Article Text

Abstract
Background/Aim This study aimed to quantify breast skin strain and strain rate and the effect of support garments at reducing strain and to determine characteristics that correlate with strain during static and dynamic activity.
Methods 39 women (UK size 32C to 36G) had electromagnetic sensors applied to their breast skin. Sensor coordinates were recorded while standing, walking, running, in no, low and high breast support conditions, plus bare-breasted in the estimated neutral position to calculate strain. Relative breast coordinates and 35 inter-sensor distances identified peak breast skin strain (%) and strain rate (%·s-1), which were then correlated with nipple kinematics, breast pain and participant characteristics.
Results Mean peak breast skin strain was generally <60% during standing, walking and running; however, some individuals exhibited 93% strain in bare-breasted running. Compared with low support, high support did not further reduce strain during standing and walking. Peak breast skin strain/strain rate location was longitudinal, in lateral and medial breast regions and displayed strong correlations with breast volume, body mass index and bust circumference.
Conclusion Static and dynamic activity did not result in excessive breast skin strain, suggesting low risk of skin damage. However, during running, some individuals experienced excessive skin strains (up to 93%) and strain rates (up to 1258%·s-1). Breast skin strain/strain rate location suggests lift is required in the lateral and medial bra cup to reduce strain, particularly in larger breast volumes due to increased skin strain risk.
- breast
- biomechanics
- exercise
- women
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings
Generally, women do not experience damaging peak breast skin strains (>60%) during standing, walking and running, regardless of breast support level. However, some individuals may exhibit damaging breast skin strains of up to 93% strain during bare-breasted running.
Lateral and medial breast regions are more susceptible to peak breast skin strain and strain rates, with these commonly occurring longitudinally.
Women with greater breast volumes, body mass indices and bust circumferences may be more susceptible to damaging their breast skin due to increased peak breast skin strains and strain rates.
Introduction
The unsupported breast moves independently during dynamic activities.1–3 This independent movement is thought to be driven by torso displacement4 5 and occurs due to limited anatomical support within the breast.4 This limited supported is provided by Cooper’s ligaments and breast skin.6 Previous research has reported that the bare breast is vertically displaced ~4 cm during walking7 8 and up to 10 cm during running.1–3 8 9 While external breast support garments decrease movement (~6 cm decrease in vertical displacement during running),10 movement-related breast pain is still common during exercise in inadequate support garments.4 9 11 12
The aetiology of movement-related breast pain is unclear, but associations with strain on breast support structures have been suggested.9 13 When measuring strain, assessment of the Cooper’s ligaments during dynamic activity may not always be possible due to their internal location.14 15 However, the measurement of breast skin strain is important as breast ptosis (sag) may be related to mechanical strain on breast skin, with mechanical failure of skin possibly manifesting in stretch marks (striae distensae).16 17
Measuring strain in the body determines the magnitude and reversibility of biological tissue’s response to external loading.18–22 Skin displays a non-linear, time-dependent stress–strain relationship.23 24 Skin’s stress–strain curve is divided into four phases25: phase 1 (<30% skin strain), straightening of collagen fibres; phases 2 and 3 (30% and 60% skin strain), realignment of fibres in the direction of stress, collagen begins to resist deformation; phase 4 (>60% skin strain), collagen fibres begin to fracture.25 26 It is this collagen failure (occurring due to defibrillation) that signifies skin damage.27
In healthy breast skin samples, Kumaraswamy et al28 identified up to 58% strain without fibril damage. However, strain assessment was performed in vitro using a testing rig restricted to 58% strain. It is therefore unknown if an increase in strain above 58% would result in skin damage. Haake and Scurr29 and Haake et al30 investigated breast skin strain in vivo during bare-breasted running reporting strains of up to ~120%. However, strain was calculated uniaxially, between the sternal notch and nipple, rather than across the breast surface. Sanchez et al31 used an 18-marker array across the breast surface to identify breast skin strain during standing. Breast skin strain of 75% in longitudinal superior and lateral breast regions were reported, providing data on strain magnitudes, locations and directions.31 While this study advanced in-vivo breast skin strain measurement, marker coordinates on the bare breast were recorded by motion capture cameras which could not determine skin strain inside a bra.
