Article Text

Abstract
Knowledge from research evidence is wasted unless it is applied. While the scientific evidence base for many sports and exercise medicine and sports physical therapy interventions is robust, real-world implementation and evolution to scale remains an ongoing challenge. Dissemination and implementation research is important to generate evidence-informed, cost-effective and context-specific strategies for implementation partners and stakeholders to effectively apply and sustain the best research evidence in public health and clinical practice. However, this field of inquiry remains underexplored in sports and exercise medicine and sports physical therapy. Most intervention studies in sports and exercise medicine and sports physical therapy are terminated at the efficacy trial stage without considerations for best practices for translation to community and clinical settings. Lack of context-specific dissemination and implementation strategies to drive the translation of evidence-based interventions results in poor execution of, and attrition from, interventions, and this is associated with suboptimal outcomes and increased healthcare costs. Theory-driven quality research informing the successful dissemination and implementation of evidence-based interventions is needed to address lingering evidence-to-practice gaps. Dissemination and implementation research completes the final stage in the research-to-practice pipeline. It seeks to close evidence-to-practice gaps, thereby ensuring speedy application of research evidence to achieve desired public health outcomes while making more efficient use of limited resources. This review introduces sports and exercise medicine and sports physical therapy researchers and stakeholders to key concepts and principles in dissemination and implementation research.
- Knowledge translation
- Intervention effectiveness
- Implementation
- Behaviour
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Louis Pasteur had a foresight for dissemination and implementation (D&I) research and practice when he noted: ‘To him who devotes his life to science, nothing can give more happiness than increasing the number of discoveries, but his cup of joy is full when the results of his studies immediately find practical applications’. However, the application of scientific evidence in real-world practice is hard to come by. It is generally estimated that only about 14% of the best available scientific evidence for prevention and treatment becomes standard practice after an average of 17 years.1 Additionally, up to 40% of patients do not receive treatments with proven effectiveness2 and only one-third (34%) of research evidence informing guidelines is routinely adhered to.3 In a recent systematic review that used the Reach, Effectiveness, Adoption, Implementation and Maintenance (RE-AIM) Model to evaluate evidence-based injury prevention interventions across 74 studies in rugby union, the adoption, implementation and maintenance of interventions was below 20% for each dimension.4
Dissemination and implementation research is needed to improve the real-world translation of proven interventions into routine practice and policy. It completes the final stage in the research-to-practice pipeline.5 To understand the nuances of translating research evidence into practice in health, D&I science has come to the fore; however, to this point, it has gained scant attention in sports and exercise medicine and sports physical therapy (SEMS) research outlets. This is not to say that D&I work is not occurring; rather, little description of successful D&I efforts has been presented in the literature and research in this area is limited. For example, in a recent umbrella review of best evidence for mitigating injury risk among soccer players, no single systematic or narrative review was found regarding intervention implementation and evaluation despite numerous systematic reviews and meta-analyses for studies regarding risk/protective factors and intervention efficacy.6 Some of the challenges of capturing D&I in research can be addressed by clarifying core D&I concepts and principles to create a ‘common language’ for SEMS researchers and implementation partners and stakeholders, including policymakers, administrative leaders and practitioners in collaborative intervention efforts.
Interventions in SEMS, including therapeutic exercise for several musculoskeletal conditions, sports injury prevention and fall prevention exercise programmes, have been demonstrated to be efficacious and effective (when adherence to intervention is optimal) in high-quality studies, including systematic reviews and meta-analyses,7–17 and they have been recommended in many clinical guidelines.18–23 However, real-world implementation and outcome optimisation remain an ongoing challenge for most interventions.24–30 This is the result of researchers’ continued priority for discovery research and very limited focus on how to translate these discoveries into practice. Current evidence shows that D&I does not occur naturally and traditional methods of knowledge transfer (eg, publication of consensus statements and systematic reviews in scientific journals and presentations seminars) are passive and ineffective in moving scientific research into practice.31 Although proof of scientific evidence in well-controlled trials (efficacy/clinical trials) is an important first step towards the development and implementation of a potentially impactful interventions, this does not in any way guarantee translation into real-world clinical or community settings. Beyond answering the fundamental question regarding intervention efficacy—‘Does it work under near-perfect conditions?’—researchers also need to establish intervention implementation and real-world effectiveness, and do so in close collaboration with stakeholders in practice and policy spheres. Indeed, in order for evidence-based intervention (EBI) work to have greater public health impact, the SEMS field, as a whole, must work together to address the ‘real world’ in all aspects of the design, implementation, evaluation, application, and adaptation of interventions, as well as how intervention findings are shared with relevant audiences. Such questions would include: ‘Does it work in everyday real-world settings’, ‘Is it cost-effective’, ‘What drives successful implementation in specific contexts?’, ‘Is the overall goal achieved?’ and ‘Can an effective intervention be scaled up?’ Evaluating the implementation of EBIs in real-world contexts is imperative for identifying effective D&I strategies, and for developing new strategies for implementing change where they are needed. These strategies, in turn, are necessary to facilitate the adoption, proper execution and successful scaling of interventions into standard practice for meaningful public health impact.
