Article Text

Abstract
There is a need for effective therapeutic options for resistant patellar tendinopathy. Ultrasound (US)-guided arthroscopic debridement has demonstrated promising clinical results.
Objectives To prospectively evaluate pain, function, tendon structure and adverse events after US and colour Doppler (CD)-guided arthroscopic debridement for persistent painful patellar tendinopathy.
Materials and methods Twenty-three consecutive patients (19 males and 4 females, mean age 28 years (±8), symptom duration 25 months (±21)), who had failed conservative management including progressive loading, were included. US+CD and ultrasound tissue characterisation (UTC) examination verified the clinical diagnosis and quantified baseline tendon structure. Patients were treated with US+CD-guided arthroscopic debridement followed by a specific rehabilitation protocol. Outcomes were VISA-P score for pain and function and UTC for tendon structure. Adverse events were specifically elicited.
Results At 6-month follow-up, mean VISA-P score increased from 40 (±21.0) to 82 (±15) (mean deviation (MD)=42.0, 95% CI 32 to 53, d=2.4), while organised echo pixels (combined UTC type I+II) increased from 55.0% (±17.0) to 69.0% (±15.0) (MD=14.0, d=0.7, 95% CI 2 to 21). Both outcomes exceeded minimum detectable change values. Twenty-one participants returned to their prediagnosis activity levels, and there were no significant adverse events.
Conclusions US-guided patellar tendon debridement for persistent patellar tendinopathy improved symptoms and tendon structure without complications at 6-month follow-up. A majority (21/23) of the patients returned to their preinjury activity level. Further studies with longer follow-ups, preferably randomised and controlled, are needed.
- knee injuries
- surgery
- tendinopathy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings
Patellar tendinopathy is difficult to manage in active athletes.
Conservative management is not always successful.
Traditional surgery is no better than exercise therapy.
Patellar tendon debridement has demonstrated promising results.
There was significant improvement in validated outcome measures.
Introduction
Patellar tendinopathy is a common overuse condition and difficult to treat.1 2 Conservative management using loading regimens is first line treatment. Both painful eccentric quadriceps training3 4 and heavy-slow resistance training5 have demonstrated promising results, but certain subgroups cannot return to full training and sports.6 7 Alternative loading programmes, such as isometric exercise approaches8 9, and adjunct interventions such as Extracorporeal Shockwave Therapy10 and injection therapy,11–15 have shown mixed and limited results.
Surgery is considered after failed conservative treatment, but traditional intratendinous approaches demonstrate varying and unreliable results.16 17 Using similar principles as polidocanol11 18 19 or high volume12 13 20–22 injection, interference with the peritendinous nerve and vessel rich region outside the deep (dorsal) aspect of the proximal patellar tendon,21 23 an US and DP-guided arthroscopic-debridement procedure has demonstrated positive outcomes in four clinical studies.18 19 24–26
There is no clear relationship between changes in structure, pain and function in tendinopathy, with some therapies leading to improved pain and function without structural change27–29 while other therapies leading to improved structure with changes in pain.30 To evaluate structure, there is a lack of objectivity and reliability using 2D US+CD or MRI.31 Recently, ultrasound tissue characterisation (UTC) has been used to visualise tendon structure and quantify tendon matrix integrity.32 33
This prospective case series aimed to establish outcomes post-US+DP-guided arthroscopic tendon debridement in participants with persistent painful patellar tendinopathy. Clinical status and function using the VISA-P, and tendon structure using UTC, was used for evaluation.
Material and methods
Participants presenting with persistent painful patellar tendinopathy at Pure Sports Medicine (London, UK) between August 2013 and October 2017 and could be evaluated at 6 months, were included. There were 19 males and 4 females (mean age 28.1 years, ±8.2) with a mean symptom duration of 24.8 months (±21.1). All had previously failed conservative management including progressive loading (eccentric training n=13; heavy slow resistance n=10) and intermediate interventions including injection therapy (cortisone n=8, high volume n=5, sclerosing polidocanol n=1) or shockwave therapy (n=10). All were active in sport including nine from rugby, five from endurance running, four from football and one from track and field, tennis, cricket, Gaelic football and cross fit. Sixteen were elite athletes.