The limited studies that measure breast skin strain have focused on strain magnitude; strain rate has yet to be considered in vivo despite associations between skin strain rate, ultimate tensile strength of skin and pain sensation.32 33 Using pig skin, which displays similar mechanics to human skin,34 Liu et al33 reported reduced pain at low skin strain rates, but sharp increases in pain as strain rate increased.33 Therefore, understanding relationships between breast skin strain rate and pain may aid our understanding of breast pain.
The aims of this study are as follows:
To quantify bare-breasted skin strain magnitude and rates during static and dynamic activity.
To identify the effects of breast support garments on breast skin strain, rates and locations of peaks.
To investigate the relationships of breast skin strain/strain rates with nipple kinematics, breast pain and participant characteristics.
Methods
Study population and study protocol
Following institutional ethical approval, 39 women gave written informed consent to participate. However, participants were not involved in the study design, reporting or dissemination of this research. Participants were (mean and range) aged 25 years (19–38 years) with a body mass of 66 kg (52–95 kg), nulliparous, had not undergone breast surgery and had not experienced >15 min of ultraviolet radiation to the breasts in the last 3 months.35 Participants had their bra size assessed by a trained bra fitter, using best-fit criteria36 (mode 34B (range 32C to 36G)), and their underband (mean 80 cm, (range 70–93 cm)) and bust circumference (mean 94 cm, (range 84–109 cm)) measurements were recorded. A 6 s bare-breasted torso surface scan estimated left breast volume (3D scanner, SizeStream, V.5.2.3) using SizeStream Studio software (V.5.2.3), giving a mean of 728 mL (range 226–1506 mL)).37
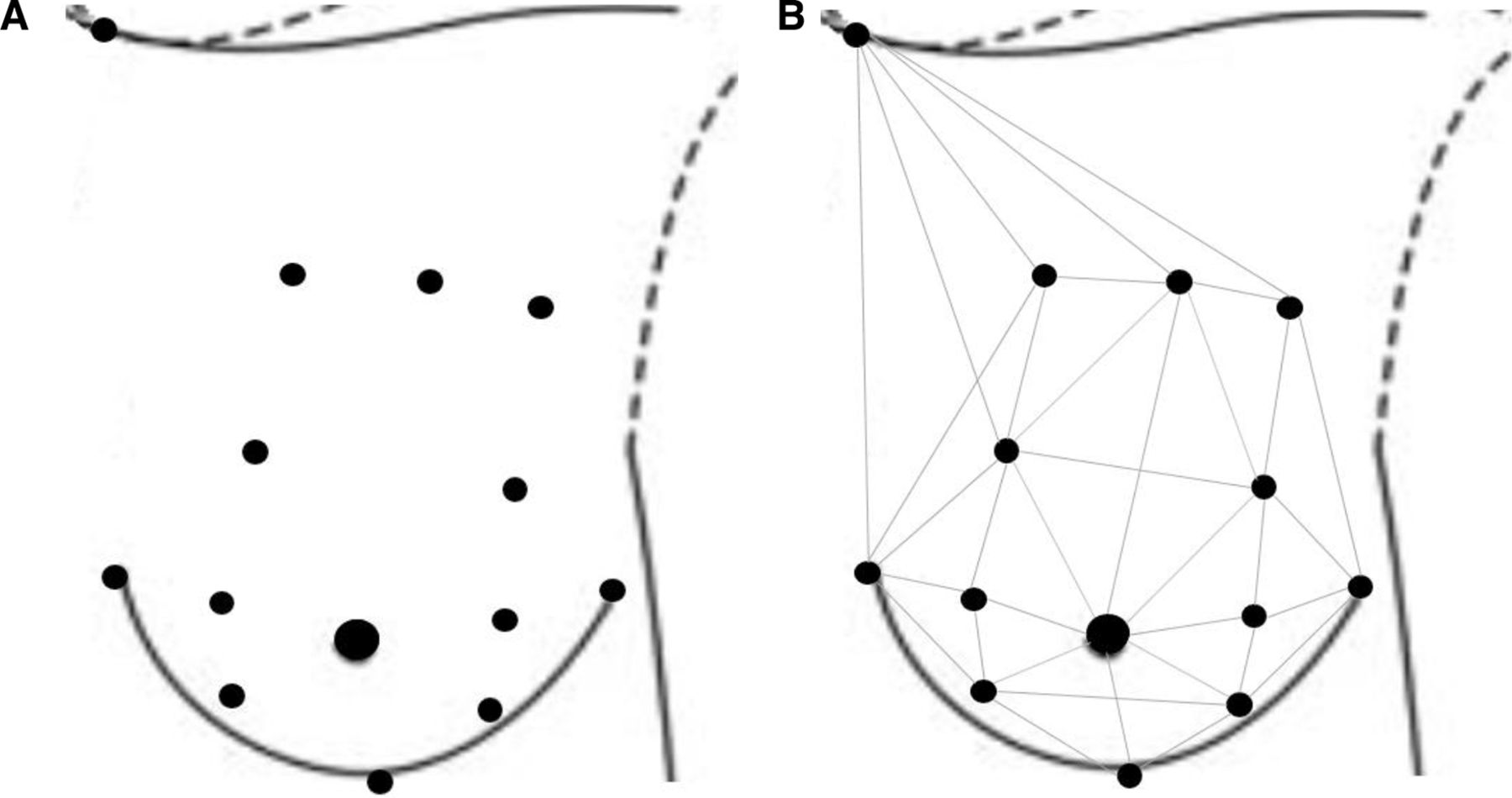
Breast and torso positional data were recorded using an electromagnetic (240 Hz, Liberty, Polhemus, USA) 14-sensor array (mass <1 g) covering participants’ left breast, based on rectangular breast segmentation38 (figure 1A).39 Two additional sensors on C7 and T8 quantified breast motion relative to the torso.40

(A) The 14-sensor array (black circles) used to measure breast position. (B) The 35 strain lines identified utilising this array.39
