Article Text

Abstract
Background/aim The purpose of this study was to compare the isokinetic peak torque profiles from the quadriceps and hamstrings muscles during concentric and eccentric contractions in elite Brazilian soccer players across different field positions and age categories. Our hypothesis was that soccer players from different field positions are subjected to different ageing-related effects on their isokinetic peak torque.
Methods This is a retrospective study based on professional elite-level soccer players between the years 2009 and 2019. It included 570 adult males who played for at least 5 years on first or second Brazilian divisions. Playing positions were divided as: goalkeepers, defenders, sidebacks, midfielders and forwards. Age categories were also divided as: G1 (17–20 years old), G2 (21–24 years old), G3 (25–28 years old), G4 (29–32 years old) and G5 (33 years old or more).
Results The results indicate a moderate effect of age (F(4545)=8.197; p<0.001; η2=0.057) and a small effect of playing position (F(4545)=2.993; p<0.05; η2=0.021) on torque of concentric extensors; mainly from midfielders and goalkeepers with 29 years or more.
Conclusions Soccer players from different field positions are subjected to different ageing related effects on their muscular performance during their career special attention should be given to these players to avoid reduction in physical performance.
- aging
- assessing physical training modalities in enhancing sports performance
- athlete
- biomechanics
- soccer
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- aging
- assessing physical training modalities in enhancing sports performance
- athlete
- biomechanics
- soccer
What are the new findings?
Professional soccer players of different playing positions have different muscular strength losses with ageing.
Midfielders and goalkeepers are more subjected to strength losses than other playing positions.
After 29 years, the knee extension strength losses increase for goalkeepers and midfielders.
Introduction
Reference values for muscle strength characteristics in different athlete populations are important for coaches, athletic trainers, sports physicians, physical therapists and others health allied professionals who are responsible for the athletes’ health and safe return to play.1 Establishing reference values for muscle strength characteristics in soccer, allows comparison between players. Reference values may also provide a better understanding of normal variation within a given position.
Reference values must be adjusted according to age (ref). Namely, one of the most important physical characteristics of soccer players, lower-limbs muscular strength, is usually affected by ageing, affecting the player’s performance.2 3
Isokinetic peak torque (PT) assessment is one of the most common evaluation method for lower extremities muscle strength in soccer.4–7 Some authors even suggest it as a diagnostic tool for sports injury prevention and rehabilitation.8–11 However, little information is available about the reference values of PT in soccer players according to their age and playing position.
Therefore, the purpose of the current study was to compare the isokinetic PT of quadriceps and hamstrings, during concentric and eccentric muscle contractions in elite Brazilian soccer players across different field positions ages. Our hypothesis is that soccer players from different field positions are subjected to different ageing-related effects on their isokinetic PT.
Methods
This is a retrospective study based on isokinetic data and clinical records from Brazilian professional elite-level soccer players between the years 2009 and 2019. This study followed the recommendations of The Strengthening the Reporting of Observational Studies in Epidemiology Statement12 and its design followed the recommendations of the Improving Healthcare Decisions Task Force (Professional Society for Health Economics and Outcomes Research (ISPOR) Retrospective Database Recommendations).13 ,14 The purpose, experimental procedures, possible risks and benefits of the study were explained to the athletes, who provided a written informed consent form to confirm participation in the study. For players younger than 18 years, their parents or legal guardians were informed of the risks and signed an informed consent before investigation enrolment.
It included 570 elite professional soccer players who had been playing for at least 5 years on first or second Brazilian divisions, training regularly one to two sessions per day, six times per week.
To be included in this study, players had to be able to fully participate in team training sessions and matches. Players who had a hamstrings or quadriceps muscle injury in the past 3 months, a knee surgery in the past 12 months, or were under treatment from other painful musculoskeletal injuries were excluded from our sample. Players with tendon or muscle injury grade I and without symptoms at rest were allowed to participate in the study. Only players who had played in their usual positions for the last year were included in the study.
Participants were requested to eat according to their team’s nutritionist diet 48 hours preceding the assessment and then refrain from eating and drinking substances other than water 1 hour before testing. All tests were carried out in January, few weeks before Brazil Regional Championships’ season starts. Players were also instructed to refrain from strenuous activities 48 hours before testing.
For evaluation of the PT an isokinetic dynamometer (Cybex-CSMI (Computer Sports Medicine Inc), model HumacNorm 2009, Stoughton, Massachusetts, USA) with signal acquisition rate of 500 Hz was used. To improve patient’s understanding of the test, we used a modified 10-points Borg scale for strength effort15; and a 10 cm Visual Analogue pain Scale (VAS), where ‘0 cm’ indicated ‘no pain’ and ‘10 cm’ indicated ‘worst imaginable pain’.16 For data storage and processing was used a Macbook Pro Notebook (Cupertino, California, USA) equipped with Microsoft Office software package for Mac (V.2011, Redmond, Washington, USA) and SPSS (V.20.1) from IBM.
