used in guiding the choice of reconstruction procedure will be the patient’s history of shoulder instability, whereby the Latarjet procedure may be more likely in patients with repeat traumatic joint instability. Due to these factors, randomisation of participants as part of this study is not appropriate. Eligible participants will be invited to participate in the study and allocated to the appropriate experimental group based on the procedure they will undergo. Given the different factors driving surgery choice (eg, presence of glenoid or humeral bone loss/defects, prior history of shoulder instability), it is likely that aspects of shoulder pathology and injury history will differ across the experimental groups at baseline in this study. Glenoid bone loss, glenoid and humeral bone defects, injury history and previous surgeries will be recorded from participants and any differences in these across groups will be considered in interpreting the final results.
Blinding
Given the nature of the surgical interventions, the study will be unable to blind participants to the specific stabilisation procedure they receive. Further, the nature of the experimental procedures also means that blinding of assessors will be impossible. During the laboratory-based testing sessions, participants will be required to have markers placed on the skin around the shoulder, leaving this area exposed to the assessor. The presence of surgical scars will reveal whether the participant received the arthroscopic or open procedure. Further, data analysis will involve examining medical imaging data from participants. The analyst will therefore be able to identify the stabilisation procedure performed. Given these factors, no blinding of participants or assessors/analysts will occur.
Data collection and analysis
Data collection will be performed at four time points (t0, t1, t2 and t3). Two of these testing sessions (ie, t0 and t2) will include all measures, while t1 and t3 will only include self-reported shoulder function and health status measures.
Glenohumeral stability and shoulder neuromechanics
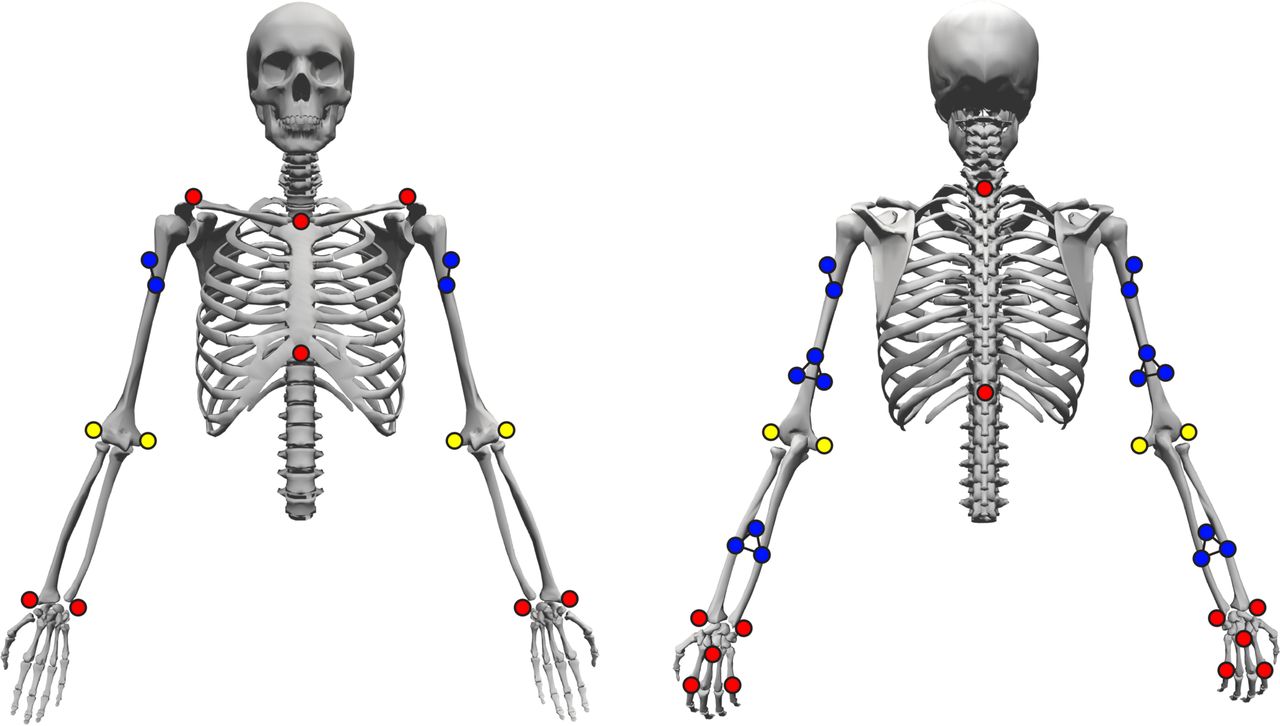
Participants will undergo a laboratory-based biomechanical assessment at t0 and t2, where they will be evaluated while performing a series of movement tasks. Prior to undertaking the movement tasks, 38 14 mm retro-reflective markers will be affixed to participant’s upper limbs and torso (see figure 3). A static calibration trial with the participant standing in the standardised anatomical position will be recorded following marker placement and prior to movement trials. Markers on the medial and lateral epicondyles of the humeri will be removed following the calibration trial. A 10-camera three-dimensional motion capture system (Vicon, Oxford Metrics Limited, Oxford, UK), sampling at 250 Hz, will be used to track the position of the markers as participants perform each task. Recorded marker trajectories will be smoothed using a low-pass fourth-order Butterworth filter, with the cut-off frequency determined via residual analysis of the marker trajectory data.