Static sensor coordinates were recorded for 10 s with the participant in the anatomical position. Following a warm up, dynamic sensor coordinates were recorded during treadmill (h/p/cosmos mercury, Nussdorf–Traunstein, Germany) walking (1.4 m·s-1, 5.0 km·h-1)7 and running (2.8 m·s-1, 10.0 km·h-1)7 for 30 s.41 Participants performed standing, walking and running in three breast support conditions, no support (bare-breasted), low support (an everyday bra used in previous research8): Marks & Spencer T-shirt bra, 92% cotton, 8% elastane lycra) and high support (a sports bra similar to that used in previous research42); Shock Absorber Run Bra, 81% polyamide, 10% polyester, 9% elastane). Following walking and running, participants rated their breast pain from ‘no pain’ 0 to ‘worst pain possible’ 10, on a 10 cm Visual Analogue Scale.43 44 Order of the bra conditions was randomised; however, the no support condition was performed last to prevent residual breast pain from bare-breasted running effecting breast pain scores.
Strain calculation requires the determination of a neutral position (zero strain). The neutral breast position was estimated following the Mills et al45 methods. Briefly, participants were submerged in water, in an upright, stationary position and sensor coordinates recorded for 10 s. While Mills et al45 used soybean oil and water immersion to estimate the neutral position, water alone identified the neutral position to within 5.6 mm.
Strain, strain rate and nipple kinematics calculation
Sensor coordinates were exported to Visual 3D (V.4.96.4, C-motion) and filtered (generalised cross-validatory quintic spline).31 A reference torso segment was created, with the proximal end (origin) midway between suprasternal notch and C7 sensors, and the distal end midway between xiphoid process and T8 sensors.40 Thirty-five inter-sensor distances were calculated for each participant, in each condition (water immersion, standing, walking and running) (figure 1B).
Static and dynamic breast skin strains were then calculated using
 (1)
(1)
 (2)
(2)
and instantaneous dynamic breast skin strain rates,
 (3)
(3)
where L was the inter-sensor distance during any activity at each time point, L0 was the mean inter-sensor distance during water immersion (10 s) and t was time.