The purpose of this review is to help SEMS researchers and stakeholders—including policymakers, administrative leaders, knowledge brokers, practitioners and individuals/patients—understand D&I concepts and principles that may speed-up the widespread integration of EBIs into usual practice and public policy. First, we describe D&I research and concepts, including an elaboration on adherence, the multilevel socioecological structure in D&I contexts and the determinants of implementation success. Next, we discuss D&I models and research designs. Finally, we discuss future directions for D&I research in SEMS.
DISSEMINATION AND IMPLEMENTATION RESEARCH: DEFINITIONS AND CONCEPTS
Dissemination is the active process of spreading EBIs to a target population through determined channels and using planned strategies.32 While dissemination alone will not bring about behaviour change in individuals, it is an imperative start towards evidence translation. Depending on context, health issue, level of effectiveness of the EBI, characteristics of the population, project goals and other factors, dissemination may precede or be preceded by implementation. The process of dissemination may be implied as an evidence-informed ‘branding and marketing’ of EBIs. While dissemination research may be taken as a part of the implementation continuum, it is an emerging field of enquiry often regarded separately from implementation research.32
In the earliest (2006) issue of the first journal dedicated to implementation research, Implementation Science, Eccles and Mittman defined implementation research as the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice, to improve the quality and effectiveness of health services.33 Implementation (the usual term in the United States) is often referred to as knowledge translation (in Australia, Canada and the United Kingdom). In this paper, we define an EBI as an activity that shows efficacy and/or effectiveness in the prevention, early detection or treatment of diseases and related health conditions. Evidence-based interventions may include programmes, policies, technologies, services or scientific information in the form of evidence synthesis (eg, systematic reviews, meta-analyses and clinical guidelines).32 The key concepts in D&I, along with other concepts discussed in this paper, are summarised in table 1 and described in greater detail in the following paragraphs.
Key concepts in dissemination and implementation research and practice
Additional fields of enquiry that have recently gained attention within D&I research are scale-up, maintenance (also referred to as sustainment), fidelity, adherence and adaptation research.39–41 44 51–53 Fidelity is defined as the extent to which an intervention is delivered (by a provider) as planned.40 Adherence is considered as a crucial element of fidelity, along with other elements including dose, quality of delivery, participant responsiveness and intervention differentiation.40 In long-term therapies, rehabilitation and preventive health, adherence is a more popular term, usually conceptualised as a socioecological and multidimensional implementation outcome that integrates most of the other elements of fidelity, for example, medication and exercise adherence.41 42 44 54 Other core concepts such as diffusion, mis-implementation and de-implementation, that may be aligned with implementation, have been described in the literature. Diffusion is defined as the ‘passive, untargeted, unplanned and uncontrolled spread of new interventions’, mis-implementation as the discontinuation of effective interventions and/or the continuation of ineffective ones and de-implementation as the ‘stopping or abandoning practices that have not proved to be effective and possibly harmful.32’
Adherence: a cornerstone for evidence-based intervention implementation
Adherence is defined as the extent to which an individual’s behaviour corresponds with agreed recommendations from a healthcare provider, an implementation practitioner or the EBI developer.41 42 Adherence is imperative for EBIs to be effective in real-world settings; however, it remains a challenge in drug- and exercise-based interventions, including home rehabilitation exercises, fall prevention interventions and neuromuscular training warm-up programmes for sport injury prevention.29 43 55 56 Lack of ‘optimal’ adherence (often operationalised as a finite threshold for intervention effectiveness), may cause a potentially useful EBI to be ineffective; in this case, a type III error bias is indicated.57 58 In such a situation, lack of intervention effectiveness is attributed to implementation failure.57
On the other hand, adaptation (or modification) is the process whereby changes are made to an EBI and/or its delivery method to better fit a given implementation context.39 45 Adaptation of EBI is a common practice in real-world settings and it is inevitable for complex interventions and system-wide implementation efforts.59 60 Adaptation can be treated as both an implementation outcome and an implementation strategy.39 Frameworks to guide and evaluate the adaptation process have been proposed.37 52 61 Ensuring that the core components of an EBI are executed in the face of adaptation and implementation barriers is imperative to maintain intervention effectiveness, and, relatedly, to ensure the integrity and intent of an EBI are sustained rather than ‘lost’ in adaptation.39 44