Marker set used to collect biomechanical data. Yellow markers indicate those used in static calibration trials only; blue markers indicate marker clusters remaining for dynamic trials; red markers indicate singular markers remaining for dynamic trials.
Participants will complete seven functional tasks representative of activities of daily living involving the shoulder (see table 2).32 These tasks will be performed with the surgical and ‘test’ limb of the experimental and control groups, respectively. The test limb for control participants will be randomly allocated as their dominant or non-dominant arm (as determined by the limb they write with)—with a 50/50 balance achieved for dominant and non-dominant test limbs within the group. Participants will be instructed on functional task start and end positions, but will be able to freely choose their joint postures and speed of movement.32 33
Functional tasks to be used within laboratory-based testing of shoulder joint neuromechanics (adapted from Vidt et al32)
An activity that simulates an overhead sporting task that requires participants to jump and reach to an overhead target will also be performed. The overhead sporting task will consist of a 6-metre run-up, followed by a single-leg jump to reach a ball placed at the participant’s maximal vertical jump height (determined via standardised methods prior to performing this task). The ball will be attached to a specially made ball rig via Velcro, ensuring that the participant can reach and remove the ball during task performance.
Participants will also perform an extreme range of motion trial with their surgical or test limb. This trial will involve the participant keeping the elbow and wrist in a neutral position (ie, arm straight, 0° of elbow flexion, and wrist flexion and deviation) and moving the shoulder to its extreme ranges of motion (within participants’ comfortable limits) in all directions. This motion will be used to create a three-dimensional range of motion ‘globe’ to which the other movement trials can be mapped on.34
All functional, sporting and range of motion tasks will be repeated (with 30 and 60 s rest given between task trials, respectively) until three successful trials are recorded. A successful trial for the functional tasks will be characterised by the participant performing the task with the desired start and end positions, and meeting the task instructions. Successful trials of the sporting task will be characterised by the participant jumping off a single leg, and reaching and removing the ball from the rig in a smooth motion. The order of tasks will be randomised across participants.
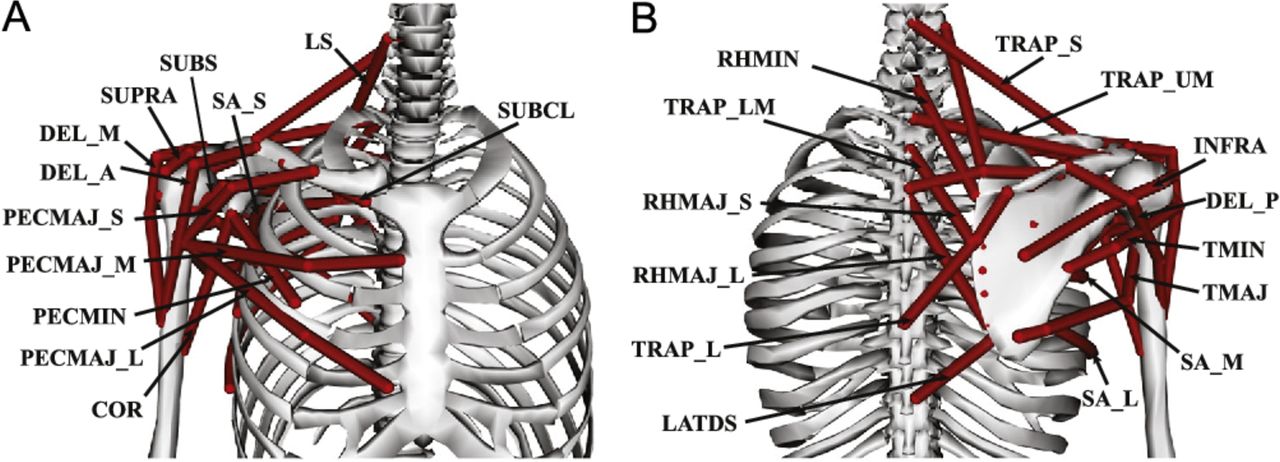
Participant-specific musculoskeletal models of the upper limb will be generated and used in the analysis of laboratory-based biomechanical data from t0 and t2. A generic seven segment (torso, clavicle, scapula, humerus, ulna, radius and hand) musculoskeletal model of the torso and upper limb will serve as the basis for the participant-specific models developed in this study. The kinematic foundation for the model35 36 will describe the kinematics of the shoulder girdle (ie, shoulder elevation, elevation plane and shoulder rotation), elbow (ie, elbow flexion) and forearm (ie, pronation/supination) as recommended by the International Society of Biomechanics.37 Overall motion of the shoulder girdle (including the clavicle and scapula will be determined by the regression equations described by de Groot and Brand,38 and driven by the shoulder elevation angle.35 36 The wrist and finger joints will be locked to minimise the df in the model, which will reduce simulation complexity and computation time. The model will be actuated by 26 Hill-type muscle–tendon units representing the main axioscapular, axiohumeral and scapula–humeral muscle groups (see figure 4).39 Idealised torque actuators will be used to drive elbow and forearm motions. Model parameters (ie, segment inertial properties, muscle strength estimates, muscle attachment points and paths) will be estimated from MRI data using established procedures.40 41 Participants in the experimental groups will undergo MRI scans prior to both laboratory-based testing sessions, with separate models created for each testing session. This approach will ensure the models take into account any changes in shoulder anatomy introduced by the stabilisation procedure. Participants in the control group will undergo one scan at the commencement of the study, with this used to create the model for both testing sessions (as no changes in shoulder anatomy are expected in this group).