Article Text

Abstract
Introduction Physical activity (PA) interventions have been introduced in patients with cancer as they may contribute to better treatment outcomes and quality of life (QoL). However, little is known about the impact of PA on patients with bladder cancer (BC). This scoping review aimed to explore efficacy and feasibility of existing PA interventions in the BC care pathway.
Methods and analysis Preferred Reporting Items for Systematic Reviews and Meta-Analyses Scoping Review guidelines and the Levac methodology framework were used; electronic databases were searched. Two independent reviewers screened all titles, abstracts and full-text publications for inclusion. The feasibility of integrating a PA intervention in the BC treatment pathway was discussed in a consultation phase with healthcare professionals and patient and public representatives.
Results A total of 675 records were identified through database searching of which 14 studies were included in our scoping review. An additional 17 clinical trials were identified of which 12 were included for which no results have been published yet. The included studies looked at the feasibility of a PA intervention programme, the associations between PA, obesity and BC, but also the determinants of PA engagement for BC patients and the assessment of QoL.
Conclusion This scoping review highlights that despite the general recognition on the role of PA in the BC treatment pathway, there is a gap regarding the understanding of the impact of PA interventions in BC care pathways as well as the limited understanding of factors underlying possible benefits of PA. No clear conclusions could be made regarding structure and processes of PA interventions that may lead to better outcomes. Further PA studies for patients with BC are needed to understand how to incorporate exercise guidelines recommendations.
- sport and exercise psychology
- urology
- cancer
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings?
Physical activity (PA) should be included in the bladder cancer (BC) preoperative and postoperative treatment pathway.
The benefit of multimodal PA interventions in BC care pathways should be further investigated.
Biological mechanisms and factors underlying possible benefits of PA in the BC care pathway have to be explored.
Background
Recognition of the impact of physical activity (PA) for people affected by cancer has expanded in recent years. Several studies have shown the potential of PA at all stages of the cancer care pathway.1–3
More specifically, PA interventions have been introduced in the cancer patient pathway to help improve treatment outcomes and increase health-related quality of life (HRQoL).4 The WHO defines HRQoL as a multidimensional concept that includes domains related to physical, mental, emotional and social functioning and focuses on the impact health status has on quality of life.5 A related concept of HRQoL is well-being, which is a broader concept that assesses the positive aspects of a person’s life including life satisfaction.6
Several studies have demonstrated that PA should be part of the standard cancer care and treatment as it may improve disease-related physiological and psychological outcomes in cancer patients; this is mostly due to the reduction on drug toxicity levels and increases treatment completion rates.2 For example, an analysis by Holmes et al7 in the Nurses’ Health Study highlighted that engagement in sufficient vigorous PA following breast cancer diagnosis was inversely associated with breast cancer specific mortality risk. A recent Cochrane review looked at the association between the intensity of PA and the effects on HRQoL; it was concluded that the greater the intensity, better HRQoL scores including factors such as social functioning and fatigue.8 The potential benefit of PA in treating patients with cancer has been linked to several mechanisms such as enhanced immune response, body composition, tumour vascularisation and tryptophan metabolism regulation.2
The potential benefits of PA on bladder cancer (BC) management has not been studied comprehensively as in other cancers; there is currently one review focusing specifically on those patients who have undergone a radical cystectomy, which is only affecting a subgroup of patients with BC.9 As highlighted in our recent research prioritisation work, although it is ninth most common cancer worldwide, with about 18 000 people being diagnosed annually in the UK alone,10 BC is an under-researched cancer.11 The 2015 National Institute for Health and Care Excellence BC guidelines concluded: ‘There is considerable variation in provision of BC care and evidence that the patient experience for people with BC is worse than that for people with other cancer’.12 13
Scoping reviews are a useful tool to determine the coverage of the literature on a given topic and have an indication of the studies available as well as an overview of its focus. Scoping reviews help to clarify emerging evidence and pose more specific questions.14 Therefore, by conducting this scoping review, we aimed to explore efficacy and feasibility of existing PA interventions in the BC care pathway and to identify the gaps in the current work on the influence of PA on BC management.
