Article Text

Abstract
Objectives Exercise programmes studied after stroke often involve specialist supervision. Determine the feasibility and safety for people with stroke (PwS) or transient ischaemic attack (TIA) participating in readily accessible, non-stroke specialised, community-based exercise programmes.
Methods Participants were recruited into a structured, group-based, 12-week programme of aerobic and resistance exercise delivered two times per week at one of five local leisure centres. Completion rates, successful attainment of intended exercise intensity (Borg Rating of Perceived Exertion (RPE)) and safety outcomes were recorded. Measures of physical activity (International Physical Activity Questionnaire), health-related quality of life (EQ-5D) and blood pressure (BP) were recorded at baseline and day 1 post intervention.
Results 79% of participants completed >75% of the intended sessions, with >90% attainment of intended RPE. Exercise was safe with no serious and very few minor adverse events related to exercise. Exercise led to significant increases in EQ-5D (Best of Health p<0.001), levels of weekly moderate physical activity (p<0.001) and decreases in systolic BP (mean change [95% CI]=−5.4 mmHg [−2.84 to −7.96]; p<0.001).
Conclusion Generalised exercise programmes delivered through existing local services, appears feasible, safe and may improve quality of life, physical activity and systolic BP, for PwS and TIA.
- Exercise rehabilitation
- Community
- Cardiovascular
- Feasibility
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Stroke is a leading cause of adult-onset disability.1 Aerobic and resistance exercise confers a variety of health benefits to people with stroke (PwS) or transient ischaemic attack (TIA), including reduced blood pressure (BP),2 improved walking speed,3 balance4 and functional capacity.5
Despite this, there is a paucity of stroke-specific exercise programmes and geographical heterogeneity in access to standardised pathways for exercise referral following stroke, particularly in the UK.6 The existing literature includes studies that have all incorporated supervision by stroke-specific therapists,7 8 but understanding whether less supervised programmes of exercise are safe and effective may extend these interventional benefit to a greater number of PwS. As such, our objective was to establish whether PwS and TIA can feasibly and safely derive overall benefit from widely available exercise programmes delivered by non-stroke specifically trained exercise instructors.
METHODS
Multi-site, single-arm, pilot study carried out at Sheffield Teaching Hospitals and five local leisure centres from March 2015 to January 2017. Approval for the study was obtained from the Yorkshire and Humber ethics committee (REC ref 16/YH/0317) and patients consented to participation.
Participants and eligibility criteria
PwS or TIA within the last 12 months and who could sit independently and understand verbal instruction were recruited from the stroke and TIA services at the Sheffield, UK, after providing informed consent. Patients were excluded if their language or cognitive function precluded participation or they had contraindications to exercise according to the American College of Sports Medicine Guidelines For Exercise Testing and Prescription (online supplemental material).9
Supplemental material
Intervention protocol
The programme consisted of 60 min group (4–8 per group) sessions, two times per week for 12 weeks based on activities from phase IV cardiac rehabilitation.7 Sessions were led by a trained exercise instructor (Level 3 or 4 trained, online supplemental material). Exercise intensity was prescribed according to the Borg Rating of Perceived Exertion (RPE),10 with target exertion ranging 11–13 (light intensity) for the first few sessions, increasing to 14–16 (moderate intensity) as the programme progressed. Participants were asked to report their RPE during the circuit training section of the exercise session. Neither cardiopulmonary exercise testing nor heart rate monitoring was used to guide exercise prescription as this is not routinely available at most leisure centres across the UK. Intervention details according to the Consensus for Exercise Reporting Template (CERT)11 are included in the online supplemental material.
Outcome measures
Demographic (age, sex, ethnicity) and clinical information (index event, National Institute of Health Stroke Score (NIHSS), Functional Ambulation Category (FAC)12 were collected at baseline.
Feasibility
Intervention feasibility was assumed if >75% of sessions were attended and completed by at least 75% of participants (electronic patient registration on entry to facility) and participants achieved target RPE at >75% of sessions.
