Article Text

Abstract
Introduction The burden of breast cancer in Canada is steadily growing. More women are surviving breast cancer, yet, survivors live with side effects for years after treatments have ended. The benefits of exercise for women with breast cancer are well established and include improvement in treatment-related physical and emotional side effects. Despite these benefits, few survivors meet exercise guidelines. Exercise programmes are needed within the cancer institution in Canada to bridge the current knowledge to practice gap. The purpose of this study is to test the effects of a novel implementation strategy that includes institution-based exercise plus self-management (SM) or SM alone versus usual care in improving exercise level, quality of life, aerobic capacity, muscle strength and use of healthcare services over 12 months for women with breast cancer receiving chemotherapy.
Methods and analysis Participants: Women with stages I–III breast cancer undergoing chemotherapy. Intervention: Group 1: institution-based exercise and SM (8 exercise sessions plus 8 SM modules); Group 2: SM alone; Group 3: usual care. Outcomes: The primary effectiveness outcome is minutes per week of moderate to vigorous physical activity. Secondary outcomes include quality of life, aerobic capacity, muscle strength, and use of healthcare services. Randomisation: Participants will be randomised (1:1:1) to one of the three groups by a blinded statistician and will be stratified based on age of participant (<40, 40–60, and >60 years). Statistical analysis: Outcomes will be measured at baseline, post-intervention, 6-month and 12-month follow-up using an analysis of covariance to test changes between groups over time adjusted for age.
Ethics and Dissemination This study addresses a long-standing need to help women with breast cancer undergoing chemotherapy become and stay more active by implementing novel rehabilitation strategies into real-world practice. This is vital in order for this population to minimise the lingering side effects of treatment, improve function and quality of life and prevent cancer recurrence.
Trial registration number The study protocol (v1: July 2020) has been registered on ClinicalTrials.gov (NCT04109274).
- Exercise
- Physical activity
- Physiotherapy
- Oncology
- Rehabilitation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
One in two Canadian women are expected to be diagnosed with cancer in their lifetime.1 The most common cancer diagnosis in Canadian women is breast cancer (25.5% of female cancer diagnoses).1 With improved screening and new treatment approaches more women are also surviving cancer; the 5-year survival rate for breast cancer is 87%.1 Common cancer treatments, such as chemotherapy, lead to side effects during treatment such as nausea, peripheral neuropathy and cancer-related fatigue.2 Survivors also live with treatment-related side effects, including fatigue, pain, loss of strength and anxiety, for years after their treatments have ended.1 3 4
Regular exercise is one health behaviour that has shown beneficial effect for women with breast cancer.5–9 Exercise during10–12 and after treatment13–16 leads to improvements in treatment-related side effects.16–19 In addition, observational research demonstrates the potential for regular exercise to decrease breast cancer recurrence20 21 and all-cause and cancer-specific mortality.20–22
Few breast cancer survivors self-report regular exercise participation.23–25 During chemotherapy treatment, it has been found that more than 77% of breast cancer survivors do not engage in any exercise.26 This lack of exercise has the potential to cause further impairment deficits and declines in functional capacity on top of common chemotherapy side effects. A large proportion of breast cancer survivors are not aware of the benefits of exercise during or after treatment.23 Treatment side effects, time and travel to exercise services also pose barriers to exercise participation.23 Furthermore, healthcare professionals working in oncology describe several barriers to exercise promotion at the institutional, personal and patient level such as time, exercise knowledge and patient side effects.27 Novel, evidence-based accessible opportunities that focus on feasible exercise interventions for all women are needed.28
Providing accessible opportunities for exercise is important as the incidence of cancer in Canadian women is projected to increase by 74% in the next 10–15 years, primarily due to population growth and an ageing population.29 Inactivity contributes to physical and psychological side effects, risk of cancer recurrence, and an increase in comorbid conditions. There is a knowledge gap regarding optimal exercise implementation strategies since there are very few studies on real-world effectiveness.30 Additionally, research on the cost-effectiveness of exercise strategies for this population and the examination of exercise implementation outcomes is scarce.