Methods
To explore the efficacy and feasibility of existing PA interventions in the BC care pathway and to identify the gaps in the current research on the influence of PA on BC management, a detailed protocol of this scoping review has been published elsewhere15 and a brief summary is presented in figure 1. Briefly, our methods were developed based on the Joanna Briggs Institute guidelines,16 and the methodological guidelines were developed by Levac et al.17 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses Scoping Review extension for scoping reviews18 was followed to ensure that all suggested items are reported. A clinical research team was consulted to define the research questions. MEDLINE (using the PubMed interface) and Ovid Gateway (Embase and Ovid), the Cochrane Library, and PsycInfo and Global Health and Healthcare Management Information Consortium were searched for relevant studies between6 A separated search was conducted on ClinicalTrials.gov using the same search strategy. All types of study design were considered for inclusion if they assessed clinical/HRQoL and feasibility outcomes in patients who had a primary diagnosis of BC and PA had been measured (either as part of their lifestyle or as part of an intervention in the treatment pathway). Studies will be excluded if the publication is any other language than English or if the study was not relevant or had a wrong study design. Two other independent reviewers analysed the studies included/excluded and discussed any conflict until a final consensus was obtained; however, no conflicts occurred, and the results of both reviewers were the same. The studies found were analysed using a qualitative and quantitative method. For qualitative aspects, the Donabedian conceptual framework19 was used to assess the possible efficacy of the PA interventions reported by analysing the structure, process and outcomes.
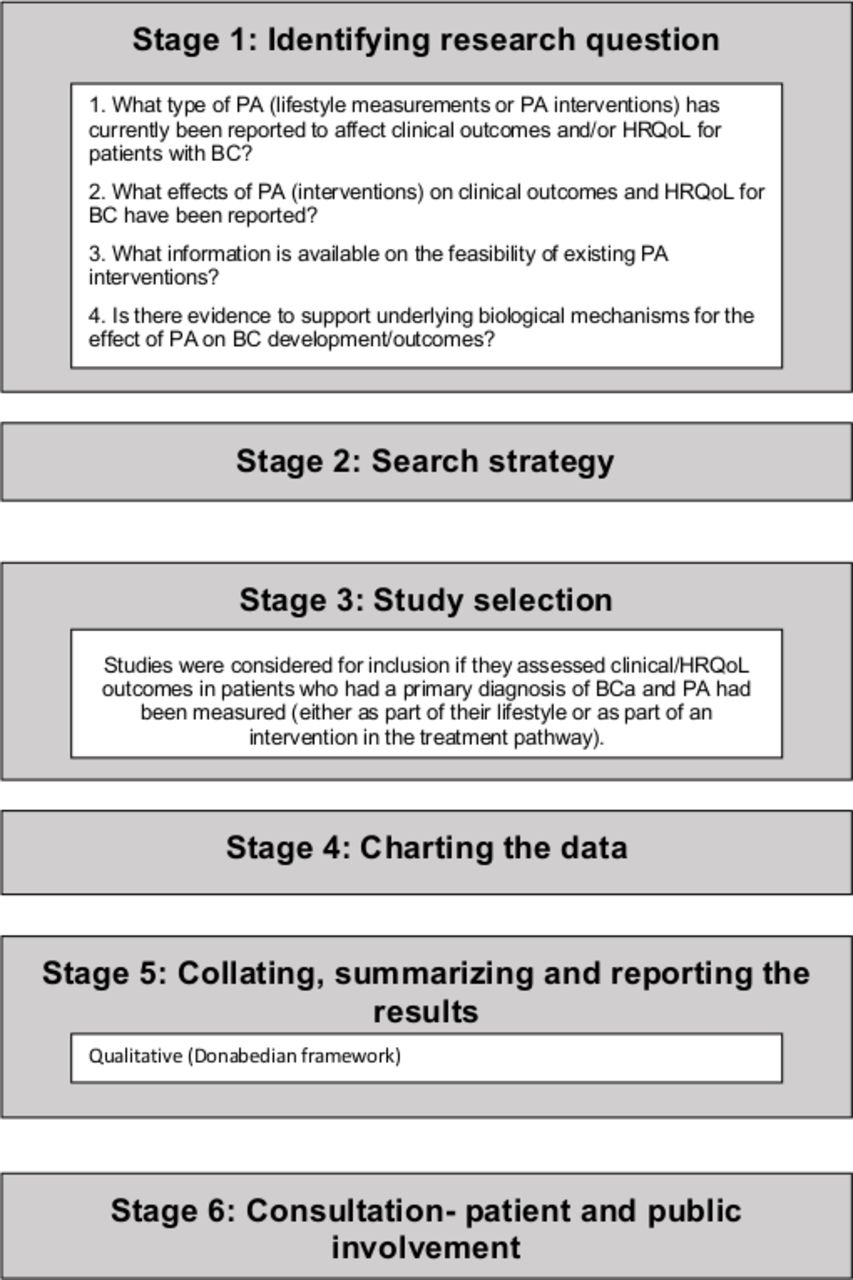
Stages of the scoping review. BC, bladder cancer; HRQoL, health-related quality of life; PA, physical activity.