Adherence research in SEMS is still at developmental stages as it grapples with variations in definitions and lack of standardised measures. The 4-step Adherence Optimisation Framework proposed by Owoeye et al 44 provides guidance for improving adherence research in SEMS. The steps proposed in this framework may also be adapted to guide the development of implementation strategies for other implementation outcomes (eg, maintenance). Given that adherence is a key modifier of EBIs and health systems effectiveness, improving adherence behaviour is essential in addressing chronic health conditions effectively, including an upstream approach for the effective prevention of chronic conditions.
Implementation across socioecological levels
The practice of implementation occurs across multiple levels of change—usually individual, organisational and systems—within a socioecological structure, with identifiable actors within each level.35 36 Essentially, an actor or a group of actors (ie, the end-users of an EBI) need to do something differently for implementation to take place. In D&I research and practice, it is important to identify who (ie, the actor, usually the provider or practitioner, is expected to perform what (ie, the action), for the benefit of whom (ie, the target or recipient actors).35
Designing and evaluating the implementation of an EBI across multiple levels can be a daunting task. Although the outcomes of implementing an EBI are mostly manifested in individuals, actors often play diverse roles across an interactive multilevel eco-structure, in a vertical (ie, between levels) and/or horizontal (ie, within the same level) manner.35 62 63 For example, an EBI may be implemented in a socioecological structure encompassing a soccer athlete (a target actor at the individual level) who is a member of a team implementing an injury prevention programme delivered by a coach (a provider actor at the individual level) who reports to the club manager or president (a policymaker actor at the organisational level), who in turn reports to the board of directors or a national association (policymaker actors at the organisational/systems level). Another example is a patient (a target actor at the individual level) who receives treatment from a physical therapist (a provider actor at the individual level), who is supervised by a physical therapist manager or other managers/administrators (a policymaker actor at the organisational level—may also act as a team member), whose practice is regulated by a professional association and state/federal government (policymaker actors at the organisational/systems level). In the examples highlighted, the quality of interventions and corresponding outcomes for the injury prevention intervention in the soccer athlete and treatment intervention in the patient are impacted at all levels.
The contributions towards the successful implementation of an EBI would vary among actors and is contingent on the context of implementation. Active engagement of actors and stakeholders (by researchers) across the multiple socioecological levels of implementation—in what is referred to as community- (or practice-) based participatory research—through the stages of intervention development, testing and implementation planning is an essential aspect of D&I research.64 65 While community-based participatory research is not always possible or applicable in all D&I research contexts, this collaborative approach to knowledge generation and subsequent translation can substantially increase research relevance and greater buy-in for implementing EBIs.65
Embracing complexity: demystifying the multifactorial determinants of implementation success
In the science of implementation, behaviour change happens or does not happen depending on a convolution of contextual factors across a given eco-structure. These contextual factors are broadly classified as: individual/patient-related factors (eg, knowledge, beliefs, perceptions, motivations, outcome expectations, self-efficacy, behavioural intention, personality); team/group-related factors (eg, social norms, pressures and expectations, role modelling, collective efficacy, cohesion, diversity, composition); systems-related factors (eg, organisational culture and climate, leadership, resource capacity and the built environment, readiness, support for actors, external policies, communication, industry standards), socioeconomic and demographic factors (eg, socioeconomic status, educational status, marital status, race, social support, culture, sex, age); condition-related factors (risk proclivity, severity of disease/symptoms, level of disability, rate of progression, consequences of diseases, presence of comorbidities), EBI-related factors (eg, intervention duration, intervention complexity, evidence of efficacy/effectiveness, immediacy of beneficial effects, side effects) and policy factors (eg, policymaker knowledge and attitudes about the EBI, policymaker experience with the EBI, economic constraints, public opinion about EBI, interest/lobby group pressure).41 44 48 63 66–68 We conceptualise these contextual factors and any D&I strategies that may be applied to foster the delivery of an EBI as being intricately intertwined with one another (indicating potential interactions among variables) to determine behavioural outcomes in D&I actors (figure 1).