This study builds on a pilot randomized control trial (RCT) previously conducted using similar methodology and intervention at the Juravinski Cancer Centre (JCC). Results from 26 women with stages I to III breast cancer undergoing adjuvant chemotherapy found the intervention to be feasible and showed preliminary effectiveness of the intervention on physical activity levels, perception of health status and exercise knowledge.31 32 We plan to build upon our previously conducted pilot RCT with a fully powered RCT that includes improvements to the intervention and methods to determine the effectiveness of this intervention for breast cancer survivors in the short and long term. Specific updates to the methods and intervention include the addition of a second intervention group, and the inclusion of booster sessions, additional outcome measures and longer follow-up timepoints. The overall findings of this project have the potential to improve the way exercise and rehabilitation services are provided within institutions delivering care for patients with cancer.
METHODS AND ANALYSIS
Research objectives
Research objective 1
To determine the effectiveness of a novel implementation strategy for an exercise and self-management (SM) programme for women with stages I to III breast cancer undergoing adjuvant or neoadjuvant chemotherapy.
Primary Question: What is the effectiveness of institution-based exercise plus SM or SM alone versus usual care in improving exercise level for women with breast cancer receiving chemotherapy?
Secondary Questions: (1) What is the effectiveness of institution-based exercise plus SM or SM alone versus usual care in improving quality of life, exercise intention, health status, aerobic capacity, muscle strength and patient engagement over 12 months for women with breast cancer receiving chemotherapy? (2) What is the cost-effectiveness of this implementation strategy for an exercise and SM programme for women with stages I to III breast cancer undergoing adjuvant or neoadjuvant chemotherapy?
Research Objective 2
To explore the barriers to exercise adherence for women with breast cancer during adjuvant or neoadjuvant chemotherapy.
Study design
This is a pragmatic trial. A hybrid type 133 effectiveness-implementation RCT will be used to address Research Objective 1. Reporting will be in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines for pragmatic trials34 (see figure 1, CONSORT diagram). A qualitative descriptive study using semi-structured interviews will be used to address Research Objective 2. The Hamilton Integrated Research Ethics Board has approved this study (Project ID# 7673). The study protocol has been registered on ClinicalTrials.gov (study identified: NCT04109274). All participants will provide written informed consent on the approved consent forms prior to study enrolment.