Ultrasound (US)+colour Doppler (CD) (GE logic E10) was performed using a high frequency linear probe (MHz 6–15) with the participant in supine position with the knee extended. In all subjects, US+CD showed a thickened proximal patellar tendon with irregular structure mainly deep and central in the tendon, including focal hypoechoic regions and high blood flow arising from the Hoffa’s fat pad and infiltrating into the focal hypoechoic regions. There were also changes on the superficial side of the tendon in 17 cases demonstrating localised thickening of the paratenon including high blood flow figure 1. In four cases, there was a bony spur or calcification distal to the inferior pole of the patella.

Blood vessels on superficial proximal patellar tendon.
UTC was performed with participants in a seated position with the foot on the floor and the knee flexed to 100°. The transducer was placed perpendicular to the long axis of the tendon. Using UTC, the echo structure of the patellar tendon was quantified for a distance of 20 mm from the proximal insertion of the patellar tendon to the mid-portion of the tendon. Contours were performed on this region of interest prior to quantification using a computer algorithm.32 33 Quantification was expressed as a percentage of organised and disorganised tissue with percentage of type I and II echopixels consistent with organised tissue and type III and IV echopixels consistent with disorganised tendon tissue.
Surgical procedure
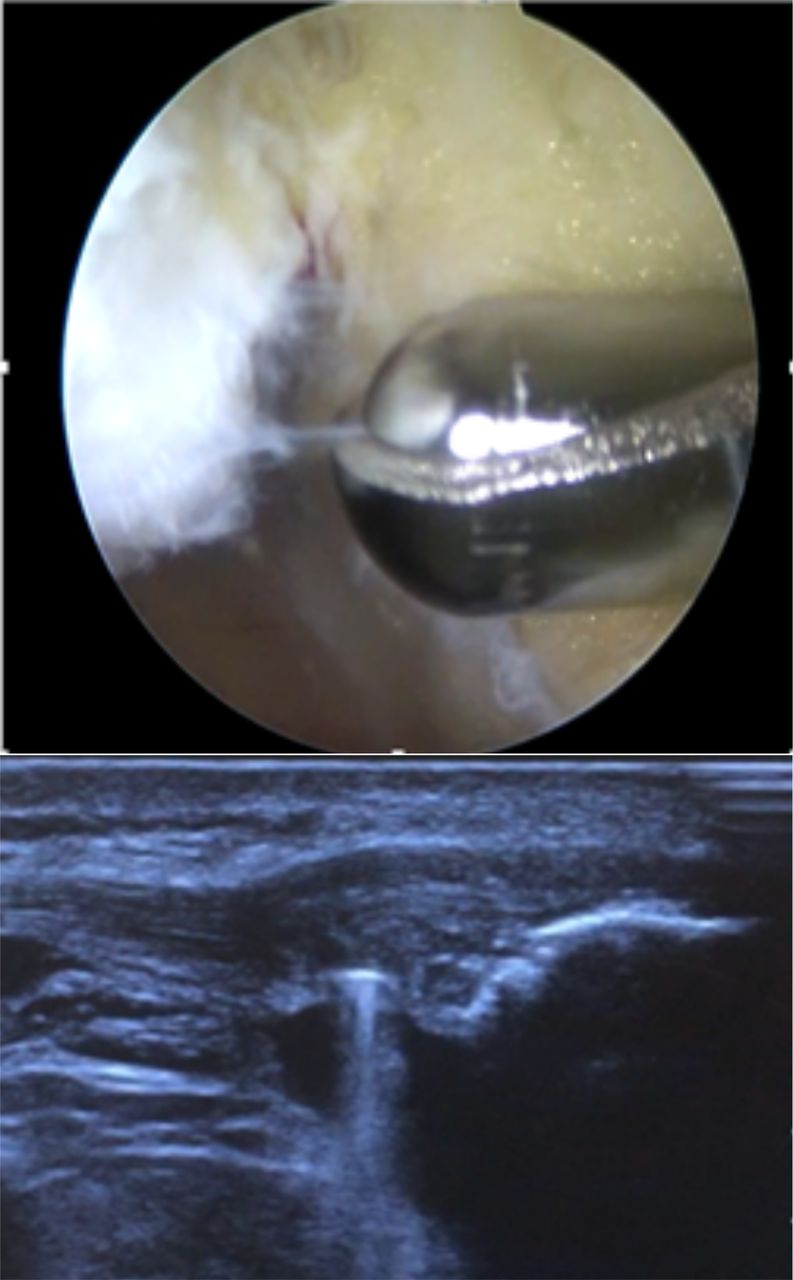
US+CD-guided arthroscopic tendon debridement was performed with general (n=5) or local anaesthesia (n=18). Participants were supine with extended knee. Standard anteromedial and anterolateral portals, pressure-controlled pump and no tourniquet were used. A routine arthroscopic evaluation of the knee joint was performed. Simultaneous US examination (longitudinal and transverse views) guided the procedure (figure 2). Careful debridement was performed using a 4.5 mm full radius blade shaver, aiming to remove vessels and nerves adjacent to the tendinopathic change on the deep side of the tendon (separating Hoffa’s fat pad from the patellar tendon) (figure 3). This technique is based on previous biopsy studies showing sensory and sympathetic nerves located close to blood vessels.21 23

Surgical patellar tendon debridement procedure using ultrasound guidance.