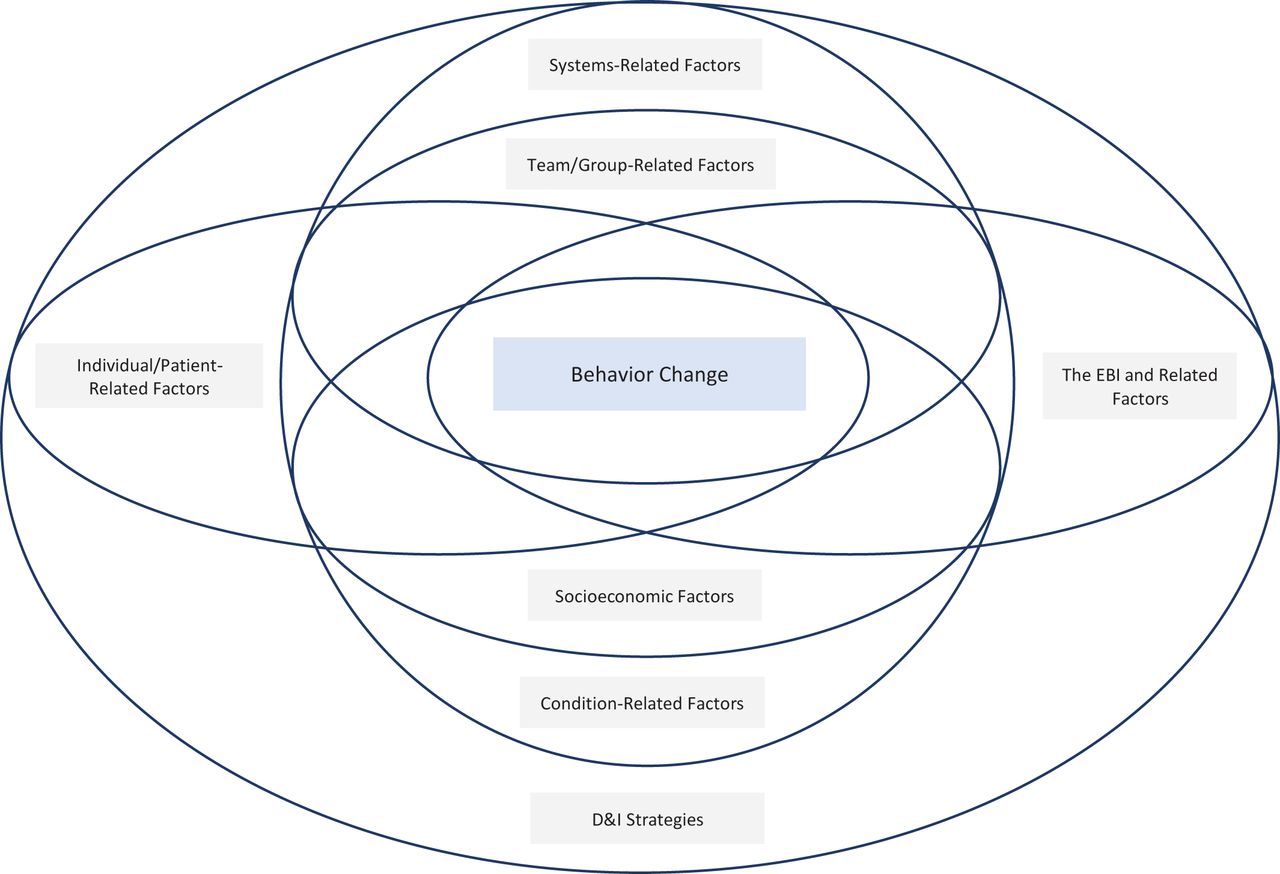
The complex interplay of the determinants of behaviour change. Behaviour change within a given socioecological level is dependent on a convolution of contextual factors. These factors, indicated as “factor rings,” potentially moderate one another and all factors relevant to the level of change influence behaviour change. EBI, evidence-based intervention; D&I, dissemination and implementation.