Walking and running gait cycles were identified using every other minima in the vertical suprasternal notch coordinates, and 20 gait cycles were analysed.46 Maximum breast skin strain and strain rate, for each strain line, were identified in each gait cycle. The mean maxima was identified for 20 gait cycles and the maximum values across any strain line were selected for each participant (peak strain). Nipple kinematics (range of motion (ROM) (m), peak velocity (m·s-1) and peak acceleration (m·s-2)) were calculated relative to the torso coordinate system,47 within the same gait cycles.
Statistical analyses
Using SPSS (V.24), data were checked for normality; 86 out of 111 variables that were not normally distributed (Shapiro-Wilk, p<0.05) were compared across no, low and high breast support conditions using Friedman tests, followed by Wilcoxon tests. Where variables were normally distributed (25 variables), data were compared using one-way repeated measures analysis of variance, followed by pairwise post hoc tests with a Bonferroni corrected significance level of p=0.0167. Effect sizes were also identified (parametric: d, non-parametric: r) (weak <0.3, moderate 0.3–0.5, strong >0.5).48 To investigate relationships of peak breast skin strain/strain rate with nipple kinematics, breast pain and participant characteristics, Pearson’s correlations (r) were calculated; trivial (<0.3), low (0.3–0.5), moderate (0.5–0.7), high (0.7–0.9) and very high (>0.9).49 Prior to conducting the correlation analysis, all peak velocities and accelerations were converted to positive values to ensure positive and negative relationships could be identified.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Results
Bare-breasted skin strain magnitudes and rates
Bare-breasted peak breast skin strain significantly increased from standing (31%) to walking (36%) to running (46%), with all activities displaying mean peak breast skin strain below the potentially damaging threshold of 60% (table 1 and online supplementary table 1). However, three participants experienced breast skin strain of greater than 60% during standing (62%, 72% and 74%) and walking (70%,70% and 72%), while seven participants experienced breast skin strain of greater than 60% during running (61%–93%). While peak breast skin strain displayed a moderate increase from walking (36%) to running (46%), peak breast skin strain rate increased greater than fourfold from walking (131%·s-1) to running (610%·s-1).
Supplemental material
Mean (and range) peak breast skin strain (%) and peak breast skin strain rate (%·s-1) during standing, walking (1.4 m∙s-1) and running (2.8 m∙s-1) with no breast support, low support and high support, and effect sizes (d or r) across breast support conditions (n=39, breast size range of 32C to 36G)