Arthroscopic patellar tendon debridement using ultrasound guidance.
If coexisting pathology was present such as bony spur or calcification at the inferior pole of the patella, careful excision using a shaver was performed. In these cases, it was necessary to also remove some tendinopathic tissue, but emphasis was placed on removal of less tendon tissue. The portals were sutured and 20 mL of local anaesthetic (Levobupivacaine 2.5 mg/mL) was injected into the knee joint.
Subsequently, the superficial part of the surgery was performed. The decision to perform a superficial scraping was based on focal superficial tendon tenderness on palpation together with abnormal US findings on the superficial aspect of the proximal patellar tendon. Via a vertical longitudinal incision in the skin and bursa, the locally thickened paratenon was visualised (see figure 1). The richly vascularised fatty infiltration located under the paratenon on the superficial side of the tendon was carefully excised until normal underlying tendon tissue was visualised. Careful haemostasis was achieved. Resorbable sutures were used subcutaneously, and non-resorbable sutures were used for the skin. Local compression was applied.
Participants rested overnight and allowed to partially weight-bear with crutches. All participants were reviewed the next day. If a knee joint effusion was present, an aspiration was performed under US-guidance using strict sterile conditions. In the absence of any postoperative complications such as a major superficial haematoma, rehabilitation was started using a specific postoperative rehabilitation plan (table 1). The general rehabilitation principles were derived from an expert consensus statement on rehabilitation of patellar tendinopathy,7 but there was often a need to individualise the programme dependent on the functional requirements of the participants. Sutures were removed at 3 weeks. All participants were reviewed at 6 months with clinical assessment and collection of VISA-P and UTC results.
Postoperative rehabilitation principles
Outcome measures
The primary outcome measure was the VISA-P, to evaluate the clinical outcome.34 This was completed independently by the participant, in the absence of guidance from the treating clinician, at both baseline (preoperative) and 6 months (postoperative).
The secondary outcome measure was tendon structure determined using UTC, measured by a single investigator (LM) at baseline and at 6 months.
Participants were instructed to report adverse events to a single investigator (LM).
All participants provided informed written consent for inclusion in the study.
Statistical analysis
Statistical testing was completed using Microsoft Excel for MacOS (Microsoft, Albuquerque, New Mexico, USA). Mean differences and associated 95% CIs were calculated for all variables to reflect postoperative outcomes. In addition, a Cohen’s d was calculated to determine the size of identified interactions, interpreted as small (<0.2), moderate (>0.5) and large (>0.8), respectively.35
Results
Primary outcome (participant function)
VISA-P scores increased from 40.0 (±21.0) at baseline to 82.0 (±15.0) at 6-month follow-up (MD=42.0, d=2.4, 95% CI 32 to 53). In addition, 21/23 participants returned to their prediagnosis activity levels.