Some other terminologies have been used to refer to these factors, including ones such as individual characteristics, intervention characteristics, inner and outer settings.48 Contextual factors may also be evaluated as barriers or facilitators across levels or in specific actors.43 69 Often, in clinical and research settings, there is a tendency to solely focus on individual/patient-related factors, to the relative neglect of the other factors that may influence an individual’s capacity for change.41 An understanding of the complex interactions between all factors and their relative influence on individual actor behaviour, across levels—provider actors in particular—and within a given context, is essential for D&I success.
DISSEMINATION AND IMPLEMENTATION MODELS
Dissemination and implementation models (also sometimes described as frameworks) are a conceptual and organised combination of theories necessary to guide the planning and evaluation of EBIs and D&I strategies.38 46 Dissemination and implementation models are essential for understanding and improving D&I processes and outcomes; they help to align research questions with appropriate constructs in order to explain why an EBI or D&I strategy does or does not work.38 Moreover, studies framed within D&I models allow one to specify clear-cut objectives with theoretical underpinnings to provide a systematic approach to evaluating the D&I process across a spectrum of actors and diverse domains of determinants.
The most widely used D&I models are designed to address specific purposes such as: (1) guide the process of translating research evidence into practice (process models); (2) identify the factors that influence implementation outcomes (determinant models) and (3) provide a structure for evaluating D&I strategies (evaluation models).46 Some models integrate two or all of the aforementioned. In a review by Tabak et al,70 a total of 63 separate D&I models were identified at the time. As such, the formulation of new models has been discouraged.38 However, the need for adapting and/or combining models to comprehensively assess if an EBI is disseminated and implemented as intended is mostly always indicated in D&I studies.
Many of the D&I models currently available, especially those most popular in SEMS, for example, the RE-AIM and the Consolidated Framework for Implementation Research (CFIR), may guide an improved implementation of EBIs in SEMS.47–50 70–74 For example, the CFIR model aids in assessing multilevel factors that can affect and shape the implementation process itself, and thereby its effectiveness. Five primary domains are represented in CFIR (intervention characteristics, the organisation’s inner and outer settings, individual characteristics, and implementation process strategies), with each domain highlighting potential implementation barriers that may apply to particular contexts.48 Rather than focusing on implementation specifically, the RE-AIM model presents a framework for understanding the impact of interventions, suggesting this impact is a combined function of five related factors across levels: reach, or individual-level participation; effectiveness, or the individual-level outcomes of interventions; adoption, or the organisation-level representativeness of settings in which an EBI is implemented; implementation, or the organisation-level delivery of a programme as intended; and maintenance, or the routinisation and sustainment of behavioural change after the intervention in individuals and organisations.49 Thus, the RE-AIM model takes multiple levels of factors into consideration in highlighting the determinants of intervention impact. Both example models highlight the diverse roles D&I models can play in translation, implementation, and/or evaluation, and the abundance of influential and interactive factors and levels with bearing on D&I work. The challenge for researchers is how to select and adapt the most appropriate model(s) to fit the goal and context of a given D&I research project. That is, to be maximally effective, generative and evidence-based, D&I projects must be developed, described and evaluated with relevant implementation models that account for diverse and multilevel factors influencing change and intervention success in a given D&I context.