Effects of breast support on skin strain/strain rate
Compared with no support, low and high breast support significantly reduced peak breast skin strain across all activities (table 1). However, in low support, one participant displayed peak breast skin strain of 62% during running. In comparison, in high support, no peak breast skin strains greater than 60% were identified. Low and high breast support also significantly reduced peak breast skin strain rate, compared with no support, with strong effect sizes. The greatest mean peak breast skin strain rate identified was 610%·s-1 during running in no support, which was almost three times that displayed when running in high breast support (237%·s-1).
Breast skin strain profiles
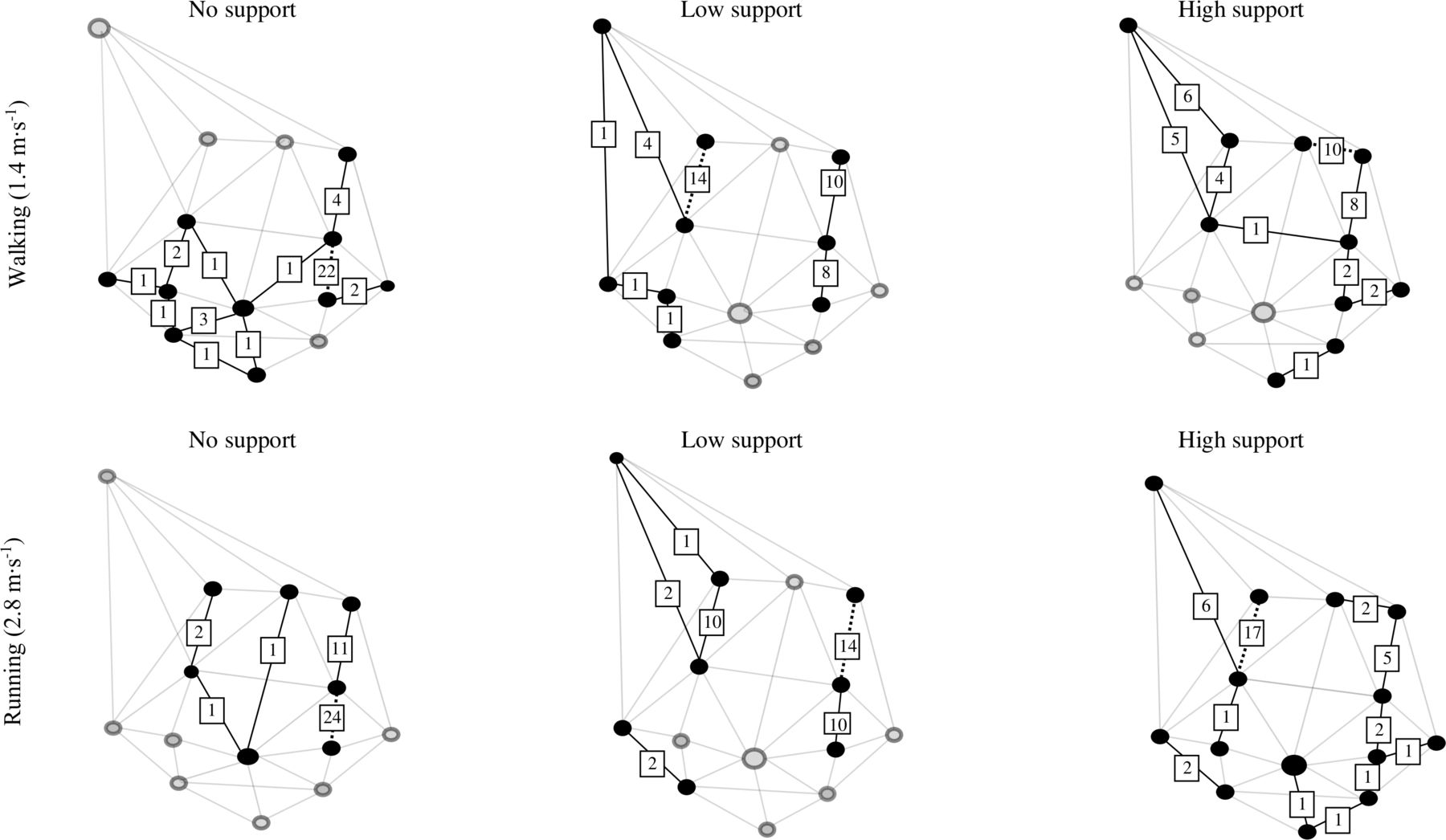
An increase in breast support resulted in a more diverse distribution of peak strain across the breast (figure 2). The number of participants with a similar location for peak breast skin strain decreased from 20 (no support) to 10 (low support) to 6 (high support) in standing, and 16 (no support) to 8 (low support) to 5 (high support) in walking. In running, the distribution of peak breast skin strain was relatively similar for no support and low support, with most participants displaying peak strain in the lateral breast region.

The number of participants who experienced peak breast skin strain in this location, during standing, walking (1.4 m∙s-1) and running (2.8 m∙s-1) in no support, low support and high support conditions (n=39, breast size range of 32C to 36G). The peak breast skin strain line(s) most prevalent across participants is indicated by a dotted line.
Peak breast skin strain rate profiles were more homogeneous than the strain profiles, with the majority of participants experiencing peak breast skin strain rate in one location; upper, lateral breast region (figure 3). An increase in breast support during running reduced the number of participants experiencing peak strain rates in the upper, lateral breast region (35 participants in no support and 24 participants in low support). In high support during running, 66% of participants (26 out of 39 participants) experienced peak strain rates in the medial breast region, suggesting a medial shift in peak breast skin strain rates as these breast support conditions increased.
{kind=link}
{kind=link}
{kind=link}
The location of peak breast skin strain rates and the number of participants who experienced peak breast skin strain rates in this location, during walking (1.4 m∙s-1) and running (2.8 m∙s-1) in no support, low support and high support conditions (n=39, breast size range of 32C to 36G). The peak breast skin strain rate line(s) most prevalent across participants is indicated by a dotted line.