Safety
Intervention safety was defined as the absence of any serious adverse events, as detailed by the National Research Ethics Service,13 with <10% participants experiencing any adverse events (AEs). During exercise sessions, instructors tracked symptoms of dyspnoea, chest pain and lightheadedness, as well as enquiring about physician visits relating to exercise.
Health-related quality of life (HRQoL)
The EQ-5D is a self-reported measure assessing five domains: mobility, ability to carry out self-care, ability to perform usual activities, pain/discomfort and anxiety/depression. It is valid, reliable and responsive in stroke patients.14 15 The overall EQ-5D is scored between 5 and 25 with lower scores representing higher HRQoL, and contains a ‘Best of Health’ visual analogue scale between 0 and 100; here, a higher score represents better perceived health.
Physical activity
Levels of physical activity and sedentary behaviour were measured using the International Physical Activity Questionnaire,16 which quantifies time (minutes) spent performing vigorous physical activity, moderate physical activity, walking and sitting in the previous 7 days.
Physiological parameters
Systolic and diastolic BPs (mmHg) and heart rate were measured (Omron M7 Intelli, non-affected arm) while participants sat at rest for 5 min. Participant height (cm) and weight (kg) were measured and body mass index (BMI, Kg/m2) calculated.
Data analysis
Data are summarised and statistically anaylsed according to whether it was normally (mean, SD, two-tailed paired t-test) or non-normally (mean, IQR, Wilcoxon signed-rank) distributed. A p value of <0.05 was taken as being statistically significant. Data analysis was performed using IBM SPSS for Windows v25.
RESULTS
Recruitment
A total of 234 PwS and TIA were screened, 140 were eligible and 61 participants consented and enrolled. Six participants (9.8%) deferred entry but completed the programme, while 7 (11.5%) participants dropped out of the study with incomplete follow-up (figure 1).

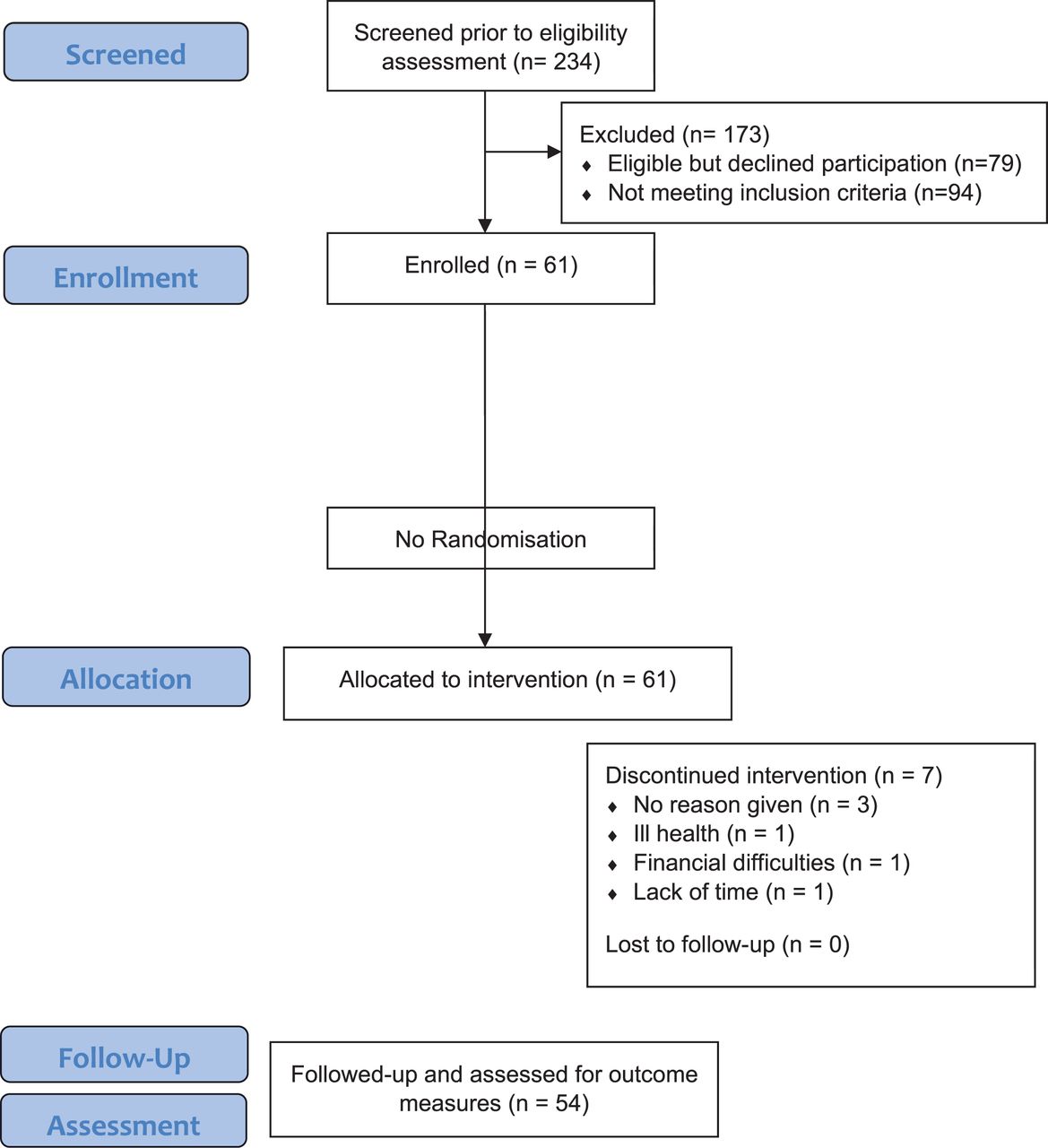{kind=link}
Study flow diagram.
Baseline characteristics