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Visual representation of muscles included in the upper limb musculoskeletal model. COR, coracoid process; DEL_A, anterior deltoid; DEL_M, middle deltoid; DEL_P, posterior deltoid; INFRA, infraspinatus; LATDS, latissimus dorsi; LS, levator scapulae; PECMAJ_L, lower pectoralis major; PECMAJ_M, middle pectoralis major; PECMAJ_S, superior pectoralis major; PECMIN, pectoralis minor; RHMAJ_L, lower rhomboid major; RHMAJ_S, superior rhomboid major; RHMIN, rhomboid minor; SA_L, lower serratus anterior; SA_M, middle serratus anterior; SA_S, superior serratus anterior; SUBCL, subclavius; SUBS, subscapularis; SUPRA, supraspinatus; TMAJ, teres major; TMIN, teres minor; TRAP_L, lower trapezius; TRAP_LM, lower middle trapezius; TRAP_S, superior trapezius; TRAP_UM, upper middle trapezius.
Biomechanical simulations of the movement tasks will be performed in OpenSim42 (V.4.0) using the MATLAB V.R2019b (MathWorks, Natick, Massachusetts, USA) API and participant-specific models. Torso and upper limb joint angles and moments will be calculated using the inverse kinematics and dynamics OpenSim functions, respectively. Activations and forces of the shoulder muscles during the movement tasks will be estimated using a static optimisation approach. The static optimisation process will aim to minimise the sum of squared muscle and torque actuator activations required to generate the movement, while also constraining the glenohumeral joint reaction force direction.39 This additional constraint aims to simulate rotator cuff muscle co-contraction, and ensures that the calculated muscle forces produce sufficient glenohumeral joint compression and stabilisation.39 Following the optimisation, the joint reaction force function in OpenSim will be used to calculate the glenohumeral joint reaction force applied to the scapula body in the humeral joint coordinate system (x-axis=anterior−posterior; y-axis=superior−inferior; z-axis=medial−lateral). Joint kinematics and moments, muscle activations and forces, and joint reaction forces across each movement will be normalised to a time-scale of 0%–100% of the movement. Joint kinematics of each task will also be used to plot the trajectory of the upper limb (humerus segment) on the globe generated from the extreme range of motion task.34 The area of the globe covered by each movement task will be divided by the total area of the globe, resulting in a percentage representing the amount of shoulder mobility used in the task.34
Glenohumeral stability across the movement tasks examined will be estimated using the direction of the glenohumeral joint reaction force vector in the scapula plane.43–45 The stability of the joint will be defined as a function of the angle of the resultant joint reaction force vector in the glenoid relative to the maximum angle required to reach the outer edge of the glenoid.43 44 The stability value will be calculated at each step across the time-normalised movement tasks. A stability value of zero will occur when the resultant force is directed to the centre of the glenoid, with the stability value increasing towards one (which is the theoretical maximum value that can be reached before dislocation of the joint) as the vector moves towards the outside of the glenoid.43 44 Medical imaging data (ie, MRI) will be used to fit a two-dimensional ellipse to a lateral view of the glenoid fossa surface for calculations of glenohumeral stability.