Relationships of breast skin strain/strain rate with nipple kinematics, breast pain and participant characteristics
Increased breast support resulted in significant reductions in nipple ROM, velocity and acceleration, in all directions, during both walking and running (table 2), with mostly strong effect sizes (d or r>0.5). As breast support increased, breast pain significantly decreased from 0.75 to 0.37 to 0.13 (out of 10) during walking and from 4.49 to 2.39 to 0.26 during running, with moderate to strong effect sizes.
Mean (SD) nipple range of motion (m), peak nipple velocity (m·s-1), peak nipple acceleration (m·s-2) and breast pain (0 to 10) during walking (1.4 m∙s-1) and running (2.8 m∙s-1) with no breast support, low support and high support, and effect sizes (d or r) across breast support conditions (n=39, breast size range of 32C to 36G)
When examining the relationships of peak breast skin strain/strain rates with nipple kinematics (table 3), the no support condition demonstrated stronger relationships between strain/strain rate and kinematics and, in general, these relationships reduced as support increased. Compared with walking, running generally displayed stronger relationships between strain/strain rate and nipple kinematics; however, anteroposterior nipple ROM during walking with no support displayed the strongest relationship to peak strain (r=0.723), while inferior peak nipple acceleration during running displayed the strongest relationship to peak strain rate (r=0.891). Breast pain displayed weak correlations (r<0.5) with breast skin strain and strain rate. When examining the relationship of peak breast skin strain/strain rates with participant’s physical characteristics, breast volume, body mass index (BMI) and bust circumference displayed moderate to high correlations with strain. Breast volume displayed the strongest correlations (for participant characteristics) to both peak breast skin strain (r=0.672) and strain rate (r=0.705).
Pearson’s correlations (r) between peak breast skin strain (%) and peak breast skin strain rate (%·s-1) and nipple kinematics, breast pain and participant characteristics, during standing, walking and running (2.8 m∙s-1) (n=39, breast size range of 32C to 36G)
Discussion
During static and dynamic activity, this study established bare-breasted skin strain magnitudes and rates, the effect of breast support on strain magnitudes and rates, and where peak strains occurred. Additionally, this study identified the relationships of breast skin strain magnitudes and rates with nipple kinematics, breast pain and participant characteristics.
Breast support levels and peak breast skin strain/strain rate
The results showed peak bare-breasted skin strain during standing ranged from 14% to 74% across participants, similar to values reported by Sanchez et al31 (14%–75%). No conclusive skin strain damage threshold exists, and the 60% value reported by Silver et al26 was derived from in-vitro torso and abdomen skin, suggesting caution when applying this threshold to in-vivo breast skin strain assessment. Nevertheless, despite mean peak breast skin strain remaining below 60% across activities (suggesting low risk of skin damage26), at least one participant displayed strain values during standing, walking and running in no support ranging from 73% to 93%, and 62% during running in low support.
Similar to Haake and Scurr,29 peak breast skin strain significantly decreased when running in high support compared with low support. Interestingly, this was not observed during standing and walking; this may be due to the lower intensities of these activities (walking <5 METs50), and reduced ROM.7 9 In walking, the low support garment constrained breast skin strain to similar levels as the static condition. Peak breast skin strain rate also significantly decreased when running in high support compared with low support. An increase in skin strain rate has been associated with increased skin stiffness,51 which is a prominent factor in soft tissue failure.52 The use of breast support during running may therefore decrease participants’ risk of breast skin damage due to decreased breast skin strain rates.51
Peak breast skin strain in no support was commonly observed longitudinally, in the superior, lateral breast region, similar to Sanchez et al.30 While Zhou et al53 identified the medial, lateral and inferior regions of the breast moved more than the superior region of the breast during bare-breasted running, the current study suggests increased breast support is needed to lift the superior, lateral region of the breast, reducing strain in this region. It must be noted that while peak strain occurs at these locations, they will also achieve their maximum at different instances in time during each gait cycle. Across participants, external breast support resulted in an increased number of locations where peak breast skin strain occurred, suggesting a redistribution of strain which varied across participants. This may be related to the manual positioning of breast tissue inside the bra, which could vary during each bra application and from woman to woman.
