Article Text

Abstract
Objective The purpose of this scoping review is to determine if and how sex and gender have been incorporated into low back pain (LBP) clinical practice guidelines (CPG), and if sex and gender terms have been used properly.
Methods CPGs were searched on MEDLINE, Embase, NICE, TRIP and PEDro from 2010 to 2020. The inclusion criteria were English language, CGPs within physiotherapy scope of practice and for adult population with LBP of any type or duration. Three pairs of independent reviewers screened titles, abstracts and full texts. Guidelines were searched for sex/gender-related terms and recommendations were extracted. The AGREE II (Appraisal of Guidelines for Research and Evaluation II) was used to evaluate the quality of the CPGs.
Results Thirty-six CPGs were included, of which 15 were test-positive for sex or gender terms. Only 33% (n=5) of CPGs incorporated sex or gender into diagnostic or management recommendations. Sixty percent of guidelines (n=9) only referenced sex or gender in relation to epidemiology, risk factors or prognostic data, and made no specific recommendations. Overall, there was no observable relationship between guideline quality and likeliness of integrating sex or gender terms. The majority of guidelines used sex and gender terms interchangeably, and no guidelines defined sex or gender.
Conclusion CPGs did not consistently consider sex and gender differences in assessment, diagnosis or treatment of LBP. When it was considered, sex and gender terms were used interchangeably, and considerations were primarily regarding pregnancy. Researchers should consider the importance of including sex-based and/or gender-based recommendations into future LBP CPGs.
- back injuries
- gender
- lumbar spine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known?
Back pain is one of the most common conditions seen by family doctors and physiotherapists.
Low back pain is highly prevalent with up to 80% of people experiencing at least one back pain episode in their lifetime.
There are known sex and gender differences in the epidemiology, diagnosis and treatment of low back pain.
What are the new findings?
Clinical practice guidelines (CPGs) do not consistently consider sex and gender differences in the assessment, diagnosis or treatment of low back pain.
When sex or gender terms are considered, the terms are used interchangeably without regard to their strict definitions.
When CPGs did consider sex or gender, the considerations primarily related to pregnancy, which is a subterm of sex, as it does not refer to sex but rather a transient period that is specific to one sex.
Introduction
Low back pain (LBP) is defined as pain located in the area between the posterior lower margins of the 12th ribs and the gluteal folds, and may occur with associated lower limb pain/neurological involvement.1 2 LBP can be classified as acute (less than 6 weeks), subacute (6 to 12 weeks) or chronic (greater than 12 weeks).2 The origin of LBP is multifactorial, and is divided into non-specific LBP (NSLBP), specific, and serious pathologies.3 According to the 2017 Global Burden of Diseases, Injuries and Risk Factors Study, LBP was ranked number one for years lived with disability in 1990, 2007 and 2017, with increasing rates of occurrence for all ages.4
LBP research indicates significant differences between genders regarding prevalence, degree of disability and number of comorbidities; which are all higher in individuals who identify as women.5 Despite known differences, research studies that focus on LBP inconsistently report or fail to integrate sex or gender differences into their design, analysis and conclusions,6 and it is common to observe sex and gender terms used interchangeably. This practice can not only lead to misinterpretation of results, but also impact how evidence is applied.
In 2009, the Government of Canada made changes to the Health Portfolio in order to acknowledge the differing needs of men and women in relation to health, and defined sex and gender as independent descriptors.7 Sex was defined as a set of biological attributes in humans and animals that is most often associated with physical and physiological features of an individual (ie, reproductive/sexual anatomy).7 Sex was categorised as female or male, accounting that there are many variations in the biological attributes that are sex, and how the attributes may be expressed.7 Gender was referred to as the socially constructed role, behaviour, expression or identity of an individual (ie, girls, boys, women, men, gender diverse) and influences how people perceive themselves and others.7 Gender is often seen as binary (girl/woman and boy/man) but there is great diversity in how individuals experience and express gender.7 The 2016 Sex and Gender Equity in Research (SAGER) guidelines were designed for both authors and peer reviewers, with the intention of standardising sex and gender reporting in research.8 In 2017 Tannenbaum et al6 examined how sex and gender were integrated into Canadian clinical practice guidelines (CPGs) for non-communicable disease. Tannenbaum et al6 found that only 35% of guidelines made sex or gender specific recommendations, and only 25% of the studies used sex and gender terms correctly.6 Currently there are no reviews that specifically examine sex and gender considerations in LBP CPGs.