On arrival, participants were provided with appropriate explanation and demonstration of all procedures. Participants informed their playing position, as the most frequently played in the past year. Positional groupings were goalkeepers (G), defenders (D), sidebacks (S), midfielders (M) and forwards (F). Dominant leg was defined as their preferred kicking leg for a penalty kick. Anthropometric information was recorded by team’s medical staff before the participants completed a standardised warm-up on the isokinetic machine.
All subjects were submitted to a testing protocol following the guidelines of American Physical Therapy Association17–20 and soccer-specific studies using isokinetic machines.5 7 21 The same physiotherapist, with 10 years of experience, performed all tests. The isokinetic machine was calibrated followed manufacturer’s manual instructions.
Participants seated on the isokinetic machine chair with lumbar spine fully supported and hip in 85° of flexion. The knee joint axis of rotation was aligned with the axis of the arm attached to the isokinetic machine. The dominant leg was tested first. The isokinetic machine lever arm length was adjusted so the contact point (Pad) was positioned one centimetre above the lateral malleolus; allowing free ankle flexion and extension during the test. The participant executed 10 concentric repetitions of knee’s extensor (Ext) and flexor (Flx) muscles at 90° per second (100° arc of motion) for familiarisation and warming up (Borg up to 5, VAS up to 1); following by a rest period of 120 s. The warm-up on the isokinetic machine was chosen to improve specificity and familiarisation with the following test (ref). The participant performed five concentric repetitions of knee’s Ext and Flx muscles at 60° per second during a second familiarisation and warm up session, following by another rest period of 120 s. Immediately after, the subjects performed three concentric repetitions of knee’s Ext and Flx muscles at 60° per second (100° arc of motion) with maximum effort (Borg 10), receiving constantly the standardised verbal encouragement: ‘Faster’. The presence of pain equal or superior to 4 on VAS interrupted the test (excluding the participant from study). The repetition with higher torque value (PT) among all the three repetitions was used for statistical analysis. The eccentric testing was performed at 60° per second (100° arc of motion). The subject executed five repetitions of warm-up and familiarisation followed by three repetitions at maximum effort (Borg 10), constantly receiving the standardised verbal encouragement: ‘Hold it’. The presence of pain equal or superior to 4 on VAS interrupted the test, excluding the participant from the study. Between each set of exercises, subjects had 90 s to rest. Between each limb’s test, subjects had 120 s to rest.
Demographic data as age, age category, height, body mass, dominance, field playing position (position) were recorded for descriptive analysis (mean±SD). Position was divided as: goalkeepers, defenders, sidebacks, midfielders and forwards. Age categories were also divided as: G1 (17–20 years old), G2 (21–24 years old), G3 (25–28 years old), G4 (29–32 years old) and G5 (33 years old or more).
Concentric peak torque (CPT) and eccentric peak torque (EPT) of right and left knee Ext and Flx were extracted from the isokinetic machine in Newtons (N/m). From these data, variables were organised as means of right and left leg in: Ext.CPT and Ext.EPT, Flx.CPT, Flx.EPT. All data were normalised by body mass in kilograms.
Data’s normality was confirmed using visual inspection (Q-Q plots) and the Kolmogorov-Smirnov tests. Homogeneity of variance was assessed via Levene’s Test. Data with normal distribution were subjected to a two-way analysis of variance (ANOVA). Data with non-normal distribution were subjected to Kruskal-Wallis analysis. Post hoc analysis used Bonferroni test, adjusted for multiple comparisons for non-normalised data. Size effects was measured through between subjects partial-eta square (η2). The magnitude was categorised as small (0.01), moderate (0.06) and large (0.14), respectively.22 23 All data were processed using a SPSS V.20 (IBM) with statistical significance set at alpha level p=0.05.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Demographic and anthropometric characteristics for all participants are provided in table 1. After applying inclusion and exclusion criteria, a sample of 1083 screened candidates were reduced to 570 healthy, male, elite-level, professional soccer players.
Demographic and anthropometric characteristics of the sample distributed by playing position and age category; with means and SD
Results of the Kruskal-Wallis analysis revealed that only Forwards and Midfielders do not have significant differences in height (X2(4)=233.21; p>0.05), when compared with other playing positions. Also, Goalkeepers from G3, G4 and G5 have significant differences (heavier) in body mass (X2(4)=233.21; p<0.001), when compared with other age categories.