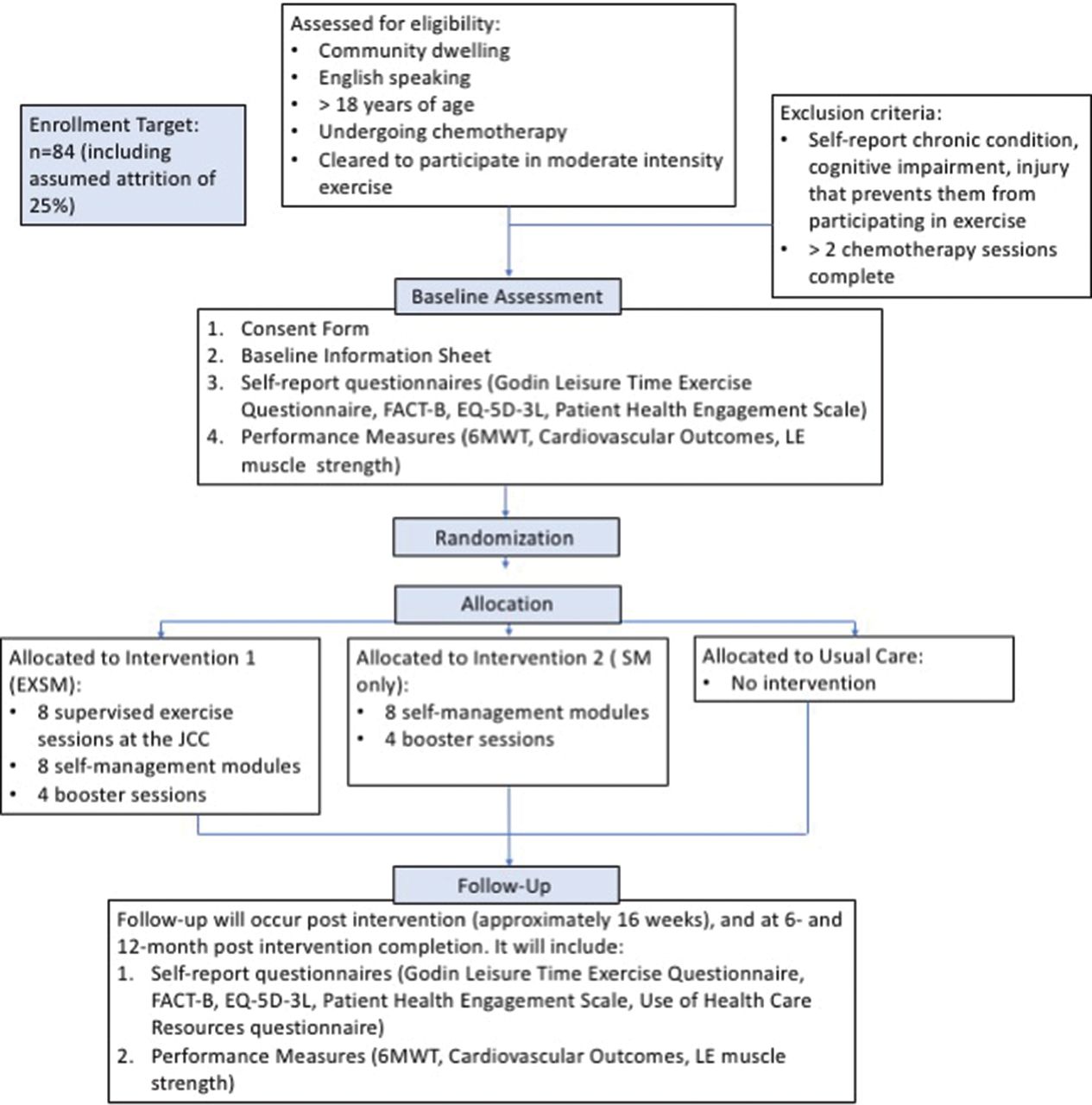
CONSORT diagram.
Sample
Inclusion/exclusion criteria
Eligible participants include: (1) community-dwelling, (2) English-speaking women, (3) over 18 years of age, (4) who are currently undergoing adjuvant or neoadjuvant chemotherapy for stages I–III breast cancer at the JCC and (5) are cleared by their oncologist to participate in moderate-intensity aerobic exercise. Participants will be excluded if they self-report on the patient intake form any chronic condition, cognitive impairment or injury that prevents them from participating independently in moderate-intensity aerobic exercise, and if they have already completed >2 chemotherapy sessions.
Sample size
Power analysis for an ANOVA test with three groups was conducted in G*Power35 to determine sample size. An alpha of 0.05 adjusted using the Bonferroni method for multiple primary comparisons, power of 0.95, and medium effect size (0.5; assumed to be the same for both comparisons) for the primary outcome of physical activity level,36 37 measured by the Godin Leisure-Time Exercise Questionnaire, was used. Based on these assumptions, the desired sample size is 66 participants. With an expected dropout rate of 25%, based on completion of the pilot study 6-month outcome data, the total sample size for this study is 83 participants (rounded to 84; 28 per group).
Recruitment
Recruitment for this study will occur in three ways: (1) medical oncologists will identify possible participants within their patient caseload. The oncologist will obtain consent from the patient for the research coordinator to contact them directly; (2) referral sheets will be put in new patient charts by hospital administration for patients who meet the inclusion criteria. Oncologists will see these referral sheets at the treatment planning appointment; (3) the research coordinator will recruit patients at the cancer centres ‘chemotherapy education class’. Potential participants will be contacted by phone to discuss eligibility and potential study enrolment.
Setting
The JCC in Hamilton, Ontario, Canada will be the site of participant recruitment and will be where the institution-based portion of the intervention occurs.