Objectives
The primary objective of this scoping review was to systematically examine if and how sex and gender was incorporated into LBP CPGs for adult populations, as it related to diagnosis, epidemiology, prognosis, risk factors and interventions. The secondary objective was to determine how sex and gender concepts have been used. The final objective was to determine if sex and gender representation was considered in the development of the guideline committee. A scoping review approach, which aims to provide a broad overview of a topic in order to identify key concepts and gaps in the literature, was deemed most appropriate due to the lack of known research on the topic of sex and gender in relation to LBP.9
Methods
The methodological framework for conducting scoping reviews, that was established by Arksey and O’Malley,10 and enhanced by Levac and colleagues,11 was used. The first five steps were followed, however, the sixth and final step, consulting with key stakeholders, was not performed, as a result of time constraints.11 This scoping review also followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension for reporting guidelines for scoping reviews.12 The protocol for this scoping review was registered with OSF prior to title and abstract screening, in order to maintain transparency and reduce bias13 (10.17605/OSF.IO/7S9BD).
Inclusion criteria
All CPGs issued by a multinational committee, within the scope of physiotherapy (PT), with an adult population (18 years or older) focusing on primary LBP, were eligible for inclusion. LBP conditions that primarily related to cancer, fracture, infection, inflammatory diseases or other serious pathologies were excluded. All durations of LBP were eligible for inclusion. The methods were based off of the protocol by Oliveira et al,14 but due to the high volume of guidelines, and recognising that sex and gender were unlikely to be considered prior to 2009, the inclusion criteria was adjusted after registration.13 After full-text screen, a limit of the past 10 years was applied and only the most recent version of a CPG was included, unless different topics were addressed. Only guidelines that were published in English were eligible.
Outcomes
The primary outcome was how sex and gender had been incorporated into healthcare recommendations within CPGs. Recommendations pertaining to diagnosis, epidemiology, prognosis, risk factors and interventions were considered. The secondary outcome addressed whether or not sex and gender concepts had been used as per the definitions that were previously outlined by the Government of Canada.7 Additionally, we examined whether diversity of sex and gender were considered in the development of the guideline research committee.
Search strategy
A search for CPGs was conducted on MEDLINE via Ovid (1946 to March 8 2020), Embase (1974 to March 9 2020), National Institute for Health and Clinical Excellence (NICE) (1999 to March 9 2020), Turning Research into Practice Medical Database (TRIP) (1997 to March 17 2020) and Physiotherapy Evidence Database (PEDro) (1999 to March 9 2020). There were no date limits applied. The following key terms were used in the search: low back pain and clinical practice guideline. A McMaster University (Ontario, Canada) Health Sciences Librarian was consulted to refine the search strategy. A comprehensive outline of the search strategy and the specific terms that were used can be found in online supplemental appendix A. This study excluded grey literature due to resource constraints. A manual search for CPGs included in the reference lists of the included studies was performed.
Supplemental material
All eligible studies were imported to Covidence15 for removal of duplicates and screening. A pilot screen was completed by all reviewers for the first 10 titles/abstracts and full texts to ensure consistency. Three pairs of investigators (TR and HH, TC and MK and SR and CT) independently screened titles/abstracts and full texts. Any disagreements were discussed between the pair of reviewers, and if a consensus was not reached, a third-party investigator (LM) was consulted.
Data extraction and analysis
The same calibration process, using the first three studies, was performed for data extraction procedures. Data extraction and quality assessment was completed by the same pair of reviewers that were previously referenced. Any discrepancies were handled in the same way that was previously mentioned.
Based on the methodology of Tannenbaum et al,6 the included CPGs were first screened electronically for keywords: sex, gender, women, men, woman, man, boy, girl and pregnan*. A guideline was categorised as text-positive if it included any keywords in the main text. In this review, pregnancy was considered to be a subterm related to sex, recognising that it is a transient period of time in a female’s life, rather than a sex-specific term.