Shoulder range of motion and strength
During laboratory-based testing (ie, at t0 and t2), participants will also undergo assessment of their shoulder range of motion and strength. Shoulder range of motion will be evaluated in the directions of abduction, flexion, extension (hyperextension), internal and external rotation at 45° of abduction, and external rotation at 90° of abduction. The order for the range of motion tests will be randomised across participants. Participants will be positioned in a dynamometer (Biodex, Shirley, New York, USA) and be instructed to move through their maximum range of motion (ie, to the point where they can no longer move any further) in the specified direction. All directions will be performed with the participant in a seated position (ie, hips and knees at 90° of flexion) with their back firmly pressed against the dynamometer chair. Straps affixed to the dynamometer chair will be placed across the participant’s chest to avoid any movement of the body during the motion. The participant will be positioned so that the axis of rotation of the dynamometer arm is in line with the shoulder joint centre across all tests. The shoulder abduction, flexion and extension (hyperextension) tests will begin with the participant’s arm placed by their side, with the palm in a neutral position (ie, palm facing the thigh), and initiated by the participant moving their arm in the respective directions until the maximum range of motion is reached. Shoulder internal and external rotation range of motion will be tested with the arm abducted to a position of 45° and the elbow flexed at 90°, while external rotation range of motion will be further tested with the arm abducted to a position of 90° and the elbow flexed at 90°. Participants will internally or externally rotate at the shoulder from the starting positions to their maximum range of motion. The displacement achieved from the starting position will be recorded as the participant’s range of motion (in degrees) across all tests. Range of motion tests will be ceased if participants report any feelings of shoulder instability. Following the active range of motion tests driven by participants, a passive test will be conducted by programming the dynamometer to move the participant through their range of motion with no active muscle contraction. The dynamometer will calculate the passive torque (in Nm) generated through the participant’s range of motion in the respective positions and directions. The passive torque generated will be time-normalised to a scale of 0%–100% of the participant’s range of motion.
Strength testing will also be conducted using the dynamometer. Isometric strength in the directions of abduction, flexion and internal/external rotation will be evaluated in a range of positions (see table 3). The dynamometer will be locked in the respective positions for each test. The participant will be instructed to perform a maximal effort concentric contraction by steadily building to maximum effort over 3 s; holding the maximum effort for 1 s and steadily returning to no effort over 3 s. Participants will perform three maximal efforts across each position, with 1 min of rest allocated between each effort to minimise the effect of fatigue. The dynamometer will record the torque (in Nm) produced across each contraction, with the maximum torque achieved across any repetition for the respective movement directions and positions used as the indicator of isometric shoulder strength. All isometric strength tests will be performed on the test limb, with three tests (see table 3) repeated on the opposite side. This will serve as a within-individual comparison of side-to-side strength imbalance between limbs.
Positions and limbs used for each isometric strength test
Eccentric isokinetic strength will be assessed in the directions of flexion and external/internal rotation, in postures associated with anterior instability injuries in contact sport athletes. These tests are designed to assess eccentric strength in shoulder positions associated with anterior instability injuries in contact sport athletes, namely: (1) external rotation in an abducted position46 47 and (2) flexion with an outstretched arm.47 48 The flexion test will involve the participant starting with the arm in a horizontal position in front of the body (ie, 0° of flexion). The test will then involve the participant resisting the motion of the dynamometer with a maximal effort contraction as the shoulder is slowly moved into flexion and relax as the dynamometer moves them back to the starting position. The external/internal rotation test will involve the participant starting with the elbow flexed at 90°, 90° of shoulder abduction and 0° of external rotation. The test will then involve the participant resisting the motion of the dynamometer with a maximal effort contraction as the shoulder is slowly moved into external rotation; and then also resist the motion of the dynamometer with a maximal contraction as it moves them back through internal rotation to the starting position. Isokinetic strength testing will be tested at 60°/s, and as such the dynamometer arm will move at this speed throughout the respective motions. Each isokinetic test will involve the dynamometer arm moving through the dictated range of motion and back for three repetitions, with the dynamometer recording the torque produced (in Nm) throughout the motion. To ensure participants are not placed in a high-risk position for instability, participants will only be tested to positions of 75% of their maximum flexion and external rotation angles. Data from each trials repetitions will be collated and averaged to obtain mean eccentric torque across the different movement directions. The maximum torque achieved across all trials for the different movement directions will be identified and recorded as the peak torque. The order for the different isometric and eccentric strength tests will be randomised across participants, and any test will cease if participants report feelings of instability.