Table 2 shows mean values of normalised knee Ext and Flx, from concentric and eccentric contractions of each age category and playing position. The statistically significant results from inferential analysis are presented in table 3. The two-way ANOVA analysis indicates a moderate effect of age (F(4545)=8.197; p<0.001; η2=0.057) and a small effect of playing position (F(4545)=2.993; p<0.05; η2=0.021) on Ext.CPT. Figures 1–4 show the changing in PT of each playing position through all five age categories.

Extensor concentric peak torque of all playing positions through all five age categories.
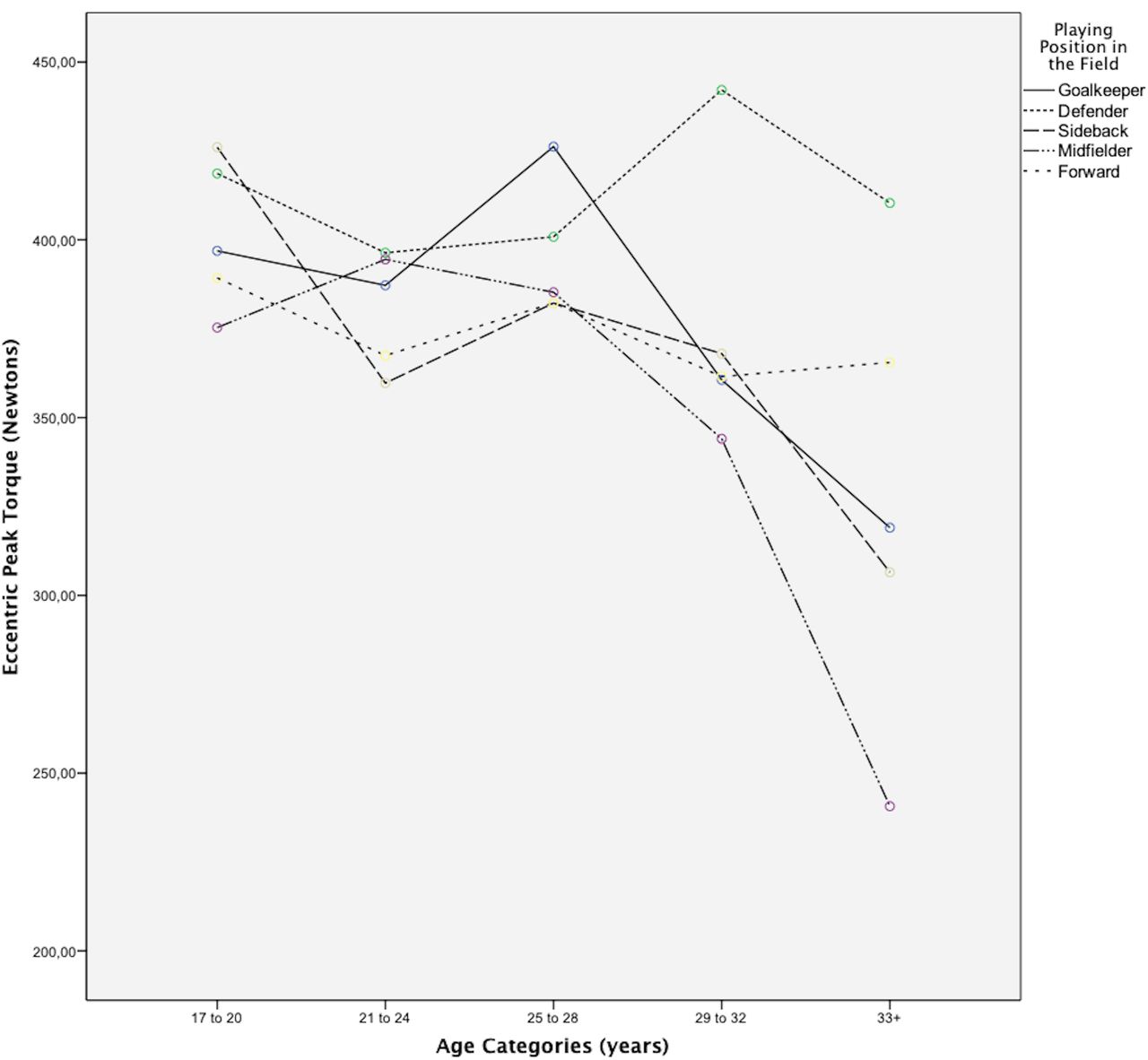
Extensor eccentric peak torque of all playing positions through all five age categories.

Flexor concentric peak torque of all playing positions through all five age categories.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flexor eccentric peak torque of all playing positions through all five age categories.