Text-positive guidelines were grouped into four categories based on how sex and gender differences were incorporated into the guidelines. Category 1 was recommended evidence-based sex-related or gender-related diagnostic approach,6 Category 2 referred to a sex-related or gender-related management approach,6 Category 3 ‘made reference to sex or gender within epidemiological data, risk factors or prognostic data, but did not make suggestions for diagnosis or clinical management’,6 and Category 4 ‘mentioned sex or gender keywords superficially’.6 In this review, the term superficial was used to describe the use of sex or gender terms without additional context or consideration as it relates to the literature or guideline recommendations. Further analysis considered the correct use of ‘sex’ and ‘gender’ terms, as defined by the Government of Canada.7 If the correct use could not be determined, guidelines were rated as ‘unclear’. Lastly, investigators examined whether the authors considered sex and gender representation in the development of each guideline committee.
Methodological quality assessment
The Appraisal of Guidelines for Research and Evaluation II (AGREE II)16 tool was used to assess the quality of the CPGs.16 A calibration of the first three CPG’s was completed prior to completing the quality assessment in pairs. A threshold of 60% was used to evaluate the overall quality for the final score of each domain of the AGREE II.16 17 When ≥5 domains had a score of greater than 60%, the guideline was defined as high quality.17 When three or four of the domains had a score of greater than 60% and when less than or equal to two domains scored greater than 60%, the guidelines were defined as average quality and low quality, respectively.17 The total score of each guideline and the domains were calculated. The median scores were used to examine any superficial relationships between the quality of the guideline and the likeliness of integrating sex or gender terms.
Results
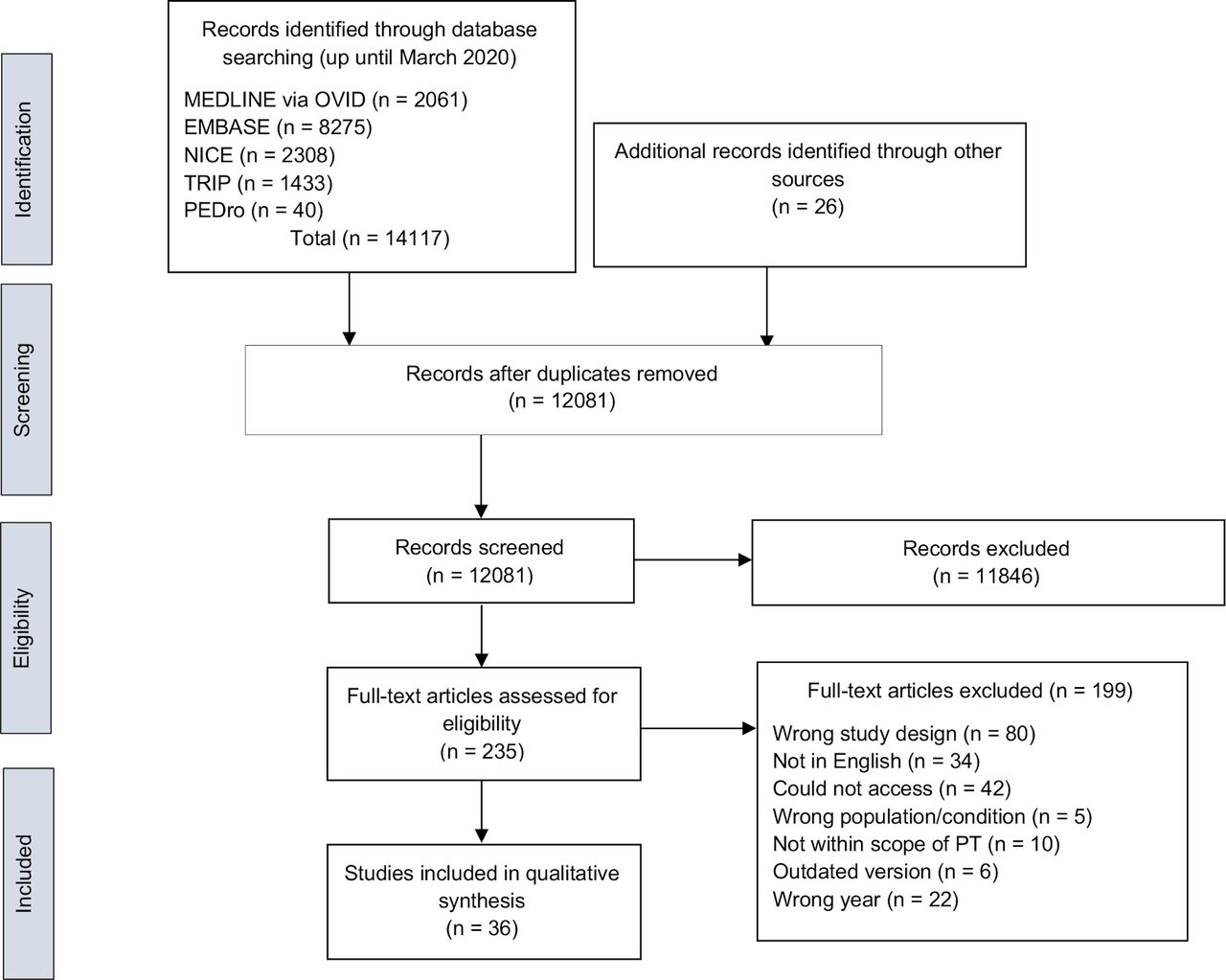
The electronic searches conducted from 2010 to March 2020 identified 14 117 studies (see figure 1 for PRISMA flow diagram). We identified 235 CPGs, from which, 199 were excluded. Reasons for exclusion included: being published before 2010 (n=22), wrong study design (n=80), not accessible in English (n=34), wrong patient population (n=5), not within the scope of physiotherapy (n=10), outdated version of CPG (n=6) or inaccessible (n=42) (online supplemental appendix B). Thirty-six CPGs were included in the review.18–53