Secondary outcome (tendon structure)
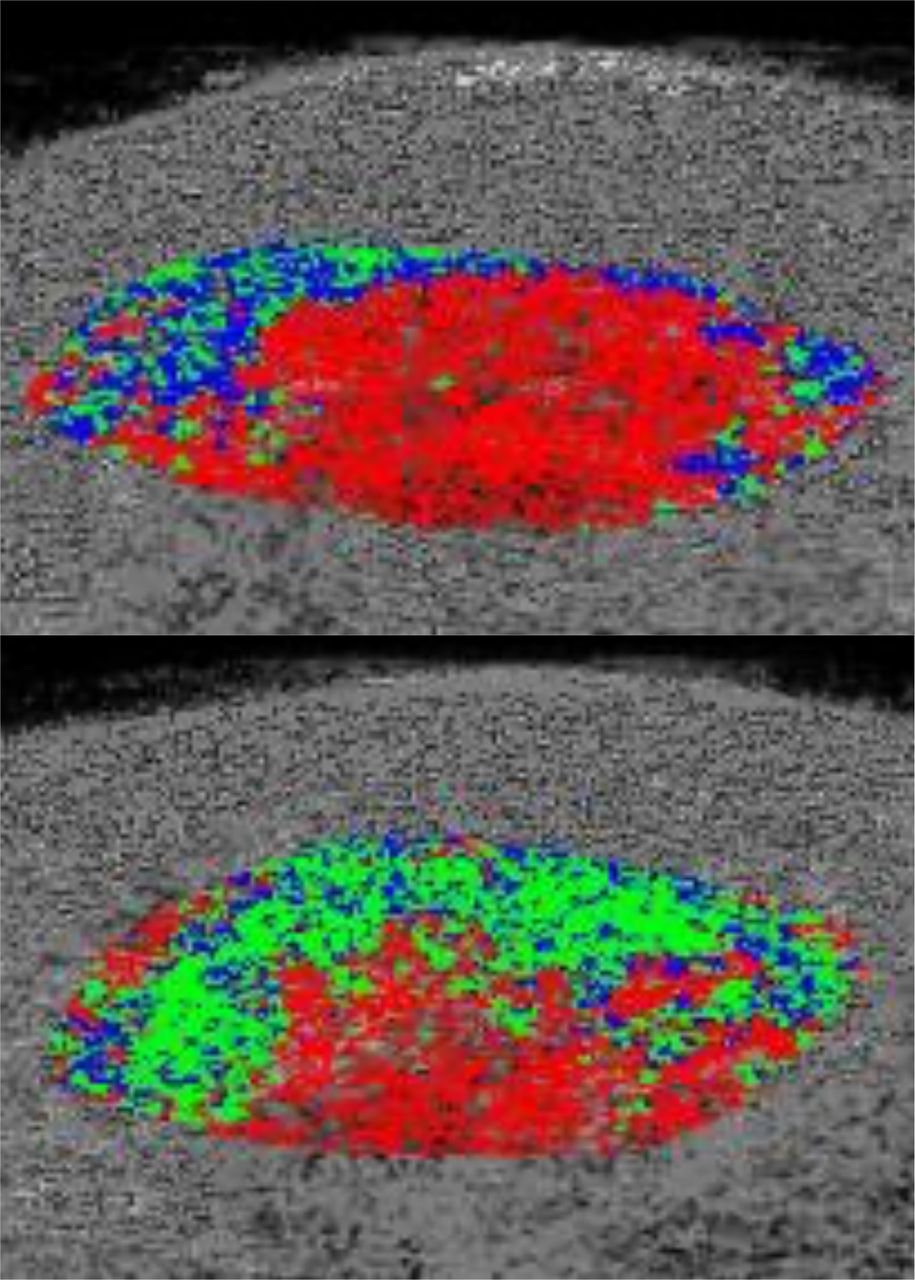
Organised echo pixels (type I+II) increased from 55.0% (±17.0) at baseline to 69.0% (±15.0) at 6-month follow-up (MD=14.0%, d=0.7, 95% CI 2 to 21) (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pre-UTC (above) and post-UTC (below) findings confirming increased organised (green) tissue postdebridement. UTC, ultrasound tissue characterisation.
Adverse events
There was one knee joint effusion, presenting 1 day after the procedure. This hemarthrosis was aspirated under US guidance. There were no serious adverse events.
Discussion
This case series demonstrated that US-guided patellar tendon debridement for recalcitrant patellar tendinopathy improves pain, function and tendon structure at 6-month follow-up. A majority (21/23) of the participants returned to prediagnosis activity levels.