To ensure that our findings are relevant to those affected by BC and their healthcare professionals, the results were synthesised, presented and discussed in a consultation phase with a clinical oncologist, a medical oncologist, a BC nurse specialist, clinical research nurses, a psychologist as well as patients and patient and public involvement representative.
Results
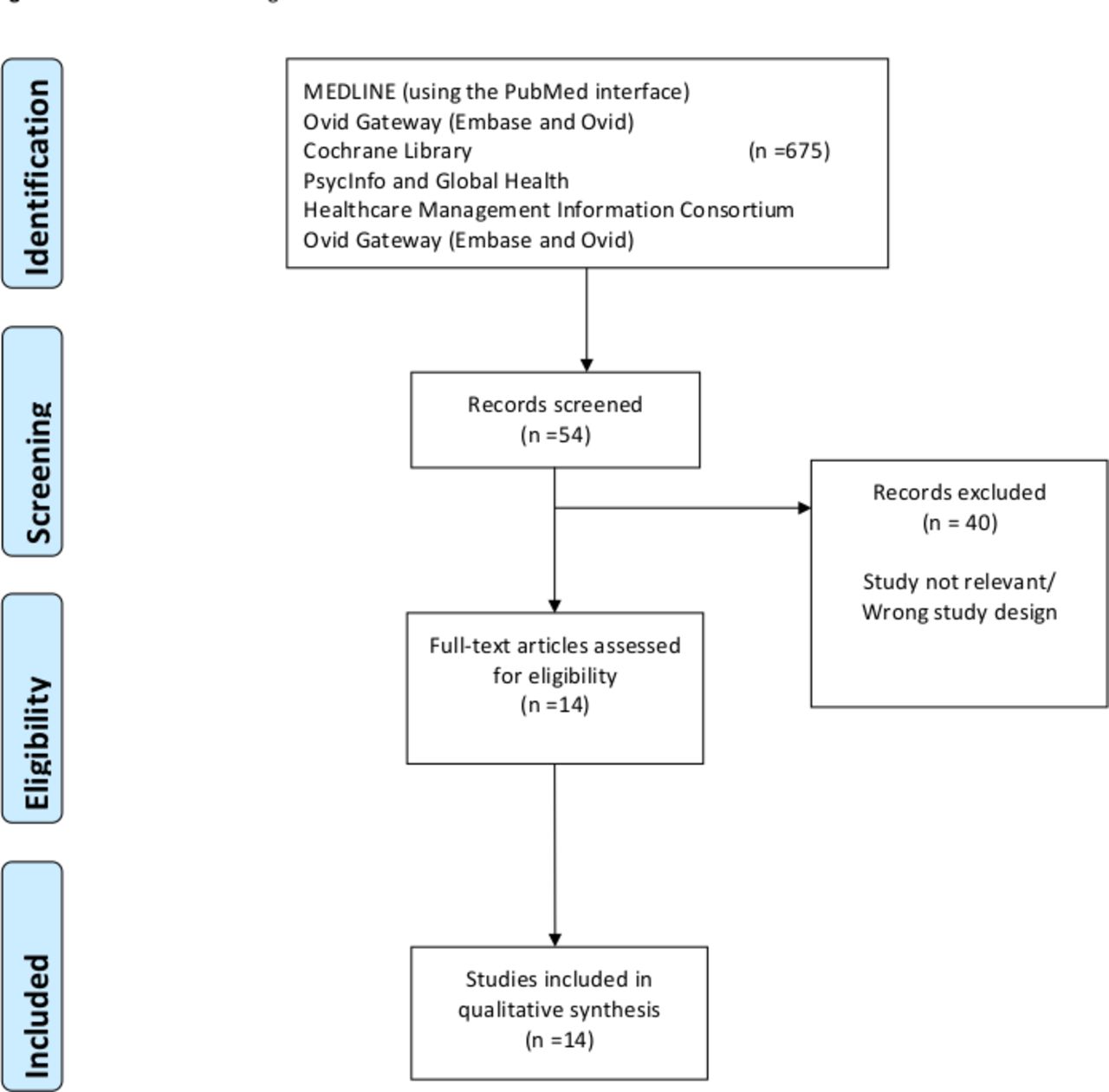
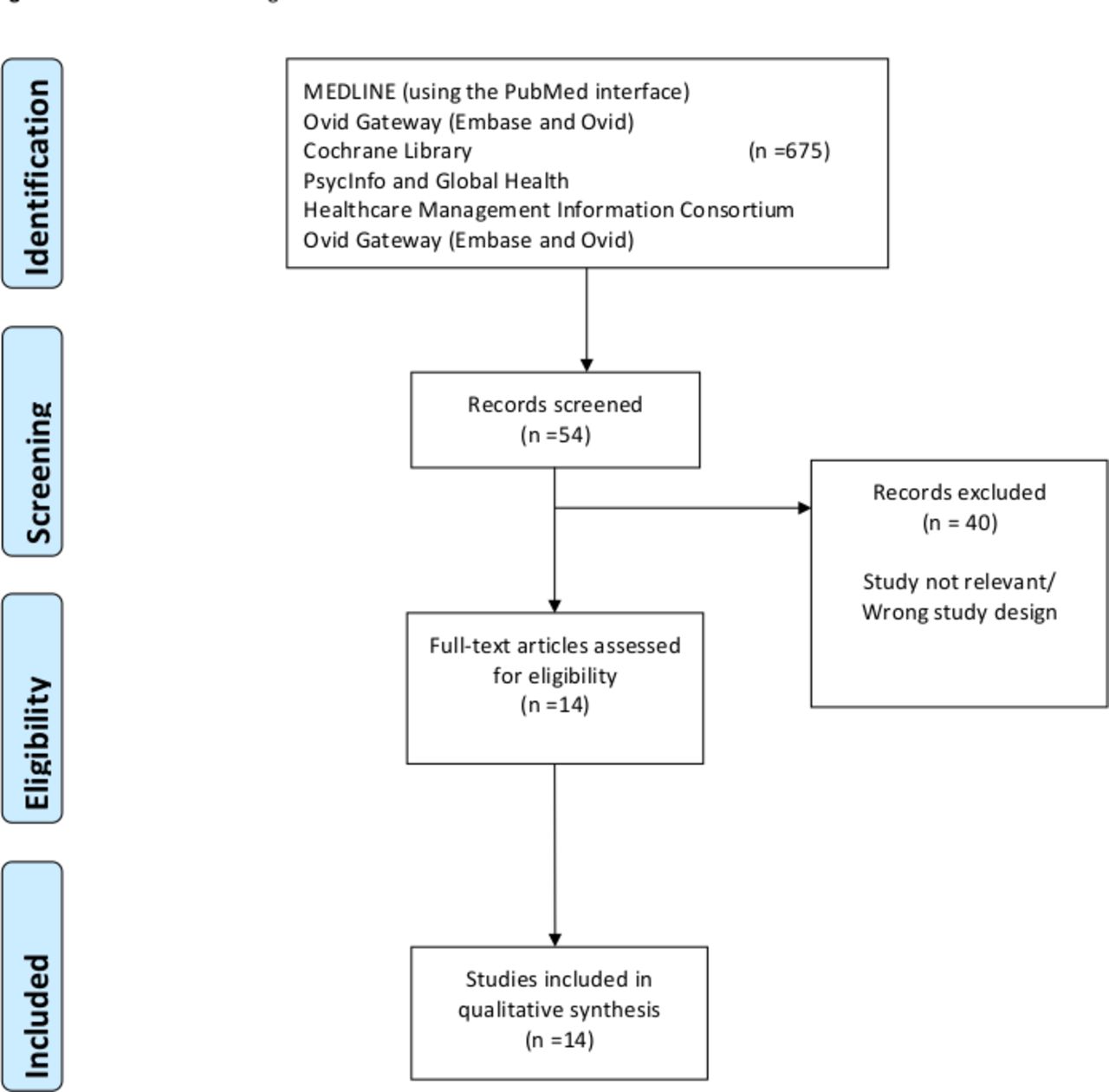
A total of 675 records were identified through database searching. After screening by title and abstracts, 54 were assessed for eligibility. In total, 14 studies matched the inclusion criteria and were included in this scoping review for qualitative synthesis (table 1). Figure 2 shows the flow chart of this scoping review. Four studies were conducted in Canada, two in Denmark, four in the USA, two in the UK, one in Sweden and one in Belgium. Of those, six were randomised controlled trials (RCTs), six were cohort questionnaires/surveys and two were interviews/semistructured interviews. From the ClinicalTrials.gov search, 17 studies were identified and assessed for eligibility and 14 studies coincide with the inclusion and exclusion criteria; of those, three had no information on location,20–22 one was in Sweden,23 five in the USA,24–28 one in France,29 one in Belgium and one in Canada.30
{kind=link}
{kind=link}
PRISMa flow chart diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Descriptive table of the studies included in the scoping review
Table 1 summarises the included studies. All RCTs had feasibility of a PA programme as their primary outcome; one also included cardiovascular outcomes.31 The interview studies evaluated the associations between PA, obesity and BC and the determinants of PA engagement in patients with BC.32 33 The questionnaires/surveys evaluated the associations of PA and QoL. The prospective cohort studies evaluated underlying biological factors such as body mass index (BMI) and glucose and one study also evaluated the cardiovascular component, in addition to the effect of PA.34–36