Supplemental material
{kind=link}
PRISMA flow diagram
Study characteristics
Most of the guidelines were from the USA (31%),23 26–30 38 39 43 45 48 Canada (11%)19 20 49 52 and North America (8%).25 34 35 The majority of CPGs (42%) made recommendations in relation to a combination of NSLBP and specific LBP,18–20 23 24 29 33 37 39 43 47 48 50–52 or NSLBP (39%) alone.21 22 25 27 28 30 36 42 44–46 49 53 Four CPGs (11%) focussed on specific LBP,26 32 34 35 two (5%) focussed on LBP prevention40 41 and one CPG (3%) focussed on a combination of NSLBP, specific LBP and pathological LBP.31
The majority of the guidelines (53%) made reference to all durations of LBP.18 19 21 22 24 25 27 29–31 33 38 39 42 43 49–51 53 Five CPGs (14%) made recommendations based on a combination of acute, subacute or chronic LBP,20 45 47 48 52 four (11%) referred strictly to chronic,26 28 37 44 two (5%) were in relation to acute LBP23 46 and the remaining six CPGs (17%) did not specify duration.32 34–36 40 41 There were two CPGs that focussed on diagnosis,30 39 nine focussed on management19 24 28 32 43 44 47 52 53 and four CPGs focussed on prevention.21 36 40 41 The majority of the CPGs provided information on both diagnosis and management of LBP.18 20 22 23 25–27 29 31 33–35 37 38 42 45 46 48–51
Inclusion of sex/gender terms
There were n=15 (42%) text-positive CPGs for sex and gender terms18 20 23 27 29 30 37 38 41 42 44 46 48 49 53 and n=21 (58%) text-negative CPGs19 21 22 24–26 28 31–36 39 40 43 45 47 50–52 when pregnancy-related terms were included. Table 1 depicts the categories for text-positive guidelines, and the AGREE II16 score for each text-positive and text-negative guideline. Category 1 and/or Category 2 guidelines which related to diagnosis and management, respectively, made up 33% of the text-positive guidelines. There were two CPGs that were identified as both Category 1 and Category 2,23 48 and three guidelines that were identified as only Category 2.44 53 Nine CPGs were identified as Category 3 (60%)20 27 29 30 37 38 41 42 46 making reference to sex or gender terms in relation to epidemiology, prognosis or risk factors. There was only one Category 4 guideline, which superficially mentioned sex or gender terms49 without providing further context.