Nearly two-thirds of participants (63%) were male and 48 (88%) Caucasian (table 1). Age ranged between 27 and 90 years with a mean (SD) of 64.5 (5.6) years. Mean (SD) initial NIHSS score of the stroke cohort was 4.2 (3.8), although this ranged from 3 to 16 indicating those with more severe stroke were also included in the programme.
Baseline characteristics of participants completing intervention (n=54, unless otherwise specified)
Feasibility
Overall, 48 participants (78.7%) completed more than 75% of the intended sessions (inclusive of six deferred participants), and target RPE was achieved during 95.2% of exercise sessions. Overall, 54 (88%) of participants progressed from low-intensity to moderate-intensity activity by Week 2.
Safety
One patient sustained a fall during an exercise session with no major injury. One individual dropped out of the study due to poor health unrelated to their stroke. No other AEs related to exercise were reported, there were no physician attendances due to the programme.
Health-related quality of life (HRQoL)
Median (IQR) EQ-5D score was 8 (6–11) at baseline and 8 (6–10) at 12 weeks, indicating no significant change (table 2). For the EQ-5D mobility domain, scores increased significantly at 12 weeks (Z=−2.65, p=0.008), as did median (IQR) EQ-5D visual analogue score (55 (50–70) vs 65 (55–80), Z=−5.73, p<0.001).
Impact of exercise intervention on health-related quality of life and physical activity (n=54)
Physical activity
Time spent undertaking vigorous physical activity did not change significantly post intervention (table 2), although three participants did report at least 45 min of weekly vigorous activity that they did not do at baseline. Median (IQR) time spent during moderate physical activity increased significantly from baseline to post intervention (0 (0–60) vs 60 (0–120), Z=−4.10, p<0.001) as did time spent walking (Z=−3.57, p<0.001), while time spent sitting reduced (540 (382.5–675) vs 480 (360–660), Z=−4.03, p<0.001).
Physiological parameters
Median (IQR) weight was 91.5 (78.9–98.0) kg at baseline and reduced to 89.5 (77.8–97.6) kg at 12 weeks (Z=−3.29, p=0.001, table 3). This was not associated with a significant difference in BMI postintervention (p=0.194). Mean (SD) systolic BP (SBP) reduced significantly post exercise by 5.4 mmHg (95% CI 2.84 to 7.96 mmHg). There were no significant differences in diastolic BP (p=0.2) or resting heart rate (p=0.429) at 12 weeks.