Overall, the studies in table 1 reported that PA helped to provide improved QoL, but in one study, a physical rehabilitation programme, it was found to not impact on HRQoL.37 However, the same study showed that preoperative and postoperative physical rehabilitation provide better results on HRQoL. In addition, another study showed that BC survivors are more interested in an exercise programme specially designed for them in a physical presence format.38 One study supported that multimodal prehabilitation resulted in faster functional recovery after radical cystectomy.39 Regarding oncological outcomes, BC mortality was noted lowest in those patients who obtained the recommended amount of exercise as compared with no exercise. Patients with BC responded well to aerobic exercise, and it is suggested that improvements in cardiopulmonary/cardiorespiratory fitness variables could have important implications for postoperative recuperation after RC.31
Table 2 shows the data extraction for studies that looked at PA and suggested hypotheses for potential underlying biological mechanisms. Both studies looked at preoperative cardio exercise31 34; patients with BC responded well to the aerobic exercise training, including the elderly population; patients were compliant with a supervised exercise regime, and it was concluded that the improvements in cardiopulmonary fitness variables could have important implications for postoperative recuperation after RC.31
Studies that evaluate PA and proposed potential underlying biological mechanisms
Table 3 summarises the qualitative Donabedian conceptual framework of the included studies where information on process and structure of a PA intervention was provided. Positive outcomes were shown in the studies that included a multimodal approach and aerobic exercise,39 but no conclusions could be made regarding what structure and processes lead to the better outcomes for patients with BC.
Donabedian conceptual framework of the included studies