Sex and gender text-positive clinical practice guidelines and text-negative clinical practice guidelines with the corresponding AGREE II score
When pregnancy-related terms were excluded from the results, the lack of sex and gender integration was more pronounced (online supplemental appendix C). No guidelines made reference to sex or gender considerations in relation to LBP diagnosis, and only one guideline considered gender differences in management.23 Eight guidelines made reference to sex or gender terms in relation to epidemiology, prognosis or risk factors.20 27 29 30 37 41 42 46 These results further depict the lack of sex or gender considerations beyond pregnancy.
Supplemental material
Sex/gender keywords
Examples of paraphrased quotes retrieved from all of the text-positive CPGs were depicted in table 2. The quotes were organised by their respective categories (1 to 4), based off of the methodology by Tannenbaum et al.6 Within Category 1 there were two guidelines that provided recommendations for contraindications against imaging techniques for pregnancy.23 48 One of the guidelines gave an additional Category 1 recommendation with regards to clinical examination.48 For example, flexion and extension movements were contraindicated during clinical exams of patients who were pregnant.48 Within Category 2, there were five studies that gave specific management recommendations in regard to pregnancy considerations.18 23 44 48 53 Pregnancy-specific recommendations included rehabilitation strategies, contraindications to electrotherapy, precautions to acupuncture and precautions or contraindications for certain medications.18 23 44 48 53 There was only one guideline within Category 2 that provided a management recommendation that was not specific to pregnancy.23 The recommendation made reference to avoiding trunk extension/flexion exercises in women at risk for osteoporosis.23 The majority of the Category 1 and Category 2 recommendations were for specific considerations in pregnancy.
Summary of the use of sex and gender terms in relation to the respective category
Category 3 CPGs were most prevalent (n=9) and integrated sex and gender terms most frequently.20 27 29 30 37 38 41 42 46 Category 3 CPGs integrated sex or gender terms into epidemiology, risk factors and care-seeking behaviours.20 27 29 30 37 38 41 42 46 CPGs reported that women tend to have a higher prevalence of LBP and are more likely to seek care for LBP20 27 37 42 One pregnancy-specific reference was made within Category 3, stating that two-thirds of pregnant women experience LBP.38 Category 3 was the only category that referenced male sex or gender, stating that men, more often than women, experience LBP as a result of manual material handling.41 Men also have a higher risk of developing ankylosing spondylitis and spondylolysis.29 30 46 The only CPG that was considered Category 4, referenced pregnancy within the exclusion criteria.49
Appropriateness of sex/gender use
None of the identified text-positive CPGs provided a definition of sex or gender within the guideline,18 20 23 27 30 37 38 41 42 44 46 48 49 53 and only three CPGs30 42 46 had appropriate use of the terms according to the Government of Canada.7 Two CPGs did not contain enough information to determine if the terms were used properly.27 41 The remaining 10 CPGs had inappropriate use of sex and gender terms, for example, using gender terms when relating to biological attributes.18 20 23 29 37 38 44 48 49 53 Only one CPG considered sex and gender representation in the formation of the guideline committee.39
Methodological quality assessment
The total score for each domain of the AGREE II16 as well as the final overall quality was determined for each guideline (online supplemental appendix D). Of the 36 evaluated guidelines, 418 19 28 51 were high quality (11%), 1225 30 33 36 38 39 42–44 46–48 were average quality (33%) and 2019 21–24 26 27 29 31 32 34 35 37 40 41 45 49 50 52 53 were low quality (56%). Only two guidelines20 51 reached an acceptable (≥60%) score in all six AGREE II16 domains. The remaining CPGs had at least one domain with a low score (<60%). Of all domains, Domain 4 (‘Clarity of Presentation’) had the highest mean quality score 79% and Domain 5 (‘Applicability’) had the lowest mean quality score 22%. The overall median AGREE II16 score of all CPGs, as well as text-positive CPGs, was 4 with an IQR of 1. There was no observable relationship between the quality of the guideline and likeliness of integrating sex or gender terms. There were five guidelines22 29 30 37 47 for which the referenced methodology or appendices were not in English, thus the scores may not be a true representation of their methodological quality.16
Supplemental material
Discussion
Major findings
Overall, the CPGs identified in this scoping review had poor integration of sex and gender considerations, and the majority of CPGs did not mention sex or gender terms. When sex or gender terms were mentioned, they were primarily in relation to epidemiology, risk factors or prognostic data. There were few CPGs that integrated any sex or gender differences into their recommendations regarding diagnosis or treatment of LBP. The majority of the time, recommendations were for specific considerations in pregnancy.18 23 44 48 53 The majority of guidelines used inappropriate terms when referring to either sex or gender. Often, sex and gender terms were used interchangeably, and there was very limited separation between the use of the biological sex terms and social gender terms. Only one guideline committee acknowledged if diversity of sex and gender was considered in the development of the committee.39 No CPG provided a definition of sex or gender within the guideline.
The findings of this review had both consistencies and inconsistencies to a similar study conducted by Tannenbaum et al.6 Tannenbaum et al6 found that 67% of the included CPGs were text-positive for sex or gender terms. Thirty-five per cent of text-positive CPGs fell under Category 1 and Category 2 recommendations (reported screening, diagnosis or management considerations specific to sex or gender), and the majority of CPGs (41%) made reference to sex or gender considerations in epidemiological or risk factors. It is clear that this scoping review had a much lower text-positive response than Tannenbaum et al,6 with only 42% of CPGs being text-positive. The inconstancies found between the number of text-positive guidelines may be due to differences in study methodology. Tannenbaum et al6 only included Canadian studies, whereas this review was expanded to international guidelines. Research funders in Canada, such as the Canadian Institute of Health Research (CIHR), are a driving force behind sex and gender integration in Canadian research.54 Canadian guidelines may be more likely to integrate sex and gender considerations into research, compared with other countries, as a result of the CIHR.
Tannenbaum et al6 excluded studies that had key words specific to pregnancy, whereas this review included pregnancy as a sex term in order to be more inclusive. The majority of Category 1 and Category 2 recommendations in this review were related to pregnancy. When pregnancy terms were omitted, there were no guidelines that made reference to diagnosis, and only one guideline that referred to management. Sex and gender considerations need to go beyond pregnancy, teratogenicity or breastfeeding, and consider more complex interactions such as specific and non-specific LBP. Future studies should integrate sex and gender terms in relation to all age milestones, rather than solely focussing on transient periods, such us pregnancy. This approach to sex and gender integration would make recommendations applicable to a broader population.
Strengths and limitations
This scoping review used rigorous methodology to ensure low risk of bias and quality of reporting. The methodological framework for scoping reviews by Arksey and O’Malley,10 and Levac et al11 was used. The PRISMA guidelines for reporting were also followed.12 The study protocol was registered with OSF prior to title and abstract screening to ensure transparency of the process and reduce potential bias.13 A comprehensive search strategy was used, which was developed in partnership with a librarian. In addition, the AGREE II16 was used to evaluate the quality of the included CPGs.16
Restricting the language to English only was a limitation of this review. This review only considered CPGs and excluded primary literature. It is possible that our results do not represent the current state of sex-based and gender-based primary research pertaining to LBP. Another limitation was limiting the inclusion criteria to the past 10 years. Earlier CPGs that integrated sex and gender terms may have been excluded by this narrow timeline. A 10-year cut-off was chosen because government bodies and experts began recognising the importance of sex and gender considerations in the literature after 2009.8 54 We recognised that these changes would take a year or more to integrate into research, therefore, before 2010, it was unlikely that CPGs integrated sex or gender terms.
Conclusion
This review provided insight on the current use of sex and gender terms in CPGs related to LBP. Integration of sex and gender considerations has the potential to guide future clinical practice and research, specifically regarding differences in the diagnosis, prognosis and management of LBP. This review is intended to be eye-opening for LBP researchers regarding the fact that sex and gender are not being integrated in current CPGs. The use of guides, such as the SAGER guidelines, should become a priority in the future.8 This review highlights that there are known sex and gender differences in management, epidemiology, risk factors and care-seeking behaviours in LBP, which should be considered during physiotherapy practice. Future research should consider examining both the inclusion and appropriateness of the use of a larger spectrum of gender specific terms (ie, non-binary), as current knowledge on this area of gender integration and research regarding LBP is limited. Clinicians should educate themselves on the differences between sex/gender and be cautious when using LBP recommendations from current CPGs.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @gazzimacedo
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors All authors contributed to the study conception and design. Study design, data collection and analysis were performed by all authors. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.