Concentric and eccentric isokinetic peak torque of knee flexors and extensors, for each playing position and age category; with normalised by body mass means and SD
Inferential analysis of statistically significant differences in peak torque for each playing position and age category
The Bonferroni post hoc analysis indicates that goalkeepers of G5 have a Ext.CPT statistically different from goalkeepers of G3 (95% CI −1.359 to −0.014: p<0.05), G2 (95% CI −1.263 to −0.083: p<0.05) and G1 (95% CI −1.284 to −0.087: p<0.05). Midfielders of G5 have a Ext.CPT statistically different from midfielders of G2 (95% CI −1.263 to −0.083: p<0.05) and G1 (95% CI −1.284 to −0.087: p<0.05). Midfielders of G4 also have a Ext.CPT statistically different from midfielders of G3 (95% CI −0.581 to −0.043: p<0.05), G2 (95% CI −0.745 to −0.191: p<0.001) and G1 (95% CI −0.689 to −0.104: p<0.001).
Discussion
The aim of this study was to compare isokinetic PT profiles of quadriceps and hamstrings, from concentric and eccentric muscle contractions in elite Brazilian soccer players across different field positions and through all age categories. Our hypothesis is that soccer players from different field positions are subjected to different ageing-related effects on their muscular performance.
Some scientific studies have analysed the effects of ageing on the physical performance markers of professional-elite soccer players.2 3 24–34 However, to the best of our knowledge, there is no study that analysed the effects of ageing on isokinetic strength values of soccer players according to their playing positions on the field. The closest to this subject was the study by Slimani and Nikolaidis31 which made a systematic review of anthropometric and physiological characteristics of male soccer players according to their competitive level, playing position and age group. However, they mentioned only three studies with limited comparative isokinetic or strength data.Therefore, we believe this 10-year retrospective research, with a sample of 570 elite, healthy, professional male soccer players, was the first to be made.
Two studies2 3 with 14 546 professional soccer players of the German league (Bundesliga) and 10 739 from Spanish league (La Liga) have similarities with our study design. However, there was no measurement of PT of those players, evaluating instead their movement during matches and calculating the number of fast runs, total distance travelled and number of sprints. Similar to our findings, they report a decrease in player’s physical performance after 30 years old when compared with players from younger age categories. The performance reduction in fast runs and sprints was most notably in midfielders. Our results indicate a significant reduction in quadriceps strength of midfielders with 29 years old or more; when compared with younger players. As quadriceps is an important muscle to running and sprinting activity, this aging-related weakness may contribute to decrease in performance as running and jumping are associated with muscle strength. Nonetheless, the aforementioned studies used a different classification of playing positions; subdividing midfielders in two subcategories: central midfielders and wide midfielders. The last, could be confound with the Brazilian definition of Forward, used in our categorisation procedure.
Muscular weakness is related to muscle injury risk in soccer.35 This is one of the reasons why isokinetic testing is largely used for screening injuries in professional soccer.8 36 Our results showed reduction in quadriceps strength of midfielders and goalkeepers during the advancing in age categories. Another study34 evaluated muscles injuries on 64 professional soccer players, divided in two age groups: players younger and older than 23 years. No significant differences of the age groups were found in terms of the number of muscle injuries when it comes to the quadriceps, the hamstrings. However, since their small sample size and no distinction between playing positions, comparisons with our results are, at least, difficult to make. According to a study develop by Schuth and collaborators,24 positional interchanges influence physical and technical performance variables of soccer players, so its performance could be wrongly underestimated by a recent change in playing position.
Conclusions
Isokinetic PT of knee Ext, from concentric muscle contractions, has a small difference between playing positions, and a moderate effect of age in healthy professional elite-level Brazilian soccer players. Midfielders and goalkeepers are the playing positions more affected by ageing, with significant reduction of strength after 29 years when compared with younger player categories.
Limitations
Unfortunately, standardisation of playing positions between different soccer leagues is difficult, as sidebacks could be considered defenders, or forwards could be divided in strikers and forwards. Future researchers may correlate these findings with their isokinetic data and regional soccer culture to use as references or guidelines.
Practical applications
These results suggest that a special attention should be applied to midfielders and goalkeepers concentric extension strength after 29 years old; to avoid physical and match performance reduction and to optimise muscle injury risk prevention.
Supplemental material
Supplemental material
Acknowledgments
We declare that all authors were fully involved in the study and preparation of the manuscript and that the material within has not been and will not be submitted for publication elsewhere.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Edgar47414998
Contributors Conceptualisation: RS. Study design: RS, RB. Data collection and extraction: RB, LMAF and BMOA. Data management: RB and LMAF. Data analysis: RAdS and EV. Supervision: CFA. Writing-original Draft: RS, RB and LMAF. Writing-review and editing: RH.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was carried out according to the Declaration of Helsinki, following the Ethical Standards in Sports and Exercise Science Research. A protocol was fully approved by the University Human Research Ethics Committee of our university with number #3 652 668.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Participants data were not allowed to be shared as it contain renomed professional athletes and different soccer teams enrolled.