Table 4 summarises the clinical trials currently listed on ClinicaTrials.gov. Four have been completed, but no results have yet been published.22 25 26 40 Two still need to start recruiting,41 42 four are currently recruiting20 21 29 43 and two have an unknown status23 29 (table 4).
Clinical trials on PA
To guarantee that our assessment (tables 1–4) is relevant to those affected by BC and their healthcare professionals, we also organised a consultation with patients, their family members and healthcare professionals. We held a face-to-face meeting in January 2020 with a clinical oncologist, a medical oncologist, urological surgeon, three nurse specialists, a physiotherapist, a patient and public involvement specialist and three patients (one male and two female) to discuss the feasibility of a PA component in an intervention for patients with BC. The findings of the scoping review were discussed, and it was concluded that PA should be included as part of a multimodal approach to support patients’ well-being by combining PA support with other components of well-being such as mental or sexual well-being. A well-being intervention including PA, sexual and mental well-being support is currently in development.
Discussion
Of the 14 studies included in our scoping review, six were RCTs, six were cohort questionnaires/surveys and two were interviews/semistructured interviews. All RCTs had feasibility of a PA programme as their primary outcome, and the interview studies evaluated the associations between PA, obesity and BC as well as the determinants of PA engagement in patients with BC. The questionnaires/surveys evaluated the associations of PA and quality of life. The prospective cohort studies evaluated underlying biological factors such as BMI and glucose in addition to PA. Nevertheless, no conclusions could be made regarding structure and processes of a PA intervention that could lead to better outcomes for BC patients. Moreover, although some clinical trials have been identified through ClinicalTrials.gov, no results have yet been published.