The most interesting finding in this study was the significantly improved tendon structure at 6 months after surgery. To the best of our knowledge, this finding has never previously been demonstrated after surgical patellar tendinopathy treatment. The relationship between tendon structure and symptoms is controversial, particularly in relation to changes that occur following treatment. Some studies, using US and MRI, have reported no relationship between improvements in clinical symptoms and structural change.31 A more recent systematic review including more reliable imaging techniques such as UTC found that there was an association between improvement in clinical symptoms and reduction in tendon thickness and neovascularisation.36 The current study used UTC to define changes in aligned fibrillar structure 6 months after surgery and demonstrated significant improvement after arthroscopic patellar tendon debridement. Recent studies have shown that scanning of the patellar tendon in a similar position demonstrates good intrarater and inter-rater reliability, and intrarater minimal detectable change is estimated to be 5.5%.37
The cause for the improvement in tendon structure is unknown but could be directly related to this surgical technique. This debridement surgery uses US and CD to detect peritendinous regions with high blood flow. Seminal studies assessing biopsies from patellar tendinopathy tissue detected abnormal sensory and sympathetic neural infiltration in close relation to blood vessels in the peritendinous regions.21 23 Removing this abnormal neural ingrowth through US-guided tendon debridement could reduce pain and allow for more aggressive rehab with improvement in symptoms and structure. Alternatively, the positive effects of this surgery could be attributable to indirect effects of enforced rest and progressive rehab that would not have occurred if surgery had not been performed. Further studies using a reliable and quantifiable imaging modality, preferably with randomisation and an exercise control group, are required for more definitive conclusions to be drawn about the cause of structural improvement in this type of tendon surgery.
This surgical procedure is primarily extratendinous and differs substantially from more traditional intratendinous surgical techniques.16 38 There are several advantages in using an extratendinous technique, the most important being that it allows for early full weight-bearing loading of the tendon. It could be argued that a randomised study comparing the US-guided arthroscopic debridement method with the traditional intratendinous revision surgery should be performed. However, this may raise issues since the results after intratendinous revision surgery has been shown to be poor and no better than non-operative treatment with eccentric training.16
The US+CD-guided arthroscopic debridement is the main surgical procedure during this treatment, but we also did a minor superficial debridement procedure. The justification for this superficial procedure is based on our findings that many subjects with longstanding symptoms have focal tenderness corresponding to US findings of localised thickening of the paratenon on the superficial surface of the proximal patellar tendon. Biopsies performed by our group (unpublished data) from this superficial tissue reveal richly vascularised fatty infiltration containing abnormal sensory and sympathetic nerves, which is similar innervation to the tissue on the deep aspect of the proximal patellar tendon.23 Therefore, it seems appropriate to excise this tissue. However, the importance of this procedure to optimise clinical outcome should be evaluated in a randomised controlled trial.
This is a short-term follow-up study, but the positive clinical outcomes demonstrated with this method are not surprising since they are in keeping with results of a previous randomised controlled trial and a 4-year follow-up study19 25 26 on this procedure. In addition, this method appears to be safe.
A limitation of this study is the lack of a control group of enforced rest or exercise therapy. Therefore, the changes in pain, function and structure cannot be directly attributable to the surgical procedure but may be related to the indirect effects of surgery or natural history. However, as the majority of participants in this study had long duration of symptoms and reduced function unresponsive to loading regimens, it seems unlikely that the changes are entirely attributable to natural history.
Conclusion
US-guided patellar tendon debridement for persistent patellar tendinopathy improved symptoms and tendon structure without complications at 6-month follow-up. A majority (21/23) of the patients returned to their preinjury activity level. Further studies with longer follow-ups, preferably randomised and controlled, are needed.
References
Footnotes
Twitter @lorenzo_masci
Contributors LM was the main researcher and primary author. HA contributed to the research and writing of the paper. BN contributed to the statistics and writing of the paper. WWB was involved in data collection.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Obtained.
Ethics approval Ethical approval was granted by the Umea University, Umea Sweden (Dnr 04-157 M).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Deidentified clinical and UTC data will be available from first author on reasonable request via email lorenzo@sportdoctorlondon.com.