Here, we present an example of the adaptation of an existing implementation model, the Awareness-to-Adherence Model, to expand its utility in SEMS research. The Awareness-to-Adherence Model developed by Pathman et al 47 postulates that there is a sequence of cognitive and behavioural steps towards behaviour change. It posits that individuals (eg, clinicians, coaches) who are initially unaware of an EBI must first become aware of it (awareness), then intellectually agree with it (agreement), then decide it is appropriate and feasible to use in their own setting (adoption), and finally execute the EBI as expected (adherence). Further, it demonstrates that research evidence progressively ‘leaks out’ at each step of awareness, agreement, adoption and adherence.3 47 Thus, the progression to adherence may stop at any step for a variety of reasons. Although the Awareness-to-Adherence Model was originally tested in physicians to evaluate their implementation of a national clinical practice guidelines in the United States,47 it has been tested in several other clinicians/practitioners, countries and settings.3 75 76
The specific modifications made to the Awareness-to-Adherence Model for purposes of its introduction to SEMS include: (1) Inclusion of additional outcomes: adaptation, attrition and maintenance; (2) Expansion of the model to include a constellation of contextual factors that may influence the process of D&I (figure 2). Based on D&I literature, we conceptualise attrition and adaptation as co-existing variables alongside adherence29 39 77 and maintenance as the continued use of an EBI—an extension of adherence,37 38 78 for example, over 6 months.79 It is an expectation that adherence to an EBI will be counterbalanced by some levels of adaptation among actors39 and in alignment with the original model, further ‘leakage’ (here described as attrition) at the adherence level is also an expectation, preventing a progression to maintenance. Finally, we posit that several contextual factors (as previously described) determine how far actors at the individual and organisational levels progress through the model.41 44 48 63 66 67

{kind=link}
{kind=link}
Adapted Awareness-to-Adherence Model. An example typifying the adaptation of an existing implementation model (adapted with permission from Wolters Kluwer Health, Inc.: Pathman et al).47
The Adapted Awareness-to-Adherence Model typifies how an existing D&I model can be adapted to fit the objectives of a D&I study, which may include evaluating the implementation of an EBI, comparing implementation strategies or testing the contextual factors that influence the success of dissemination or implementation efforts. When applying the Adapted Awareness-to-Adherence Model or any other model to inform the D&I and evaluation of an EBI, researchers should carefully identify the socioecological level(s) of change applicable to the design of the EBI to be disseminated/implemented within a given setting.
DESIGNS FOR DISSEMINATION AND IMPLEMENTATION RESEARCH
Design and analysis in D&I research occur across different but overlapping phases of D&I, described as exploration, adoption/preparation, implementation and sustainment.80 Research designs would vary across these phases and would depend on the research question(s) asked. Similar to discovery research, traditional designs such as randomised controlled trials (RCTs), quasi-experimental and observational designs are frequently used in D&I studies.53 81 However, the focus in D&I studies is more on implementation outcomes (vs clinical outcomes) and context, and the exposures are D&I strategies (vs the EBIs implemented). Additionally, pragmatic cluster RCTs, as in the case of real-world intervention effectiveness trials (vs near-perfect efficacy trials), are often favoured in D&I studies.82 While still ensuring a careful concealment of allocation of participants during randomisation, pragmatic RCTs provide a realistic compromise between internal and external validity of a study to better reflect what is obtainable in real-world settings.83 Alternative research designs to RCTs, ones that allow researchers more flexibility while maximising external validity, are also used in D&I studies, although less frequently.81 Common examples of alternative designs include: roll-out (randomised) design (also referred to as stepped-wedge design), in which units/sites/clusters are randomly assigned to different start times (ie, randomisation by time) for EBI and/or types of implementation strategies53 and interrupted time series, a quasi-experimental design in which data are collected at multiple and evenly spaced time points (eg, weekly, monthly, every 6 month) before and after implementing an EBI.84 85
Depending on the stage of development of the intervention and how much of scientific evidence is available, pragmatic studies may focus on both clinical (eg, reduction in pain, injury) and implementation outcomes (eg, adoption, adherence) in a hybrid effectiveness-implementation design.86 Hybrid designs foster the movement of interventions towards implementation. Three categories of the hybrid design are possible in randomised and non-randomised trials.53 The degree to which the focus of a trial is skewed towards evaluating the effectiveness and/or implementation of an EBI determines its design in the hybrid spectrum (table 2).