Self-reported shoulder function and health status
Self-report measures of shoulder function and health status will be recorded at all time points (ie, t0, t1, t2 and t3) through an online survey (REDCap, Vanderbilt University, Nashville, Tennessee, USA). Self-reported shoulder function will be assessed using the Oxford Instability Score (OIS)49 and Melbourne Instability Shoulder Scale (MISS)50 ; while self-reported general health status will be assessed using the EQ-5D-5L.51 The three survey instruments will be included within one online survey that participants will complete at the appropriate time points. The survey will be sent to participants in the experimental groups 2 weeks prior to their scheduled shoulder stabilisation procedure and at the follow-up time points. The same schedule will be followed for control participants, with the exception of the first survey being sent to the participant upon study enrolment. The total and section scores for each of the different survey instruments (ie, the OIS, MISS and EQ-5D-5L) will be calculated according to their established methods49–51 for each participant at each time point.
Statistical analysis
Sample size calculations are based on the primary outcome of glenohumeral stability. To our knowledge, no specific data pertaining to the metric of glenohumeral stability are available for individuals following shoulder stabilisation surgery; nor is there any indication in the literature as to what is deemed to be a clinically important difference for this metric. As such, sample size calculations are based on data presented in Marchi et al,45 which examined glenohumeral stability in individuals with a history of shoulder joint dislocation during hand-positioning tasks. Mean and SD in this existing study for glenohumeral stability was 0.655±0.023.45 We have assumed a conservative difference of 5% (ie, 0.033) to represent a clinically important difference. Based on this difference, a sample size of 27 participants (ie, nine per group) is calculated with a power (1−β) of 80% and a type I error (α) of 5%. This study will therefore include a total of 30 participants (10 per group) to meet the computed sample size while allowing for 10% dropout. To compensate for any potential insufficiencies in our a priori sample size calculation (due to lack of comparable studies), we will perform post-hoc power calculations to evaluate any beta error. Additionally, all differences will be presented and interpreted with 95% CIs and effect size estimates.
Data will be compared across groups and time points using a two-way (group×time) analysis of variance (ANOVA) with repeated measures on one factor (ie, time) design or the non-parametric equivalent should data not be normally distributed (as assessed by a Shapiro-Wilk test). The discrete outcome measures of glenohumeral joint stability, shoulder strength, shoulder range of motion and self-report measure scores will be submitted to a traditional ANOVA using the aforementioned design. The continuous outcome measures of joint kinematics and moments, muscle activations and forces, and joint reaction forces will be submitted to an equivalent ANOVA design using vector-field one-dimensional statistical parametric mapping. Relevant post-hoc comparisons (with Bonferroni corrections applied) will be made between groups and time points where ANOVA detects a statistically significant difference (p<0.05 adjusted for the multiple comparisons made). The 95% CIs and estimates of effect sizes (ie, Cohen’s d) will also be calculated for differences between and within groups across the time points.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
References
Footnotes
Twitter @aaron_s_fox
Contributors AF and RSP conceived the study. AF oversaw manuscript writing and submission. AF, JB, SDG and RSP contributed to the design of the study protocol, assisting with drafting the manuscript, and have read and approved the final version of the manuscript.
Funding This work is partially supported by a Deakin University Postdoctoral Research Fellowship grant (held by AF). Funding will be used to pay for costs associated with data collection and analysis.
Competing interests RSP receives institutional educational support from De Puy Synthes, New Brunswick, New Jersey, USA. AF, JB and SDG report no competing interests.
Patient consent for publication Not required.
Ethics approval This study will be conducted in accordance with the Declaration of Helsinki and the Australian National Health and Medical Research Council’s National Statement on Ethical Conduct in Human Research. The study protocol has been approved by the Barwon Health (project number 19-53) and Deakin University Human Research Ethics (project number 2019-419) committees. All collected data will be stored electronically using a re-identifiable coding system for participants. This will ensure that data are stored and used in the strictest confidence and will not reveal participant identity. Electronic data will be stored on secure servers only accessible to the project lead and associate investigators. The results will be submitted for publication in peer-reviewed journals and for presentation at relevant scientific conferences. Where appropriate, we also aim to disseminate the results through relevant media outlets (eg, specialised magazines, websites). No data or participant information will be identifiable in the disseminated results. Any specific individual data reported will be non-identifiable.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. This paper represents a study protocol, hence no data have been collected.