Peak breast skin strain rate was also commonly identified longitudinally in the superior breast region, however, in both medial and lateral breast regions. This is supported by the breast Langer lines,54 which represent collagen fibre orientation in the skin.55 As maximum skin extensibility occurs at right angles to Langer lines,54 the most prevalent locations of peak breast skin strain rates within this study (longitudinally in medial and lateral breast regions) may occur at maximum skin extensibility.
Relationships between variables
All nipple kinematics displayed moderate or high correlations (r>0.5) with peak breast skin strain rate during bare-breasted running. This was interesting but not surprising, as peak breast skin strain rate was not commonly identified on a strain line connected to the nipple, but these results are based on mechanical principles. Further investigation is required to identify whether nipple kinematics could predict breast skin strain magnitudes and rates. Despite previous research reporting associations between skin strain and pain,56–60 only weak relationships were observed in this study. This is an important finding from a participant perspective as this suggests that although breast skin strain may not be related to pain, it may still be relevant to skin damage and breast ptosis.16 17 However, the subjectivity of pain ratings, large SD across participants and very low breast pain ratings during walking (<0.75 out of 10) question the sensitivity of the pain scoring system. Considering participant characteristics, breast volume, BMI and bust circumference displayed the strongest and most prevalent relationships with peak breast skin strain/strain rate. This may in part support Sanchez et al31 who reported that larger breasted women (>34D) displayed increased static breast skin strain (compared with smaller-breasted women). Willson et al61 identified that breast skin thickness decreased with increased breast size, and thinner skin may be more distensible than thicker skin,62 suggesting that women with larger breast volumes may be more susceptible to higher breast skin strain.
Strengths and limitations
This was the first study to consider breast skin strain rates in vivo. Breast skin strain rate appears to be a valuable measure; when compared with breast skin strain magnitude, strain rate demonstrates consistent differentiation between breast support conditions and activity levels, a more consistent pattern in strain rate location and stronger correlations with nipple kinematics. However, this study is also not without its limitations. While the walking and running speeds of participants were controlled, previous research has identified that individual running styles contribute to breast movement,63 with females adopting mechanical alterations to their gait64 and trunk displacement65 dependent on breast support levels. Future research into breast skin strain/strain rates should incorporate whole-body kinematic and kinetic analysis which may provide further insight.
Conclusion
This novel study investigated breast skin strain magnitudes and rates during static and dynamic activity. For most participants, breast skin strain was below 60% during standing, walking and running, suggesting reduced risk of breast skin damage. However, during running, one participant exhibited skin strains up to 93% in no support and 62% in low support, coupled with increased strain rates suggesting an increased risk of breast skin damage is possible for some women. Interestingly, when compared with low support, high support did not further reduce breast skin strain during standing and walking, questioning the need for high support during these activities. The location of breast skin strain/strain rate was longitudinal, in the lateral and medial strain lines, suggesting lift is required in these regions to reduce breast skin strain risk. Contrary to previous literature, only weak correlations were observed between breast skin strain/strain rates and breast pain, suggesting that, although breast skin strain may not be related to pain, it may still be relevant to skin damage. Breast skin strain/strain rates were correlated with breast volume, suggesting that women with larger breast volumes may be more susceptible to breast skin strain.
Acknowledgments
The authors declare that the results of this study are presented clearly, honestly and without fabrication, falsification or inappropriate data manipulation.
References
Footnotes
Contributors All coauthors are in agreement to be accountable for the work presented in this manuscript. All authors were involved in the conception and design of this study and the interpretation of data. MN was responsible for initial writing and drafting of the manuscript, which was reviewed by all authors. All authors approved the final version to be submitted.
Funding This work was supported, in part, by the Science Foundation Ireland grant 13/RC/2094 and has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No. 754489. MN and AS have also received funding for the current study from Hanes Brands. For the remaining authors, none were declared. The results of the present study do not constitute endorsement by ACSM.
Competing interests This work was supported, in part, by the Science Foundation Ireland grant 13/RC/2094 and has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No. 754489. MN and AS have also received funding for the current study from Hanes Brands. For the remaining authors, none were declared. The results of the present study do not constitute endorsement by ACSM.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.