Types and characteristics of hybrid designs
CONCLUDING REMARKS AND FUTURE DIRECTIONS
This review provides a primer for SEMS researchers and stakeholders interested in D&I research. Given that many SEMS interventions have been demonstrated as EBIs through traditional RCTs, systematic reviews, meta-analyses and umbrella reviews, there is a need for comprehensive D&I research efforts to accelerate translation of these interventions into practice in real-world settings. Sports and exercise medicine and sports physical therapy researchers need to acquire an appreciable level of proficiency in D&I research towards improving D&I practices for the adoption, adherence or fidelity, appropriate adaptation, delivery, scale-up and sustainment of EBIs in SEMS, for the greatest public health impact possible. Researchers, in collaboration with and informed by other SEMS stakeholders, should be interested in understanding the core questions related to knowledge translation in diverse settings: ‘What makes an intervention work in the real-world?’, ‘Where do D&I actors mostly fall off the path to adherence and maintenance/sustainment?’, ‘What contextual factors influence the progression of D&I actors across the cognitive and behavioural steps that lead to change (eg, a clinician implementing an evidence-based clinical guideline or a coach implementing a proven neuromuscular training warm-up injury prevention programme)?’. They should consider using established but relevant theory-based D&I models to evaluate the contextual factors that influence the implementation process in relation to specific outcomes and across levels of change, using both quantitative and qualitative methods, and a multidisciplinary approach. Although a broad range of contextual factors has been suggested in this review, researchers will need to make an informed decision regarding the factors that are most pertinent to their study, and to the practical settings in which their intervention will be (and, in the future, could be) implemented and scaled-up. These factors may also be integrated into other models of interest.
There is an urgent need for D&I research in SEMS in order to ‘level up’ translational D&I research with discovery research. In many areas of SEMS research, sport injury prevention, for instance, there is a need to move beyond RCTs evaluating intervention efficacy to RCTs evaluating (new) implementation strategies—and, then, testing these strategies where they are needed. For example, conducting more efficacy RCTs for the 11+ and other proven neuromuscular training warm-up injury prevention programmes would be a misplaced research priority; instead, a Type 2 or Type 3 implementation-effectiveness hybrid design would be a valuable addition to the knowledge base towards improving their translation to routine practice and public policy. The Expert Recommendations for Implementing Change Project93 provides a detailed list of a broad range of potentially effective D&I strategies from which researchers can select, contingent on the empirical evidence specific to the implementation context of their project, for the purpose of preliminary implementation and evaluation of EBIs or to test the effectiveness of such strategies. Additionally, researchers with knowledge of system dynamics modelling may apply basic to complex modelling techniques in their D&I projects, from causal loop diagrams to agent-based modelling, to engage implementation actors and stakeholders in collaborative D&I research and practice. Finally, we have included in this review, a set of selected resources to provide additional instructions regarding D&I research (box 1).
Box 1 Useful resources for dissemination and implementation research
Choosing/combining/adapting D&I models
One-stop resource for implementation researchers
Implementation science webinars, blog, sample D&I grants
D&I toolkits
Summary box
What is already known
Several interventions in sports and exercise medicine and sports physical therapy have been tested and proven in high-quality studies and reviews, and they have been recommended in many practice guidelines; however, real-world implementation and outcome optimisation remain an ongoing challenge.
Dissemination and implementation research is critical for understanding and applying evidence-based interventions in different health contexts, but underexplored in sports and exercise medicine and sports physical therapy.
Evidence-based interventions must be complemented by evidence-informed, cost-effective and context-specific dissemination and implementation strategies for policymakers, administrative leaders, knowledge brokers and practitioners to effectively apply and sustain the best research evidence in public health and clinical practice.
What are the new findings
This review introduces sports and exercise medicine and sports physical therapy researchers and stakeholders to key concepts and principles in dissemination and implementation research; creating a ‘common language’ for use in evidence-based intervention partnerships.
This review presents an adaptation and expansion of an existing implementation model that incorporates the factors (eg, policy, socioeconomic, systems-related, individual/patient-related factors) that impacts implementation success and behaviour change sustainment, and across multiple socioecological levels in specific implementation contexts.
Theory-driven real-world translational research is needed to complement the ever-increasing discovery research in sports and exercise medicine and sports physical therapy .
REFERENCES
Footnotes
Twitter Oluwatoyosi Owoeye @owoeye_oba.
Acknowledgements This review was completed during the COVID-19 pandemic lock-down and work-from-home period. The lead author wishes to acknowledge the support received from his wife, Adeola Owoeye and kids, Dami and Demi Owoeye through the completion of this work.
Contributors OBAO conceived and designed the study, wrote the first draft of the manuscript and conducted the literature review for study content. RSR and RCB contributed to the design, and provided additional literature relevant to study. All authors contributed to the critical revision of manuscript drafts and approved the final version.
Funding This research work was funded by the Saint Louis University, St. Louis, MO, United States.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.