Intervention
Research objective 1
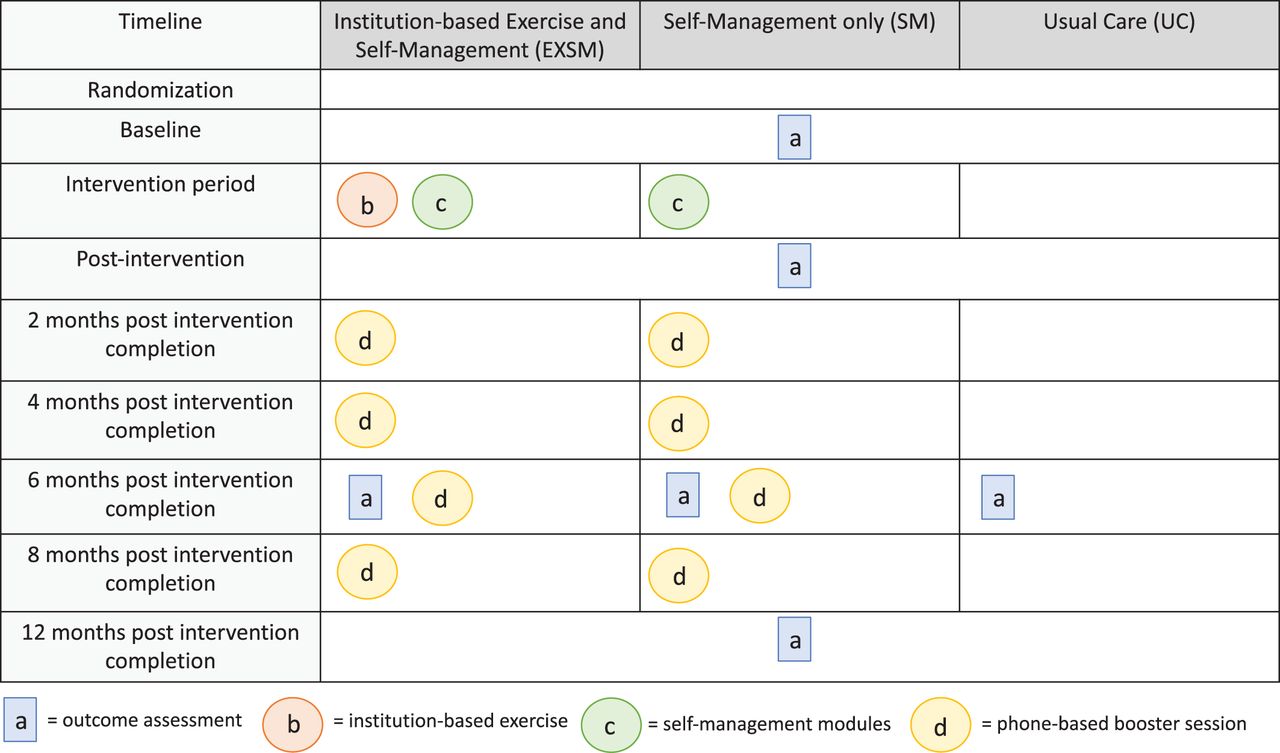
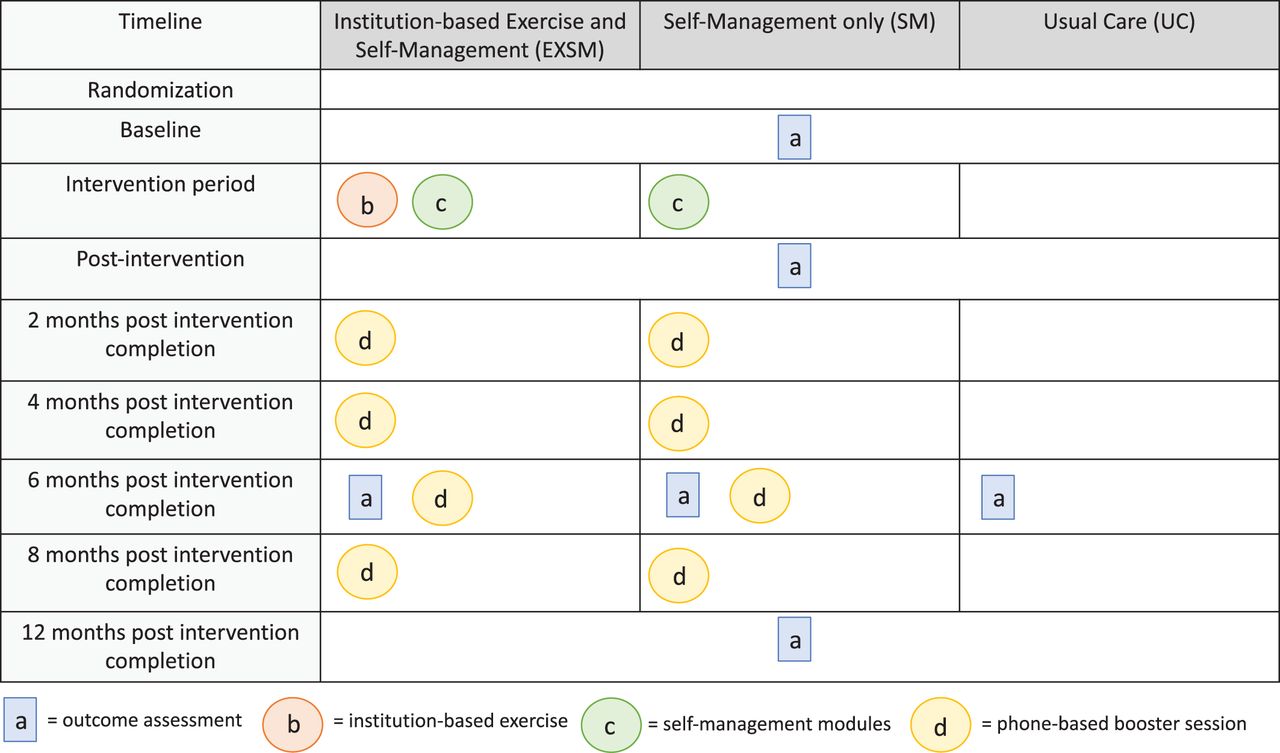
Participants will be randomised (1:1:1) to one of the three groups by a blinded statistician and will be stratified based on age of participant (<40, 40–60 and >60 years). Allocation of participant randomisation will be concealed using a computer software program by a blinded statistician. The three groups will include: (1) institution-based exercise and SM, (2) SM only, and (3) usual care. Participants in all groups will be provided with a Fitbit Inspire to wear for the duration of the project and will be able to keep the Fitbit after the study is complete. Refer to figure 2 for a study timeline based on group allocation.
{kind=link}
{kind=link}
Study timeline.
Institution-based exercise and self-management (EXSM)
Participants randomised to the EXSM group will take part in eight sessions of supervised exercise within the cancer institution concurrent with eight SM modules focusing on goal setting and action planning for safe and effective exercise strategies. Four booster sessions will be provided to this group at 2, 4, 6 and 8 months post-intervention completion.
The exercise component will include aerobic exercise using recumbent bikes. The intervention will be delivered within the cancer institution when the participant is already coming in for another appointment. Participants will perform up to 30 min of moderate-intensity exercise (4–6 out of 10 on Rate of Perceived Exertion scale or 50–70% HRmax based on physical activity guidelines for individuals with cancer)7 8 for eight sessions during chemotherapy. An exercise professional trained in providing exercise support for individuals with cancer will conduct the exercise component. The SM component will include eight previously created and piloted SM modules31 delivered to participants on an iPad prior to or after the exercise component. The goal of these modules is to help participants develop physical activity goals and action plans to continue with between sessions, with an overarching goal of helping them reach exercise guidelines for cancer survivors7 8 and the Canadian Physical Activity Guidelines.38 The most recent guidelines published for cancer survivors in 2019 recommend moderate-intensity aerobic training for at least 30 min, three times per week and resistance training for all major muscle groups at least two times per week using sets of 8–15 repetitions at 60% of an individual’s 1RM.8 During the COVID-19 pandemic, the EXSM group is on hold until it is safe to resume in person sessions.
Four booster sessions will be provided to participants in this group. An assessor trained in behavioural counselling will provide booster sessions by phone and will discuss the individuals physical and emotional condition, current level of exercise, accomplishment of previously set goals and action plans and perceived barriers to participation in exercise. The assessor will use facilitation strategies to aid participants in devising strategies to overcome barriers and set realistic goals and action plans.
Self-management only (SM)
Eight SM sessions for safe and effective exercise strategies will be provided to this group as well as four booster sessions (as described above).
SM modules will be viewed by participants in this group when they are coming into the cancer centre for another appointment. However, during the COVID-19 pandemic, participants in this group will be given the option to have these modules delivered virtually using zoom media and/or email and phone. An exercise specialist will aid in the administration of each session module and answer participants questions as needed.
Usual care (UC)
Participants in this group will receive care as normally provided by their treating oncologist. This can be heterogeneous between different physicians and centres, but usually has a similar goal and includes oncologists encouraging patients to ‘stay active’ during treatment.27
Research objective 2
Participants in the EXSM and SM only groups with an intervention adherence rate of less than 75% will be asked to complete an interview to determine the barriers to intervention adherence. Semi-structured interviews will be conducted with these participants by a researcher trained in qualitative methods. Interviews will be recorded and transcribed.
Data collection and management
All outcome data will be collected in person at four different time points (baseline, post-intervention, 6-month and 12-month post-intervention completion). At baseline, participants will complete the baseline information form and consent in addition to completing the self-report and performance-based outcomes (six-minute walk test, cardiovascular outcomes, lower-extremity strength testing) with a blinded assessor. At the follow-up time points, participants will fill out the described self-report questionnaires and be assessed by a blinded assessor on performance outcomes. Outcome data will be given by the assessor to the research coordinator who will manage the data in a secure data management software. During the COVID-19 pandemic, participants who are scheduled for a follow-up assessment will be given the option to have the self-report outcome measures sent by email to complete and send back to study investigators by email. In person outcomes will not be conducted until it is safe to resume the study.
Outcomes
Primary outcome
Physical activity level will be the primary outcome for this study. This outcome will be assessed using a Fitbit Inspire. All participants will be asked to wear the activity tracker during waking hours for the duration of the study. They will be asked to track the number of steps recorded by the device each day and to bring a printout of their daily activity totals to each assessment time. Physical activity level will also be assessed using the Godin Leisure-Time Exercise Questionnaire.39 This self-report measure gives weekly frequencies of strenuous, moderate, and mild activities and a total weekly leisure activity score and is reliable and valid to classify respondents into ‘active’ and ‘insufficiently active’ categories.39–42
Secondary outcomes
Quality of life will be measured using the FACT-B,43 a self-report measure designed to assess multi-dimensional QOL specifically for women with breast cancer. This measure is valid and reliable when used to assess the quality of life in women with breast cancer.43
Exercise intention will be assessed using a Theory of Planned Behaviour (TPB) based questionnaire. This questionnaire assesses each construct of the TPB (attitude, subjective norm, perceived behaviour control, intention) to understand an individual’s intention to change behaviour. The TPB has been used broadly to determine levels of intention and behaviour for various health behaviours, including exercise.43 44 The TPB is supported for use with individuals with cancer.45 46
Health status will be measured using the EQ-5D-3L.47 This scale has two components: a descriptive scale assessing problems with five dimensions of health (mobility, self-care, usual activities, pain/discomfort and anxiety/depression) and a visual analogue scale recording respondent self-rated health on a scale of 0–10 (0 worst health state, 10 best health state).47 The EQ-5D is a valid and reliable tool in assessing health status in individuals with cancer.48 The EQ-5D will also be used as part of the economic analysis to determine quality-adjusted life years.
Functional capacity will be measured using the 6-minute walk test (6MWT),49 a submaximal exercise test that assesses total distance walked in 6 min. This test has been found to be a valid and reliable tool to assess sub-maximal aerobic capacity in adults >18 years and with various chronic conditions.50 51 Age-based norms are available by sex.
Lower-extremity strength will be measured using a manual muscle dynamometer. Movements assessed will be isometric hip and knee flexion/extension and ankle plantarflexion/dorsiflexion. Lower-extremity strength is a predictor of all-cause mortality52 and physical functioning.53 Refer to table 1 for a description of how dynamometry will be performed for each movement.
Manual muscle testing dynamometer methods for assessing lower-extremity strength
Patient engagement will be measured using the Patient Health Engagement Scale.54 This scale assesses five domains related to the experiences and preferences of patients for their engagement with their healthcare treatment.54 It is valid and reliable in adults with chronic conditions.54
Cardiovascular outcomes to be measured include resting blood pressure (RBP) and heart rate (RHR). As common chemotherapy drugs are known to increase the risk of cardiomyopathy, these measures will assess changes in basic cardiac function across the study (at various time points and during chemotherapy infusion). RBP and RHR will be measured at all intervention times by a blinded assessor as well as at each intervention session by the exercise professional for the EXSM group.
Adverse events resulting due to this intervention will be reported and documented in each participants exercise logs. These logs are updated by trainers at each intervention session for both the EXSM and SM only groups. Adverse outcomes may include any orthopaedic injury or pain, cardiac event or trip or fall that occurs during or after the intervention that the participant relates to the provided intervention.
Implementation outcomes
The implementation strategies are designed to increase the reach of the programme beyond what has been described in the literature to date. Therefore, outcome assessment will be guided by the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) framework.55 This framework has been used to guide the planning and evaluation of health-related interventions from efficacy to implementation interventions.56–58 RE-AIM will be used to inform this interventions delivery and evaluation to long-term impact and ongoing legacy of this initiative. See table 2 for a definition of each RE-AIM framework item and measures to be used to determine implementation effectiveness.
RE-AIM framework and associated measures
Economic evaluation
The economic evaluation will occur in three main ways. First, the costs to run the two intervention groups (EXSM and SM) will be calculated and compared in total value. Second, the use of healthcare resources will be compared between all three groups (EXSM, SM and UC) at each follow-up time. This will be assessed using a piloted self-report outcome measure assessing healthcare facility visits (walk-in clinic, urgent care use), doctor visits (family doctor, specialist appointments), procedures obtained (ultrasound, X-ray, etc.) and support services used (registered nurse, physiotherapist, social worker, etc.). All costs will be determined based on the current Ontario healthcare standards and will be presented in Canadian dollars. Finally, the EQ-5D-3 L will be used to compare quality-adjusted life years of participants in the intervention arms and the control group. This outcome has been used extensively to perform cost-utility analyses for individuals with chronic conditions.59 60
Analysis
The analysis and reporting of this trial will follow the CONSORT guideline.34 Participant characteristics will be analysed at baseline to ensure no significant differences exist between groups. Mean and SD and one-way ANOVA tests will be used to assess differences between the three groups for continuous variables. Frequencies and the Kruskal–Wallis H test will be used to assess differences between groups for categorical variables. Multiple imputation will be used to handle missing data. All results will be reported as estimate of difference (95% CI) and associated p-value. The overall level of significance will be set at alpha=0.05 adjusted using the Bonferroni method for multiple primary comparisons. There will be no adjustment of alpha for secondary outcomes—their analyses are exploratory. All analyses will be performed using STATA/MP14.
Research objective 1
An analysis of covariance will be used to determine within and between group differences for the effectiveness outcomes between the three groups. Covariates will include age, stage of disease and socioeconomic status (SES). An intention to treat analysis will be used for these analyses by imputing last observation carried forward. A subgroup analysis will occur for Research Objective 1 to determine if intervention effectiveness is affected by (1) age and (2) SES. The effect of SES is important to analyse as it has been found that individuals with lower SES have lower accessibility to cancer services and higher cancer-related incidence and mortality rates.61 For this analysis, participants will be divided into groups based on their SES (household income < CA$40 000 (low income), CA$40 000–125 000 (middle income) or > CA$125 000 (high income).62) Refer to table 3 for a summary of analysis methods for Research Objective 1. All subgroup analyses will be performed by adding the interaction effect between the subgroup-variable and the intervention variable. The criterion for statistical significance will be set at alpha=0.05, and this will not be adjusted for multiple testing since these analyses are exploratory. RE-AIM measures will be analysed using descriptive statistics. Attendance rates will be determined based on the % of total intervention sessions attended.
Method of analysis for primary and secondary outcomes of research objective 1
Research objective 2
Interview transcripts will be analysed using qualitative content analysis and inductive coding. The first five transcripts will be coded independently using line-by-line analysis by two researchers. The researchers will meet to discuss emerging themes and develop a coding scheme for subsequent analysis. The remaining transcripts will then be independently coded as they are completed. All transcripts will be uploaded to NVivo12 (qualitative analysis software) and the coded data will be aggregated into nodes and grouped into meaningful categories based on the patterns that arise from the data.
Patient and public involvement
Individuals with breast cancer were involved in the design of the exercise intervention for this study. A focus group was held to discuss exercise needs of breast cancer survivors and strategies to increase exercise availability within the cancer institution in 2015. The intervention methodology for the pilot trial and this trial was based on these findings.28
DISCUSSION
Findings of this trial have the potential to improve the way rehabilitation services are provided within cancer institutions. Results can be used to guide future programming and allocation of funds related to supportive care services for women with breast cancer in this geographical location. Rehabilitation programmes should be accessible for all cancer survivors. The unique implementation characteristics to increase accessibility employed in this trial include that sessions are scheduled when participants are already coming into the cancer centre for another appointment and that the programme is free for all eligible survivors. The use of goal setting and action planning for exercise self-efficacy are important intervention components to facilitate behavioural change.63 64 The updates made in this study’s methodology from the pilot trial, including the addition of a SM only group, will help determine the active ingredients of the intervention; what additional effect does exercise have over SM alone? The inclusion of SM education, including goal setting and action planning, is vital to provide women with the knowledge and confidence to independently maintain healthy lifestyle behaviours on a daily basis over the long term.63 Furthermore, SM strategies have been suggested to lead to beneficial effects on quality of life for women with breast cancer.63 64 Currently, whether SM alone is enough to promote the uptake of exercise recommendations among cancer patients is unknown. Since preliminary estimates of effect from the pilot trial demonstrated significant between group differences at the post-intervention assessment time-point (and not at 2-month and 4-month follow-up) booster sessions were included in this intervention for both the EXSM and SM only group. The inclusion of booster sessions to behavioural interventions is suggested as a way to maintain treatment effects.65 66 Booster sessions are follow-up sessions conducted after the initial intervention to encourage the continuation of a behaviour.66 They often include components of goal setting, action planning and facilitation strategies to overcome barriers and are effective to maintain exercise levels in individuals with various chronic conditions.66 Additional outcomes were also added to this study to get a more holistic view of the effects of the intervention on function, and 6-month and 12-month follow-up assessment time points were implemented in order to see if the intervention facilitates sustained behaviour change.
Debate currently exists regarding the optimal way and location to deliver this type of programme.67 This novel implementation strategy incorporates both institution-based and home-based exercise strategies within regular practice during chemotherapy and highlights the need for women with breast cancer to take an active role in self-managing this condition early on in the course of their disease in order to prevent future treatment-related complications. Results of this study will help to inform future decision making about the optimal implementation strategy regardless of a survivor’s socioeconomic status. The findings of this study will inform stakeholders as to whether the proposed translational strategy can be effectively introduced into a clinical setting. This study addresses a long-standing need to help women become and stay more active by implementing novel rehabilitation strategies into real-world practice. We hope the results of this study will help to determine the best ways to make exercise a standard of care for all women with breast cancer.
REFERENCES
Footnotes
Contribution All authors have been involved in the development of the study protocol. JST drafted this manuscript and all other authors reviewed, provided feedback and approved the manuscript for submission.
Funding This work is supported by the Juravinski Hospital and Cancer Centre Foundation (grant number T210).
Competing interests None declared.
Ethics approval The Hamilton Integrated Research Ethics Board has approved this study (Project ID# 7673). Results of this project are planned to be disseminated through peer-reviewed journal publications and presentations at local, national and international conferences.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.