Article Text

Abstract
Objectives To allow the implementation of effective injury and illness prevention programmes for road cyclists, we wanted to first identify the injury/illness burden to this group of athletes. We, therefore, undertook a systematic review of all reported injuries/illness in road cycling.
Design Systematic review.
Data sources Identification of articles was achieved through a comprehensive search of: MEDLINE, Embase, PsycINFO, Web of Science and Cochrane Library from inception until January 2020.
Eligibility criteria for selecting studies Studies reporting injuries/illness in adults participating in road cycling. Cycling commuter studies were excluded from the analysis.
Method Two review authors independently screened titles and abstracts for eligibility and trial quality. Initial search criteria returned 52 titles and abstracts to be reviewed, with 12 studies included after reviewing the full text articles.
Results The most common injuries sustained were abrasions, lacerations and haematomas accounting for 40–60% of the total injuries recorded. Fractures (6–15%) were the second most frequent type of injury. Head injuries (including concussions) accounted for 5–15% of injuries with musculotendinous injuries accounting for 2–17.5%. The upper limb was more frequently affected by injuries than the lower limb, with amateurs appearing to be at higher risk of injury/illness than professionals. Clavicle was the prevalent fracture, with patellofemoral syndrome the number one overuse diagnosis. No meta-analysis of the results was undertaken due to the inconsistent methods of reporting.
Conclusion This is the first systematic review of road cycling injuries. Injuries most often affected the upper limb, with clavicle being the most prevalent fracture and the most common overuse injury being patellofemoral syndrome.
- Injuries
- Illness
- Cycling
- Review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
BACKGROUND
Recent statistics have shown that one in four adults do not meet the recommended physical activity guidelines.1 The WHO recommend that adults should do at least 150 min of moderate-intensity physical activity or 75 min of vigorous physical activity per week.2 Road cycling can be promoted as a measure to help overcome the population’s failure to achieve the recommended levels of weekly physical activity. Road cycling can be defined as an umbrella term for recreational, racing, commuting and utility cycling that is based on well-marked roads rather than off-road tracks. It is a form of physical activity with a range of health benefits. As well as providing an effective source of aerobic exercise, it has been demonstrated that cycling can improve cognitive function and well-being in adults3 4 and is relatively cheap to participate in.5 For this reason, participation in road cycling continues to grow and UK traffic counts suggest that the number of miles cycled in 2017 surpasses that in 1997 by 29%6 and organised recreational bicycle tours continue to increase in number.7
Whilst the popularity of cycling continues to grow, maintaining participation in a sport can be affected by illness and injuries sustained while participating in road cycling.8 Studies have described the most common types of injuries experienced by amateur cyclists, namely buttock injuries, lower-back injuries and knee-overuse injuries.9 10 However, the findings to date have been heterogenous—including different subjects and inconsistent methods of data capture and reporting. Meanwhile, the studies focusing specifically on the injuries in professional cyclists have reported a high incidence of traumatic injuries such as fractures as well as overuse injuries affecting the knee and lower back.10 11
Injuries sustained during cycling also prevent progression and success at an elite level.
To date, no one has undertaken a systematic review in this area. This is vital if we are to identify the most common injury patterns across various events at different points in time.
Moreover, knowledge of the incidence and prevalence of the most common illnesses and injuries that occur during road cycling would facilitate implementation of preventative measures that reduce injury occurrence and thus increase participation and facilitate better performance by the professional road cyclists. Indeed, for elite road cycling teams, those teams with the fewest injuries/illnesses would be expected to perform the best and achieve the best results, similar to other sports.12 A systematic review of road cycling injuries/illnesses would therefore allow the development of optimal treatments as well as proposing preventative measures, helping to maintain participation, both amateur and elite, in road cycling.
AIM
This systematic review primarily aims to evaluate the incidence of injuries reported in road cycling, excluding studies that primarily look at cycling as a form of commuting. The study also aims to evaluate the effect of age on reported injuries, the most common injury type and locations as well as the difference in injury incidence between amateur and professional cyclists.
METHODS/DESIGN
This systematic review was reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidance.13 Peer-reviewed published articles, which described injuries occurring during road cycling were included. The review focussed on adults aged 18 years and over, who participated in road cycling for purposes other than commuting. We included papers on both recreational and competitive road cyclists. Studies were excluded which included only participants who cycled for commuting purposes. This study was prospectively registered on PROSPERO on 5/9/2019 (registration number CRD42019140465).
Search methods for identification of studies
Appropriate medical databases were searched, including: MEDLINE, Embase, PsycINFO, Web of Science and Cochrane Library from their inception until January 2020. In order to identify studies suitable for inclusion for this review, we devised detailed search strategies for each of the electronic databases. This was done in accordance with a medical librarian. These were based on the search strategy developed for Medical Literature Analysis and Retrieval System Online (MEDLINE) (see online appendix 1) but revised appropriately for each database. Results obtained from the searches were imported into EndNote (X7) bibliographic software. Duplicates were subsequently removed. Titles and abstracts of the studies obtained from the search strategy were independently screened by two authors (DR, NH), with IS available as an arbitrator in any disputes, although this was not required. Additional studies were identified from reviewing the reference lists of the retrieved papers through a hand search.
Supplemental material
Articles not meeting the eligibility criteria were discarded, with a record kept outlining the reason for their exclusion. Remaining articles were retrieved for further assessment. Using a standardised form tested prior to use, two review authors (DS, NH) then independently extracted data on methodological issues, eligibility criteria, interventions and study design.
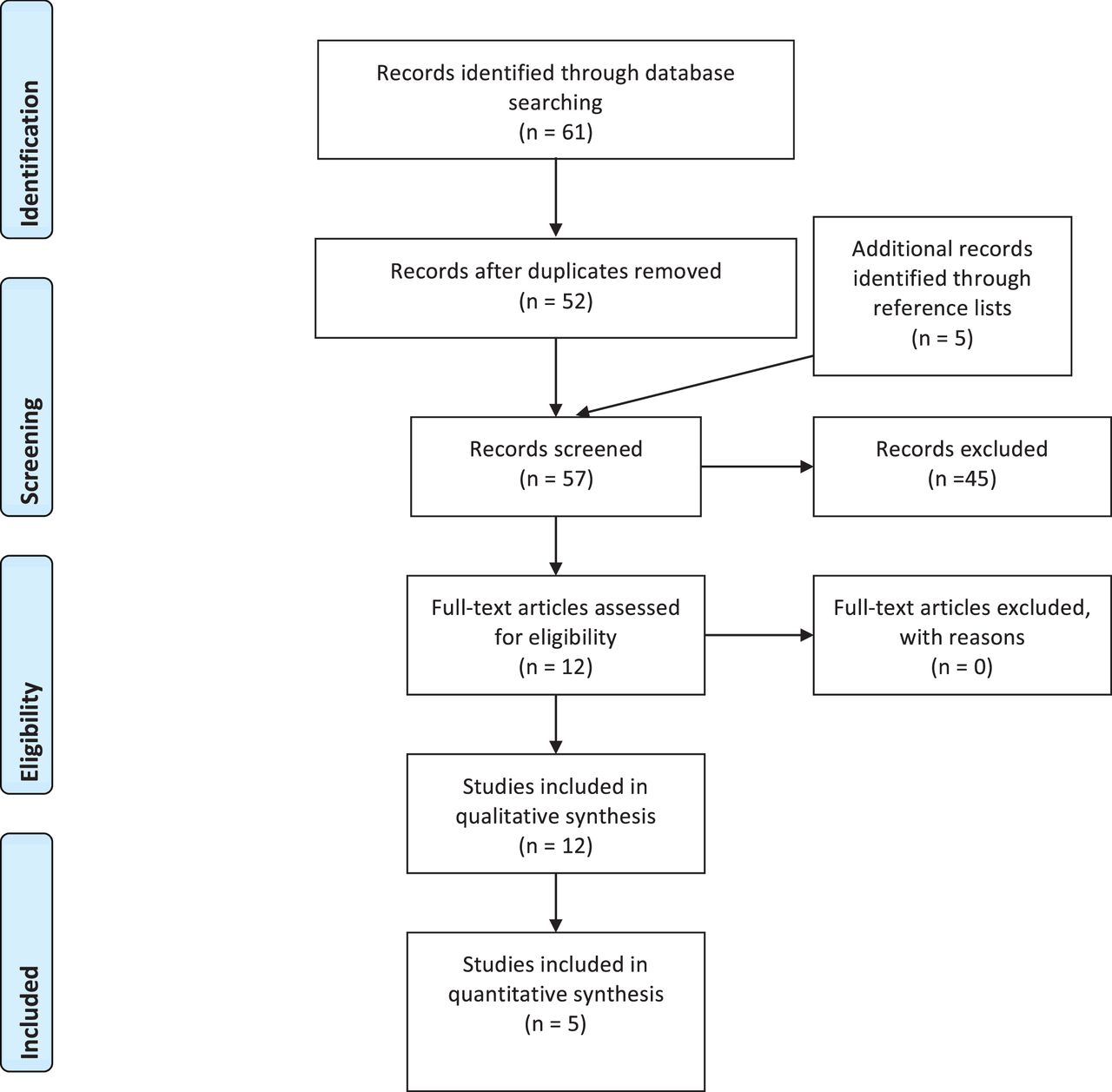
There was no blinding to study author, institution, or journal, and a record was kept of each study included in the review (see figure 1—flow diagram below).

{kind=link}
Flow diagram of excluded and included studies for the review.
Study inclusion and exclusion criteria
Study inclusion was based on the following criteria:
Adults aged ≥18, of both sexes, and recreational and/or professional road cyclists;
The outcome measure for the study focussed on injuries and/or illness sustained by the road cyclists;
The outcome measure of the study occurring during or as a result of recreational and competitive road cycling.
The exclusion criteria were:
Review articles;
Studies that included injuries and/or illness that occurred during cycling that primarily serves the purpose of commuting;
Assessment of quality and risk of bias
External validity
The included studies were independently assessed for risk of bias (‘high’, ‘low’, or ‘uncertain’) using the risk of bias tool, following guidance from the Cochrane Handbook for Systematic Reviews of Interventions.14 Where required, a third reviewer acting as an arbitrator was consulted (IS). These are listed in online supplemental table 1.
Summary of types of injury in each study (%)
Supplemental material
Assessing for heterogeneity
Diversity across the studies was assessed qualitatively in terms of participant demographics, outcome measures, and follow-up.
RESULTS
Descriptive characteristics of the studies
The search returned 61 titles and abstracts for the review, which was reduced to 52 after removing duplicates. The title and abstracts of 52 studies were reviewed (figure 1), with 7 studies being included in the review after reviewing their full texts. An additional five studies were retrieved from the reference lists of the previously identified 52 studies, thus giving us 12 studies in the review. Forty five (79%) of the studies were excluded because the sample comprised participants who cycled for commuting purposes only or they included participants under the age of 18 and a further number of papers were excluded because they were reviews.
Of the studies included in the review, nine sampled only recreational/amateur cyclists,16–18 20–25 while two studies included data for amateur and professional cyclists,15 26 with only one study focusing solely on professional cyclists.19 Five of the studies involved multi-day cycling events,16 18 19 21 25 while four involved one-day cycling events.15 17 24 26 Of the remaining studies included in the review, two involved questionnaire-based report of injuries over a defined period of time20 23 and the remaining study involved a one-year surveillance of hospital emergency room attendances for cycling injuries.22 The quality of the studies was generally low, with 3 at high risk of bias19 21 22 and the remainder being at moderate risk of bias.
Amateur cyclists
Five of the studies that included injury data from amateur cyclists focused on recreational multiday cycling events.15 16 18 21 25 Pommering et al 16 described the injuries and illnesses that occurred during a 7-day recreational cycling event in Ohio between 2013 and 2014. They reported an injury rate of 55.3 per 1000 persons in the first year of the event, and 54.6 per 1000 persons in the second year. Just over half of these were acute injuries (51.8%), while 12.3% were overuse injuries.
This injury rate reported in Pommering et al 16 is lower than that reported in Townes et al 21, who report an injury rate of 116 per 1000 riders during a six-day long AIDs charity cycling event. The high injury rate reported may be explained by the fact that many of the participants were HIV positive and had various chronic diseases that may have led to an increased frequency of medical encounters. The demographics of the cyclists in this paper, with a focus on HIV-positive patients, limits the generalisability of the findings.
On the other hand, in a one-day recreational cycling event in the United States, Emond et al,17 reported a much lower injury rate of 5 per 1000 persons. This comparably small injury rate may be explained by the much shorter distance cycled across only one day as opposed to multiple days of road cycling and the less hazardous urban route. Indeed, within this study, most emergency service calls occurred in the second half of the Bike New York tour, along downhill stretches with terrain or road hazards, identifying course selection as an important factor for injury causation.
The findings by Emond et al 17 are similar to that described by Killops et al,24 which reported the medical encounters of 102 251 race starters in the Cape Town Cycle Tour, across 3 years of the race running. The incidence rate of injury-related medical encounters was reported as 3.23 per 1000 cyclists. Of these medical encounters, 0.22 were deemed ‘serious’, that is, life-threatening. The lower rate of injury reported in this study compared to the above studies, can be explained by the exclusion of minor injuries (those that do not require medical assessment) from the study.
Poulos et al 20 examined the self-reported prospectively collected data from 2038 adult cyclists from New South Wales (Australia). We only included the data for the recreational road cyclists in this paper, as per our inclusion/exclusion criteria. Among the recreational cyclists in this study, there was an injury rate of 0.127 per 1000 km cycled. This is similar to the injury rate of 0.193 per 1000 km that was reported in Emond et al (12–13 per 100 000 person miles).17 However, this paper may have been biased by the self-reporting of injuries or illness and included only those injuries who attended the hospital for treatment. This may have led to an underreporting of minor injuries sustained during the cycle tour.
In an epidemiological analysis of acute and overuse injuries among recreational cyclists, Wilber et al 23 reported a high injury incidence, with 24.5% of the cyclists in the study sample reporting an acute traumatic injury in the past year. Similarly, 85% of the cyclists reported one or more overuse injuries, with 36% requiring medical treatment. However, the majority of cyclists competed in other sports, which would impact on the acute/overuse injury rate in these individuals.
Decock at al15 examined the incidence and aetiology of acute injuries during a competitive road cycling event in the years 2002 and 2012 for both amateur and professionals. Within the amateur 19–22 age group, the injury rate was 18.7% in 2002 and 18.0% in 2012. However, much of the data in this paper cannot be used as it does not meet the inclusion criteria of participants being over the age of 18. The injury rates from this paper are discussed below in the ‘Amateur versus Professional Road Cyclists’ paragraph.
Effect of age on reported injuries
Many of the studies also examined the effect that age has on injury rate. Pommering et al 16 found that the rate of injury/illness increased with age. Compared with the youngest age group (<30 years), individuals between the ages of 31 and 40 years had 1.7 times the rate of injury/illness, and individuals between the ages of 61 and 70 years had 1.6 times the rate of injury/illness. This finding is supported by a study by Boeke et al,18 who also studied a group of amateur cyclists competing in a 7-day bike ride. This survey found participants older than 45 years of age were more likely to require medical transport for an injury or illness. However, this study was created as a cross-sectional sampling of medical service requirements, specifically on-route services, rather than a comprehensive list of all injuries sustained during the event. In contrast to the findings of Pommering et al 20 and Boeke et al 16 18 regarding age and injury rate, Emond et al found that injury were more common in younger cyclists (RR=1.4 for age ≤35 years vs age >35 years; 95% CI, 1.0 to 2.0; p<0.05).17 Thus, the effect of age on the rate of injuries appears mixed.
Injury location and pattern
In each of the studies that included information regarding the type of injury sustained, abrasions, lacerations and haematomas were the most common (See table 1). The % of injuries recorded that were due to abrasion, laceration or haematoma was between 40 and 60% in all of the studies reported. Similarly, there was a high incidence of fractures among amateur cyclists, varying between 6 and 15% of all reported injuries, accounting for the second most common injury type. The other commonly reported injury types were ligamentous and musculotendinous injuries and head injuries (including concussion), with head and neck injuries accounting for approximately 3% of all injuries recorded.16 21 23
Three of the studies that reported % of injuries that were due to fracture also provided information regarding location of the fracture15 18 19 (table 2). In all of these studies, the shoulder girdle was the most common location. In particular, Boeke et al report that the most common bony injury each year for their recreational bike race was a clavicle fracture, which represented 44.4% of all recorded fractures from 2004 to 2008.18 This was a finding shared by Decock et al, who reported that 30.2% of all fractures involved the shoulder girdle.15 The other commonly fractured locations included the hand, wrist and lower arm. The upper limb was also more frequently affected by injuries than the lower limb.18 24
% location of total fractures in each study
Decock et al found that the most common region for ligamentous injuries was the hand, with nearly 50% of all ligament injuries occurring in this region over the 2 years recorded.15 Musculotendinous injuries were equally distributed among the elbow, hand and upper leg. However, only 18 injuries of this type were recorded over the two years of data and are therefore relatively uncommon injuries in road cycling.
Wilber et al 23 found that in amateur cyclists, overuse injuries frequently involved the development of chronic pain, most commonly in the neck, knees, groin and buttocks, hands, and back. Pommering et al 16 report that patellofemoral syndrome was the most commonly reported overuse injury. This was followed closely by iliotibial band syndrome and rotator cuff tendonitis.
Professional road cycling injuries
Only one of the studies within this review focused solely on professional cyclists. Haberle et al 19 described the prevalence and epidemiology of all injuries sustained by cyclists in the Tour de France (TDF) from 2010 to 2017. The study included information on cyclists who ‘withdrew’ from the event due to an injury although this study was at a high risk of bias as it obtained its results through review of press releases. Among the 1584 cycling entries to the TDF evaluated in the study period, 259 (16%) cyclists withdrew due to injury or illness. 138 (53%) of these were due to acute trauma and 121 (47%) were due to non-traumatic causes, for example, medical illness.
In comparison to the studies that focused on recreational and amateur cyclists in which lacerations/abrasions were the most common type of injury, Haberle et al 19 reports that fractures were the most common reason for race withdrawal. Over the 8-year period, 67 (49%) of all acute trauma injuries were due to fractures. This compares to the 17 (12%) withdrawals that were due to lacerations and/or haematoma. The location of fractures reported followed a similar pattern to that seen in the studies of amateur cyclists, with most fractures occurring in the shoulder girdle (30.2%), followed by the leg (10.4%) and wrist (9.0%).
Regarding treatment of these fractures, 43% required surgery, and those undergoing surgery had a longer return-to-competition time of 77 days vs 44 days for those treated non-surgically. However, the time to return to competition from clavicle fractures treated operatively was significantly shorter compared with the same injury treated non-operatively, suggesting that surgery for clavicle fractures may help cyclists return to competition more rapidly.
Of the withdrawals due to non-traumatic causes, 16 (13%) were due to ‘illness’, unspecified, and 16 (13%) were due to GI distress. However, there are a number of weaknesses in this study that must be noted. Most importantly, the data collected was from publicly available press reports and is therefore susceptible to inaccuracies. Similarly, the study excluded data from less severe injuries, which may not have led to withdrawal but still impacted race performance. This limits its comparability to other studies included within this review.
Another paper included in the systematic review was by Ueblacker et al 26 which reviewed acute injuries of amateur and professional road cyclists at the Hamburg UCI ProTour ‘Cyclassics’ event and found that the most common injury location was the upper limb, with 34% of all injuries occurring here. This was followed by the lower limb, which accounted for 21.5% of all injuries sustained. Similarly, 12.6% of all injuries involved the face or skull, including concussion. However, it is not possible to tell what proportion of these injuries occurred in the amateur cyclists compared to the professional cyclists.
Amateur vs professional road cyclists
The study by Ueblacker et al 26 allows comparison of the injury rates between amateur and professional cyclists competing in a similar event. The event studied had four distances; 55, 100, 155 and 243.2 km. Whilst the 243.2 km race consisted of professional cyclists only, the authors note that the 55 km consisted mainly of inexperienced amateur cyclists. In comparison to the injury rate of 8.25 per 100 000 km in the 55 km group, the professionals had a much lower injury rate of 3.10/100 000 km. Additionally, within the Decock at al15 paper, they report that the elite without contract (≥23) age group (ie, professionals), the injury rate was 15.6% in 2002 and 17.0% in 2012, which was lower than the reported injury rates in the amateurs of approximately 18%.
DISCUSSION
The main purpose of the current study was to perform a systematic review of injuries in road cycling, excluding cycling commuter studies. We also aimed to evaluate the effect of age on reported injuries, the most common injury type and locations as well as the difference in injury incidence between amateur and professional cyclists.
From our search of studies, we found only 12 studies that met the study’s inclusion criteria and all the studies used different injury reporting mechanisms. This made it difficult to collate the information due to different injury definitions, methods of injury reporting and injury classification. We were also unable to undertake a meta-analysis of our findings due to the inconsistent injury reporting. For this reason, it was decided that a narrative review would be the most appropriate study design to convey our findings and identify any patterns that were consistent across the data.
In summary from our review, the incidence rate of injuries in amateur cyclists varies widely among studies included in this review, ranging from 3.23 to 116 per 1000 persons. The most common injuries seen in cyclists were superficial skin injuries (abrasions, lacerations and haematomas) although fractures were the second most common injury reported. Of the fractures recorded, the shoulder girdle was the most affected region, with clavicle fractures being the most frequently reported. The knee was the number one area for overuse injuries in cycling, with patellofemoral pain syndrome being the most prevalent overuse diagnosis. This was followed closely by iliotibial band syndrome and rotator cuff tendonitis.
The injury rate in amateur cyclists is variable among studies, varying from 3.23 per 1000 persons to 116 per 1000 persons. This figure depends on a number of factors, some of which are based on the race demographics. These include participant details, distance cycled, cycle route/terrain and also the study design. Indeed, direct comparison of the incidence rate of injuries in the studies is not valid due to differences in the definition of a medical encounter. In 2019, the International Olympic Committee devised an International Consensus27 that aimed to define terms for injury and illness-related medical encounters. A medical encounter was defined as an ‘interaction between the medical team and a race participant requiring medical assistance or evaluation, taking place from the official start of the event, up to 24 hours after the official cut-off time of the event.’ As well as this, the Consensus differentiated minor medical encounters (interactions with a medical team not severe enough to result in withdrawal from the event) and moderate medical encounters (interactions with a medical team that are severe enough to result in withdrawal from the event). Use of these definitions was seen in the study by Killops et al 24 although not in the other studies within the review. The use of the International Consensus definitions of medical encounters allows direct comparison to other sports using the same method of injury classification. These standardised definitions should be used in future road cycling epidemiology studies along with other best practice guidelines.28 Similarly, in future epidemiology studies of injuries/illness in road cycling, medical encounters should be reported per 1000 race starters (or 10 000/100 000 if there is a small number of specific encounters) and per 1000 hours of competition. This allows comparison to other cycling events as well as to other sports. Standardisation of the way in which we report medical encounters will allow completion of meta analyses and subsequently higher quality epidemiological data.
The most common injuries seen in our review were abrasions, fractures, overuse and head injuries, including concussions, with the upper limb generally being more affected than the lower limb. This is in contrast to other sports, for example, football, which have higher rates of lower than upper limb injuries.29 Concussion and head injury percentages in the review varied between 2% of all injuries in Haberle et al up to 15% in Emond et al This is similar to the general reported rates of concussion in sport. A recent review paper quoted the annual risk of concussion to athletes in organised sports is between 2 and 15%.30 In a paper looking at the population-based incidence rates for head injuries and total injuries resulting from bicycle crashes, Thompson et al 22 found that 28% of those treated in the emergency room were treated for head injuries. Thus, head injuries and concussions are prevalent within road cycling. However, road cycling does not currently have a discipline-specific concussion assessment and management protocol.31 The current authors have however proposed a potential concussion protocol for use in elite road cycling.32 The high number of concussions and head injuries as a percentage of the overall injuries identified in this review, indicates the need to test and refine a concussion protocol in road cycling. Additionally, collaborating with road cycling manufacturers, for example, helmet manufacturers, to maintain the highest safety standards for riders will be key. Researchers also need to be able to identify the consequences of concussion in road cycling. This therefore requires ongoing, prospective injury and illness surveillance studies within road cycling, with consistent methods of injury and illness reporting,28 allowing more accurate and meaningful comparison between studies and between sports.
Emond et al 17 found a higher rate of injuries in amateur cyclists at points of the road course, which require more technical bike skills, including on the downhill section of the course and on sections with more road furniture present. Thus, injury prevention also needs to consider course and terrain selection, working with course organisers to ensure an appropriate race for the level of the road cyclists. Awareness of course design allows riders to identify parts of the course that may have an increased potential for crashes before starting the race. Riders should be properly educated regarding the course design, including topographic data and location of food and rest stops.
Although it was only one paper, Ueblacker et al 26 looked at the injury rates in amateur vs professional cyclists and found a lower injury rate in the professional cyclists. This is in contrast to other sports, with the professional athletes generally having a higher injury rate than the amateurs.33–36 Possible explanations for this might be the bike handling skills being less in the amateurs compared to the professionals and therefore, they fall off the bike more, causing more acute injuries, as well as the amateurs potentially taking more risks during the competitions than they would normally take in training. One public health prevention measure for reducing road cycling injuries could be to introduce compulsory ‘cycling efficiency’ skills prior to a competition, to ensure the riders, particularly the novices, can ride to a certain standard. Moreover, the papers reviewing injuries in amateur cyclists found higher injury rates in older cyclists, particularly over the age of 45 years. Road racing organisers should therefore improve the pre-participation advice distributed to amateurs undertaking a cycling event to ensure appropriate training and preparation has been completed prior to competing in a cycling competition, particularly in those events with a large proportion of participants over the age of 45 years old.
In our systematic review of road cycling injuries, there was a high rate of traumatic fractures, the most prevalent being clavicular. One paper included in the review by Haberle et al 19 found that surgical fixation vs conservative management for fractures had a longer return to competition, 77 days vs 44 days, respectively. This may be a reflection of injury severity, with the more severe injuries most likely to require surgery. However, the time to return to competition from clavicle fractures treated operatively was significantly shorter compared with the same injury treated non-operatively, suggesting that surgery for clavicle fractures may help cyclists return to sport more rapidly. Indeed, surgical fixation of clavicular fractures is the typical management in elite cyclists, allowing the rider to return to competitive action quicker than compared to conservative management. Medical professionals working in road cycling need to optimise prevention of this injury and this could involve partnership work with clothing manufacturers to develop ‘clavicular protection plates’ within jerseys, for example, as well as optimising the bone health of our riders.37
The knee is the anatomical site most involved in overuse injuries within road cycling,31 with patellofemoral syndrome (PFS) being the most prevalent manifestation.16 In elite sport, daily well-being monitor of athletes is undertaken.38–40 Thus, two questions to consider asking explicitly to elite/professional road cyclists on a daily basis within the well-being monitoring would be, ‘do you have any knee pain today?’ and ‘if you do, how would score this from 1 to 5, with 1 being mild and 5 very severe, enough not to ride the bike today?’ This would allow the medical team to monitor the road cyclist for developing PFS/knee pain symptoms and therefore to initiate appropriate load management reduction and ongoing subjective monitoring of the pain level, to ensure it does not become a chronic problem.
Haeberle et al 19 found that 16% of race entries to the TDF prematurely withdraw from the race due to injury or illness but this study is at high risk of bias. Although no direct comparison can be made between road cyclists and football, Junge et al 29 report that approximately one injury per match at the football World Cup, 2014, would cause loss of training or matches. Further studies are therefore required to have consistent reporting of injuries and illness in road cycling, including injury severity, allowing comparison with other sports.
Strengths and limitations
The current study is the first to review the incidence of injuries sustained during cycling events. It also identifies the most prevalent location and types of injuries that medical professionals working in road cycling are likely to manage. The search criteria were thorough and systematic, allowing a thorough review of the injury and illness literature in road cycling. Through identification of the common injuries and illnesses, this review paper allows us to consider prevention mechanisms that could be initiated in road cycling, helping to protect the health of the cyclists.
Papers included in this review were mainly documenting the injury and illness risk to road cyclists during tournament and competition events. We know that this will likely underestimate injury and illness rates as opposed to season-long surveillance studies,41 as participants are more likely not to compete if they have a significant injury or illness that would have affected participation. That is, they will self-select prior to the study starting and withdraw if they have significant injury and these injuries/illnesses would therefore be missed by these studies. Nine studies were of competitions and therefore the number of injuries reported in these studies likely underestimates the true extent of injuries and illness experienced within road cyclists. Whilst the review was registered on PROSPERO, this was done in retrospect on completion of the review.
Implications for future research and road cycling practitioners
The current study allows road cycling practitioners to implement preventative measures that will minimise drop-out from competitive cycling events and cycling as a recreational activity. Injury and illness rates were reported inconsistently in the included studies and we were therefore unable to undertake a meta-analysis of our findings. This highlights the need to publish an expert consensus statement for reporting of injuries and illnesses in road cycling, in keeping with recent published guidance.28 If implemented, the consistent reporting of injuries will allow high-quality meta analyses to be undertaken focusing on injuries within road cycling.
CONCLUSION
This is the first systematic review undertaken of road cycling injuries/illness in amateur and professional cyclists. The most prevalent injuries experienced in road cycling are abrasions, fractures (particularly clavicle), overuse (the most common being of the knee) and head injuries, with upper limb being more affected than the lower limb for injuries. These are different injury patterns to other sports and therefore require unique harm minimisation strategies to improve rider safety. Amateurs appear to have a higher risk of injury than compared to professional cyclists, and this may require specific harm minimisation strategies targeted to this group, such as bike handling skill courses. This review also highlights the different ways that injury and illness are reported in road cycling epidemiology and we therefore call on future studies to implement standardised injury/illness reporting to allow direct comparison between road cycling studies as well as with other sports.
What is already known
1 in 4 adults does not meet the physical activity guidelines recommended by the WHO (WHO).
Road cycling is an effective form of exercise that can help overcome the population’s failure to meet physical activity guidelines.
Injuries sustained during road cycling can act as a deterrent to future participation; both at amateur and professional levels.
There have been no systematic reviews focusing on the types of injuries experienced by amateur and professional road cyclists.
Knowledge of the most prevalent road cycling injuries and illnesses would allow better prevention to be put in place, allowing improved safety of participation in road cycling.
What are the new findings
The incidence rate of injuries in amateur cyclists varies widely among studies included in this review, ranging from 3.23 to 116 per 1000 persons.
The upper limb is more affected in road cycling than the lower limb in terms of injuries sustained.
The most prevalent injuries in road cyclists were superficial injuries involving the skin (abrasions, lacerations and haematomas) followed by fractures.
The clavicle is the most common location of fractures. Surgical management of clavicle fractures allows quicker return to competitive action than compared to conservative management.
Injuries involving the head, such as concussion, are frequently reported among road cyclists.
The most common body area for overuse injuries in road cycling is the knee, with patellofemoral pain being frequently diagnosed.
Difficult cycling terrain increases the risk of injury among cyclists. Future cycling events should provide race information prior to the event to reduce the risk of injury.
Road cycling injury and illness epidemiology studies have reported their findings inconsistently to date. We call on future studies to be reported as per current best practice, allowing comparison of findings.
REFERENCES
Footnotes
Twitter Neil Heron @neilSportDoc.
Contributors NH conceived the idea of the study with IS; NH undertook the literature search, supported by DR; DR produced a 1st draft of the paper and all authors reviewed and agreed the final draft of the review.
Competing interests NH and IS are team physicians to Team Ineos, World Tour Professional Cycling team.
Ethics approval Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data related to this publication has been made freely available to the journal and will be published with the article.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.