Impact of exercise intervention on physiological parameters (n=54)
DISCUSSION
A 12-week mixed aerobic and resistance exercise programme, delivered through local facilities in the absence of stroke specialist supervision, appears feasible and safe for PwS and TIA. Furthermore, this programme was associated with statistically significant improvements in HRQoL, weight and SBP. The minimal clinically important difference for EQ-5D visual analogue scores stroke patients undergoing rehabilitation is approximately 10 points,17 indicating the changes seen with the programme are clinically meaningful. While the relationship between weight loss and stroke risk is unclear, that between SBP and stroke risk is very clear.18 Antihypertensive therapy can reduce the risk of secondary stroke by up to 24% when compared to placebo,19 and meta-analyses of randomised-controlled trials of such therapy for secondary stroke prevention indicate average SBP reduction of around −5.1 mmHg,20 not dissimilar to the reductions seen in this cohort following exercise (−5.4 mmHg). However, as this study did not have a control group, we are unable to establish whether such meaningful improvements in HRQoL and SBP would not have happened as part of the natural course of recovery following stroke and TIA.
Relationship with previous research
There is a strong evidence base for the beneficial effects of exercise on cardiovascular risk after stroke.21 However, individual barriers to exercise after stroke include fear of falls, physical disability, fatigue, post-stroke depression and pain and uncertainty about how to exercise appropriately.22 23 System-level barriers include access to appropriate facilities, supervision expertise, transportation availability and costs.22 Previous studies have confirmed that patients with minor stroke and TIA can successfully be incorporated into cardiac rehabilitation programmes,21 24 however access to such programmes for PwS and TIA is lacking. In contrast to this, conventional exercise facilities (including gymnasiums and leisure centres), aimed for the general population, are widely present in most areas. Group-based exercise sessions at these existing services may provide an opportunity for PwS and TIA to engage in regular exercise in a setting that is more accessible and at a lower cost than clinician-supervised exercise programmes. The findings of this study should allay fears regarding safety of less specialised supervision, at least in those with mainly mild and moderately severe stroke undertaking light- and moderate-intensity activity. The completion rate (79%) of the exercise programme further emphasises the positive level of engagement of PwS in alternative, community-based exercise interventions.
Limitations
Firstly, no control group existed which could have delineated the effects of the exercise intervention against spontaneous improvements. Nevertheless, most participants were more than 6 months poststroke or TIA and may have reached a plateau in their physical rehabilitation. Second, while intervention completion rates were high, and achievement of RPE targets were >90%, we do not know how well the intervention was tolerated. In particular, no measure of fatigue was recorded to qualify this. Third, we did not record a comprehensive list of outcome measures during the study as such may have overlooked other benefits of exercise for example, on mood, however, those chosen reflected measures easy to undertake that were not time-consuming and were important to help drive changes in clinical practice. Fourth, we acknowledge that these results may not generalise to people with more severe stroke.
Conclusions
PwS and TIA successfully engage in a 12-week community-based structured exercise programme, delivered through local facilities, in the absence of stroke specialist supervision. This was safe and associated with beneficial signals in SBP and HRQoL. A definitive randomised-controlled study is now warranted to determine if such an intervention is effective at improving recovery and HRQoL following stroke and TIA.
What are the new findings
Exercise programmes delivered in community leisure centres by non-stroke specialist exercise professionals are feasible and safe for people with stroke (PwS) and transient ischaemic attack (TIA).
Such programmes may be associated with meaningful improvements in systolic blood pressure, physical activity levels and health-related quality of life.
This may be an important way to extend the benefits of exercise-based rehabilitation to PwS and TIA in the UK.
REFERENCES
Footnotes
Contributors AA planned and designed the study and supervised all aspects of the study including recruitment, follow-up, data collection and analysis and manuscript writing. SB performed data collection and analysis and all authors contributed to the manuscript writing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval NHS ethical approval for the study was obtained (REC ref 16/YH/0317) and patients consented to participation.
Provenance and peer review Not commissioned; externally peer-reviewed.
Data availability statement The data that support the findings of this study are available on request from the corresponding author (AA). The data are not publicly available due to restrictions on information that could compromise the privacy of research participants.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.