There is a increasing number of studies suggesting a potential benefits of PA at all stages of the cancer care pathway.1 Looking at patients with BC in particular, our findings support this recommendation with studies showing the important implications of a preoperative and postoperative physical rehabilitation with most studies on aerobic/cardiovascular exercises. More studies are needed to evaluate the benefits of other types of exercises in relation to different BC treatments and time points. As PA may be part of BC treatment pathway, PA integrating exercises to strengthen pelvic floor and improve continence should be considered.
The benefits of prehabilitation activities for patients with cancer in general are well documented.35 44 In the context of BC, preoperative interventions have been found to be feasible and acceptable. However, few studies evaluated the underlying biological mechanisms of PA effects in the context of radical cystectomy and survival. The studies that aimed to clarify the underlined biological mechanisms focused on increasing the aerobic/cardiovascular/cardiopulmonary capacity of those patients.16 17 However, they mainly focused on the short or intense implications of PA, and it would be interesting to evaluate the effect of long-term PA in terms of biological mechanisms and its implications in BC response to treatment and survival.
It is known that after a cancer diagnosis and during medical treatments, it is difficult to become physically active.45 Rammant et al9 explored the determinants of PA in patients with BC before and after radical cystectomy and, as per other cancer types, concluded that the PA behaviour in patients with BC is multifactorial. Minnella et al39, in their RCT, also concluded that a multimodal prehabilitation approach resulted in faster functional recovery after radical cystectomy. These observations also support the points highlighted during our consensus meeting regarding the need for a multidisciplinary approach that also incorporates mental and sexual well-being to support patients with BC. PA activity is positively associated with HRQoL in BC survivors, and therefore, it would be interesting to further evaluate the underlying reasons that support that association. As explained above, HRQoL is a multidimensional5 concept that includes domains related to physical and mental well-being; it focuses on the impact health status has on quality of life.
From the literature review and the consultation phase, we can conclude that there are many questions to be answered concerning PA and BC. For example, which patients with BC would benefit the most from engagement in PA in terms of survival and quality of life?46 Moreover, there is a need to understand which types of PA are needed and when they should be included during the BC treatment pathway. Given the high level of physical inactivity in the population, especially in a more elderly population such as patients with BC, it should be considered priority to understand how to implement PA in this group of patients.6 Our consultation phase with patients and HCPs confirmed the need to include a multimodal approach developing PA interventions.
Our extensive search through different databases, allowing for the inclusion of all types of interventions focused on PA, quality of life and biological mechanisms, is a strength of this scoping review. Another strength is the inclusion of a consultation phase that allowed to discuss the findings with patients and healthcare professionals. However, due to the nature of the methods used of the included studies and the lack of information in these published study designs, we were unable to provide a conclusion regarding the structure and processes of PA interventions that lead to better clinical outcomes for patients with BC. Future studies should better report on the development of their intervention, the different components and the processes followed. Additionally, the studies that analyse the possible underlying biological mechanisms to support the benefits of PA are limited, restricted to short period of time before BC treatment and no conclusion could be made on the long-term benefits of PA. Moreover, it is important to highlight that we did not identify any studies conducted in low-income or middle-income countries or non-western countries. Also, no multinational studies have been conducted.
Conclusion
This scoping review highlights the gap regarding the understanding of the impact of PA interventions in the BC pathway. It also highlights the limited understanding of the factors that are underlying the possible PA benefits, such as psychological aspects and biological components. Further PA studies for patients with BC are needed to understand where and how to incorporate the global WHO recommendations on PA.
Acknowledgments
The authors gratefully acknowledge the helpful comments from the bladder cancer patient support group.
References
Footnotes
Twitter @_LouisFox
Contributors Conception and design: AB, CB and MVH. Acquisition of data: AB, CB, SM, MR and HZ. Analysis and interpretation of data: AB, CB and MVH. Drafting of the manuscript: AB and CB. Critical revision of the manuscript for important intellectual content: BR, LF, KB, ER, SA, KC, NP, CH and MVH.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository.