Article Text

Abstract
Background/Aim Physical inactivity (PIA) is a growing global health problem and evidence suggests that PIA is a key driver for cardiovascular and chronic diseases. Recent data from South Africa revealed that only about half of the children achieved recommended daily physical activity (PA) levels. Assessing the intensity of PA in children from low socioeconomic communities in low-income and middle-income countries is important to estimate the extent of cardiovascular risk and overall impact on health.
Methods We conducted a cross-sectional survey in eight quintile 3 primary schools in disadvantaged communities in the Port Elizabeth region, South Africa. Children aged 10–15 years were subjected to PA, blood pressure, cholesterol, blood glucose and skinfold thickness assessments. Cardiovascular risk markers were converted into standardised z-scores and summed, to obtain a clustered cardiovascular risk score.
Results Overall, 650 children had complete data records. 40.8% of the children did not meet recommended PA levels (ie, logged <60 min of moderate-to-vigorous physical activity (MVPA) per day). If quartiles were developed based on children’s cardiorespiratory fitness (CRF) and MVPA levels, a significant difference was found in clustered cardiovascular risk among children in the highest versus lowest fitness (p<0.001) or MVPA (p<0.001) quartiles.
Conclusions CRF and objectively assessed PA are closely linked with children’s clustered cardiovascular risk. Given that 4 out of 10 South African schoolchildren from marginalised communities do not meet international PA recommendations, efforts should be made to ensure that promoting a physically active lifestyle is recognised as an important educational goal in primary schools.
Trial registration numbers ISRCTN68411960 and H14-HEA-HMS-002.
- Cardiovascular
- Cholesterol
- Non-communicable disease
- Physical activity
- Risk factor
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Sedentary lifestyle and physical inactivity (PIA) are growing global health issues and evidence suggests that PIA is a key driver for cardiovascular and chronic diseases.1 At a global scale, the prevalence of obesity increased at an alarming rate from 0.9% in girls and 0.7% in boys in 1975 to 7.8% in girls and 5.6% in boys in 2016.2 Recognising the negative public health consequences of a sedentary lifestyle encouraged new research to investigate and promote public health interventions to improve physical activity (PA).3–6 The first PA guidelines for children were published in 1988.7 At present, children aged 5–17 years are advised to pursue moderate-to-vigorous physical activity (MVPA) for at least 60 min per day.8 The current and projected PA levels for low socioeconomic status (SES) communities are worse in low-income and middle-income countries (LMICs), compared to more affluent populations in LMICs.9 10
In low socioeconomic communities in South Africa, unsafe neighbourhoods and poor school facilities typically offer children no or only limited opportunities to play and be active.11 Hence, we hypothesise that a considerable portion of South African children from poor neighbourhoods will not meet the recommended PA guidelines. For instance, in 2018, only around half of South African children were reported to have achieved daily PA recommendations.12 In order to estimate the health impacts of insufficient PA in children from lower socioeconomic communities, it is necessary to examine their cardiovascular disease risk factors.13
We designed a cross-sectional study in the Port Elizabeth region in South Africa with the following aims. First, we described the cardiovascular health risk, PA behaviour and cardiorespiratory fitness (CRF) levels of children attending primary schools in lower socioeconomic communities. Second, we examined differences in these variables dependent on children’s age, sex, SES and ethnicity. Third, we investigated whether PA and CRF are independently associated with a composite measure of children’s cardiovascular health risk.
METHODS
Study setting
The study was conducted in eight quintile 3 primary schools located in disadvantaged communities in and around Port Elizabeth, South Africa. It should be noted that South African schools are ranked into five quintile groups in accordance with the national poverty table, and based on the income levels, dependency ratios and literacy rates in a specific area.14 The procedures to select the schools for this study have been described in the study protocol.15
Participants’ involvement and procedures
The current investigation is based on cross-sectional data from the 2-year follow-up of the ‘Disease, Activity and Schoolchildren’s Health’ (DASH) study. DASH, a cluster-randomised controlled trial, implemented different school-based health interventions (ie, PA promotion, health education, deworming and nutritional supplementation) over a period of 20 weeks in order to improve children’s health status. Children were eligible for inclusion if they assented, did not simultaneously participate in other clinical trials during the study period and did not suffer from medical conditions (as determined by qualified clinical personnel) that prevented participation. Written informed consent was obtained from parents/legal guardians before the first data assessment and after sharing detailed written and oral information about the study’s aims, procedures, risks and benefits. The study protocol was approved by the responsible ethics committees in South Africa and Switzerland. Approval was also obtained from South Africa’s Eastern Cape Provincial Departments of Education and Health.
Participants were not directly involved in the design of the study presented here. However, the development of the research questions, study procedures and outcome measures were informed by participants’ experience, needs and preferences, as expressed in the formal meetings arranged with education authorities, where these matters were discussed. Caregivers (eg, parents and guardians of participating children) and lay people (eg, education authorities) were involved in the recruitment to and conduct of the study. Recruitment commenced in September 2014, baseline assessment was done in February 2015 and 2-year follow-up data were obtained in February and March 2018. At baseline, all children (n=1009) were in grade 4 and their age ranged between 8 and 13 years. The present study included 650 children who had complete data records at follow-up; hence, the children’s age ranged from 10 to 15 years. At school level, our research team, together with the Department of Health, disseminated the main findings.
Measures
Blood pressure was assessed with a validated oscillometric digital blood pressure monitor (Omron M6 AC, Hoofddorp, Netherlands). Three measurements were performed, and the mean of the last two measurements were employed as indicators of systolic and diastolic blood pressure. Using a Harpenden skinfold calliper (Baty International, West Sussex, UK), skinfold thickness was assessed three times at triceps and subscapular skinfold sites. The mean of all six measurements was taken as the overall skinfold thickness index.16 Capillary blood sampling was used to assess blood markers for cardiovascular risk, using the Alere Afinion AS100 analyser (Abbott Technologies, Abbott Park, Illinois, USA). Total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides and blood glucose (HbA1c) were assessed using fasting capillary blood samples.17 Evidence of the clinical utility and accuracy of this fingerstick technology has been described previously.18
To objectively assess children’s PA, children wore a light triaxial accelerometer device (ActiGraph wGT3X-BT, Pensacola, Florida, USA) for 7 consecutive days. Evidence for the validity and reliability of this device has been published.19 Children were instructed to wear the accelerometer around the hip, except for activities that involved contact with water. Data were recorded at a sample rate of 30 Hz. Analysis was performed with ActiLife software version 6.13.2, using raw data set to epochs of 10 s. Non-wear time was determined using the algorithm defined by Troiano and colleagues.20 Children’s data were considered valid if the accelerometer was worn for at least 8 hours a day, on 4 weekdays and 1 weekend day.21 22 Furthermore, data were restricted to the period between 06:00 and midnight, hence 18 hours per day. Using the cut-points for children defined by Evenson, we considered time spent sedentary, and in light physical activity (LPA), moderate physical activity (MPA) and vigorous physical activity (VPA).23 MPA and VPA were summed up to generate an overall index for MVPA. For all PA indices, results are reported in min/day.
Based on a standardised test protocol, children’s CRF was assessed with the 20 m shuttle run test, with a starting pace of 8 km/h. Based on the number of completed laps, children’s maximum oxygen uptake (VO2 max) was estimated, using a standard protocol.24 25 Evidence for the reliability and validity of the 20 m shuttle run test has been reported.26
Statistical analysis
Descriptive statistics for all study variables are reported for the total sample. In the case of severe non-normality (skewness and kurtosis values of ≥ |2| and ≥ |7|, respectively), measured values were log-transformed (natural log) before calculating inferential statistics.27 Univariate analyses of variance (ANOVAs) were performed to examine differences based on children’s age, sex, SES and ethnicity. χ2 tests were carried out to examine whether based on children’s age, sex, SES and ethnicity, some children were over-represented/under-represented in the group that did not meet current PA standards. Additionally, a series of linear regression analyses were performed to determine whether and to what extent PA and CRF might predict the various cardiovascular risk markers. Since ANOVAs revealed significant differences (p<0.05) between schools in most of the study variables, we used mixed linear regression with random intercepts for school classes to account for the nested nature of the data (learners assessed in classes) and for potential influences of class and school on the association between PA and CRF with the cardiovascular risk markers. The regression analyses were further controlled for children’s age, sex, SES and ethnicity. To examine the independent contribution of CRF and PA, analyses were controlled for total time spent in MVPA, when CRF was used as a predictor. By contrast, when PA indicators were used to predict cardiovascular risk, the analyses were controlled for CRF. All risk markers were z-standardised and summed up to obtain a clustered cardiovascular risk score. Similar to previous publications based on data of the European Youth Heart Study,28 the following formula was used in the present study to compute the clustered risk score: (systolic + diastolic blood pressure/2) + mean of six skinfold measurements + (HDL-cholesterol × −1) + LDL-cholesterol + triglycerides + blood glucose. To examine whether (a) students classified to different CRF and PA quartiles and (b) students who met versus did not meet current PA guidelines differ in clustered cardiovascular risk, three analysis of covariance (ANCOVAs) (controlled for age, sex, SES and ethnicity) were performed. Differences between the different quartile groups were analysed with Bonferroni posthoc tests. All analyses were carried out with SPSS version 24 for Mac. Associations were considered as significant, if resulting p values were <0.05.
RESULTS
Demographic features of the 650 children who had complete data records are shown in table 1. In short, the sample was composed of 351 girls and 299 boys with a mean age of 12.4 years (SD 0.9 years) at endline. In terms of ethnicity, 384 children were black African, 232 were of coloured ethnicity, while for the remaining 34 children, this information was not available. Although children lived in disadvantaged areas, most of them had relatively high scores on the SES index. Table 1 also provides descriptive statistics for cardiovascular health risk markers, PA behaviour indices and CRF. Overall, 40.8% of the children did not meet recommended PA levels, therefore achieved <60 min MVPA per day.
Descriptive characteristics of 650 children from Port Elizabeth, South Africa, in February and March 2018
As shown in table 2, children aged 13–15 years had higher measured systolic and diastolic blood pressure than their younger counterparts aged 10–12 years. While older children engaged less in sedentary activity and LPA, they had higher scores for MPA, VPA, MVPA and CRF. Compared to boys, girls had higher readings for diastolic blood pressure, thickness of skinfolds, triglyceride levels and sedentary activity. Girls also had a higher clustered cardiovascular risk than boys. By contrast, boys had higher scores for HbA1c, LPA, MPA, VPA, MVPA and CRF. Differences between boys and girls were particularly marked with regard to PA behaviour and CRF, where levels of explained variance ranged from 2.1% to 28.4%. Only small differences were observed with regard to children’s SES. Children with higher SES had higher skinfold thickness and performed somewhat more poorly in the CRF test. Ethnic differences appeared in most study variables showing that black African children had higher scores with regard to thickness of skinfolds, sedentary activity and LPA, whereas coloured children had higher scores for diastolic blood pressure, total cholesterol, LDL cholesterol, triglycerides, MPA, VPA, MVPA and CRF. The portion of children not meeting international PA recommendations was higher among younger children (χ2(1650)=6.0, p<0.05, 44.6% vs 34.9%), girls (χ2(1650)=108.0, p<0.001, 59.3% vs 19.1%) and black African children (χ2(1650)=12.3, p<0.001, 47.1% vs 32.8%).
Differences in outcome and predictor variables, based on children’s age, sex, socioeconomic status and ethnicity of 650 children from Port Elizabeth, South Africa, in February and March 2018
Table 3 provides information on whether CRF and PA indices are independently associated with cardiovascular health risk markers. After controlling for MVPA, class-in-school (random intercept) and potential confounders (age, sex, SES and ethnicity), higher CRF levels were negatively associated with systolic blood pressure, thickness of skinfolds, total cholesterol and LDL cholesterol. A statistically non-significant trend was also observed for diastolic blood pressure. Higher levels of CRF were significantly and negatively associated with the clustered cardiovascular risk index. Similar (although weaker) relationships were observed for MVPA. Thus, after controlling for class-in-school (random intercept), CRF and potential confounders (accelerometer wear-time, age, sex, SES and ethnicity), children who engaged in more MVPA had lower systolic blood pressure, lower thickness of skinfolds and a lower clustered cardiovascular risk. A statistically non-significant trend was also observed for total cholesterol. Furthermore, table 3 shows that children who spent more time in sedentary activities had higher systolic blood pressure, although sedentariness was not significantly associated with any other cardiovascular health risk marker.
Prediction of cardiovascular health risk markers with physical activity and cardiorespiratory fitness among 650 children from Port Elizabeth, South Africa, in February and March 2018
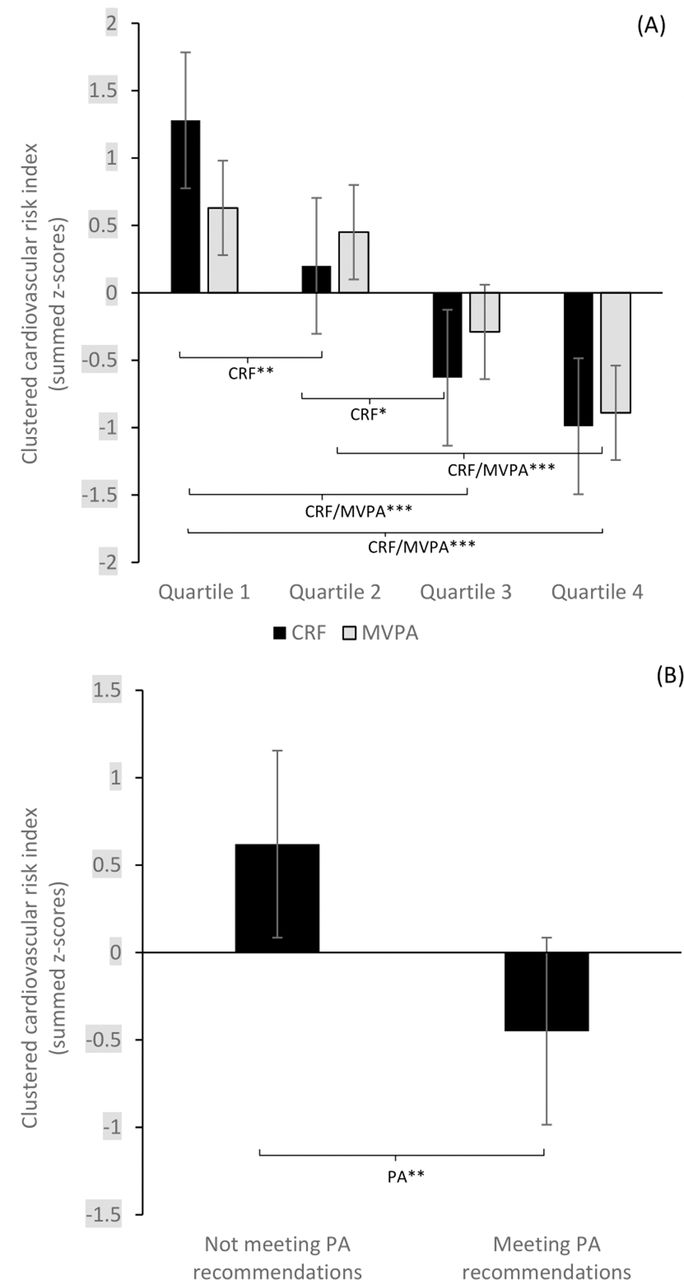
Based on ANCOVAs, figure 1 shows that if children’s CRF and MVPA levels were based on quartiles, a clear gradient of lower clustered cardiovascular risk among children with higher CRF or MVPA levels could be observed (figure 1A). The same is true if children who met PA recommendations were compared with peers who did not (figure 1B).
{kind=link}
Means for clustered metabolic risk, stratified by quartiles of cardiorespiratory fitness (CRF) and moderate-to-vigorous physical activity (MVPA) (A) and by current international physical activity (PA) recommendations (B). Error bars represent SE. Data are adjusted for age, sex, socioeconomic status (SES) and ethnicity. */**/***Differences are significantly different (*p<0.05, **p<0.01, ***p<0.001) between groups. If more than two groups are compared, group differences are based on Bonferroni posthoc tests.
DISCUSSION
Quartiles based on children’s CRF or MVPA levels showed evidence of decreased clustered cardiovascular risk among children with higher fitness or MVPA levels living in lower socioeconomic neighbourhoods in Port Elizabeth, South Africa. To our knowledge, objective assessments of PA from lower socioeconomic communities in South Africa, as a representative of a LMIC, have not yet been carried out to the extent and intensity of this study.
Compared to the European Youth Heart Study, we used a slightly different formula to calculate an overall cardiovascular risk score. Nevertheless, our findings are in line with those reported by Andersen and colleagues28 and Ekelund and colleagues,29 indicating that low levels of PA are linked to a clustering of cardiovascular disease risk factors in South African children, and particularly children living in socioeconomically deprived neighbourhoods. Moreover, our findings show that 4 out of 10 children do not meet recommended PA guidelines (at least 60 min of daily MVPA), with insufficient PA being particularly widespread among girls, black Africans and children aged 10–15 years. The low PA levels in our cohort of children from disadvantaged urban settings in townships of Port Elizabeth are not surprising given that options to perform PA are limited due to insecurity and poor school and public infrastructure.30 The conditions are compounded by a lack of basic services, including sewage and road infrastructure, overcrowding, violence, unemployment, large class sizes, lack of teachers with adequate physical education training and qualifications, lack of motivation and commitment, and a diverse set of learners and learning abilities in a single classroom.31 These contextual factors directly and indirectly influence children’s health and well-being.
LMICs, including South Africa, are experiencing rapid urbanisation, which might have considerable negative effects on social PA inequalities in marginalised communities.32 In addition, policy change also plays a significant role in promoting this situation, as physical education in schools lost its stand-alone status and was marginalised in the South African national curriculum in 1994. Indeed, physical education was combined with other subjects in the ‘Life Orientation’ learning area. Thus, higher cardiovascular risks in children may be linked to the absence of institutionalised/mandatory PA programmes in schools. Supplementary analyses indicated that children accumulated very little PA while at school. This raises the question of whether a single sport lesson per week is sufficient and whether such a physical education lesson is taught intensively enough for the individual learners. Earlier results obtained from the DASH project showed that higher CRF is associated with better cognitive performance in schoolchildren.33
The following limitations should be considered when interpreting the key findings of our study. First, due to the cross-sectional nature of the data, we are unable to infer causality. Second, it is difficult to record all types of activities through waist-worn accelerometers, which might have led to an underestimation of PA levels. Third, due to natural fluctuations, a 7-day assessment period may not be fully representative of a child’s ‘typical’ PA level and may still be too short and dependent on the climatic conditions during the assessment period. Fourth, the blood pressure results of the study subjects may be slightly increased due to experiencing an unknown situation.
CONCLUSION
Collectively, CRF and objectively assessed PA seem to be closely linked with a composite measure of children’s cardiovascular risk. Given that 4 out of 10 South African schoolchildren do not meet international PA recommendations, efforts should be made to ensure that a physically active lifestyle is seen as an important educational goal. We believe that physical education at school can make an important contribution to children’s overall PA levels. Hence, concerted actions are required for children in low-resourced communities in South Africa to (i) improve the status of, and resources allocated to, physical education in the South African school system and (ii) create conducive environments (eg, teacher training in physical education) that allow and stimulate regular PA in children, which meet the prognostic importance in childhood and adolescence of critical development periods for a healthy adult life.
What are the new findings?
Here, we present physical activity and cardiorespiratory fitness profiles among 10-year-old to 15-year-old children from disadvantaged communities in South Africa.
We found that when quartiles were formed based on children’s cardiorespiratory fitness or moderate-to-vigorous physical activity levels, there was a clear gradient of decreased clustered cardiovascular risk among children with higher fitness or higher moderate-to-vigorous physical activity levels.
How might it impact on clinical practice in the future?
The findings of our study emphasise the importance of a physically active lifestyle and call for action to address these issues in underserved communities and schools such as those in the townships of Port Elizabeth.
There is a pressing need to design policies and create environments that allow children to achieve international physical activity recommendations. Since the cardiovascular risk of children living in marginalised communities depends on various lifestyle factors, longitudinal and comprehensive monitoring is also required.
Acknowledgments
The authors are grateful to the children and parents/guardians for their willingness to participate in the study. Special thanks are addressed to the education authorities of the participating schools, for facilitating support and collaboration of the teaching staff and the school health services. Moreover, we thank all the participating MSc and Honours students for their dedicated contribution to data collection.
REFERENCES
Footnotes
Contributors IM, CW, RDR, HS, PS, NP-H, JU, UP and MG designed the study, established the methods and wrote the original study protocol. All other authors contributed to the development of the study protocol. IM, CW, RDR, LA, JD, SG, NJ, SN, DS, UP and MG conducted the fieldwork of the study. IM, LA, JD, SG, NJ, SN and DS managed data entry, cleaning and preparation of the database. Statistical analysis was done by MG. IM wrote the first draft of the manuscript with support of MG. CW, RDR, AA, LA, JD, SG, NJ, SN, SDR, DS, HS, PS, CW, NP-H, JU and UP provided comments on the drafts and have read and approved the final version of the manuscript prior to submission. IM and MG are guarantors of the paper.
Funding The cross-sectional study presented here was financially supported by the Novartis Foundation (Basel, Switzerland). The funder had no role in study design, data collection, data analysis or data interpretation, nor the decision to submit the paper for publication.
Competing interests The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf, indicating no support from any other organisation for the submitted work, no financial relationships with any other organisations that might have an interest in the submitted work in the previous three years, and no other relationships or activities that could appear to have influenced the submitted work. AA and SDR are employees of Novartis Foundation (Basel, Switzerland); ChrW is an employee of Novartis International AG (Basel, Switzerland). All other authors declare no financial competing interests.
Ethics approval This study was approved by the ethics committees of Northwest and Central Switzerland (EKNZ; reference no. 2014-179, approval date: June 17, 2014), the Nelson Mandela University (NMU; study number H14-HEA-HMS-002, approval date: July 4, 2014), the Eastern Cape Department of Education (approval date: August 3, 2014) and the Eastern Cape Department of Health (approval date: November 7, 2014). The study is registered at ISRCTN registry under controlled-trials.com (identifier: ISRCTN68411960, registration date: October 1, 2014).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The raw datasets are available from the corresponding author on reasonable request.