Article Text

Abstract
Objectives (1) To describe the cardiorespiratory fitness (CRF) in an adult cystic fibrosis population related to sex and age, (2) to evaluate the cause of low CRF and (3) to study the association between peak oxygen uptake (VO2peak) and forced expiratory volume in 1 s (FEV1).
Methods A total of 204 cardiopulmonary treadmill exercise tests (CPETs) performed by 116 patients were included. VO2peak, gas exchange, heart rate, oxygen saturation and ventilatory variables were measured.
A low CRF was defined as a VO2peak <80% of predicted, ventilatory limitation was defined as a breathing reserve <15%, exercise hypoxaemia was defined as an oxygen saturation <88% and ventilation-perfusion mismatch was defined as a minute ventilation/ventilatory equivalent for carbon dioxide slope ≥34. In patients who had performed three or more CPETs, the annual change in FEV1 and VO2peak were calculated using linear regression.
Results The VO2peak was 40.6±11.5 and 35.2±8.9 mL kg−1 min−1, which was 87±23 and 93±20 in percentage of predicted for men and women, respectively. VO2peak was moderately affected by age, for men (r=−0.36, p<0.001) and women (r=−0.53, p<0.001), respectively. In 45 of 101 tests where CRF was low, no cardiorespiratory limiting factors were identified. The correlation coefficient between VO2peak and FEV1 was r=0.64 (p<0.001). In participants with a low CRF, FEV1 ranged from 20% to 112% of predicted.
Conclusions The correlation between VO2peak and FEV1 was moderate. The majority of the tests resulted in a VO2peak within normal limits. Interestingly, 44% of the tests with a low VO2peak could be explained by deconditioning. Thus, exercise therapy may be beneficial for these patients.
- exercise testing
- pulmonary
- respiratory
- physiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings?
Somewhat surprisingly, two thirds of the tests resulted in a peak oxygen uptake (VO2peak) within the reference limits of the general population.
In almost half of the patients with a low VO2peak, deconditioning seemed to be the cause.
Forced expiratory volume in 1 s (FEV1) could not invariably predict the cystic fibrosis (CF) patients’ cardiorespiratory fitness.
How might it impact on clinical practice in the future?
Cardiopulmonary exercise test provides valuable insight beyond FEV1 in order to identify:
Cardiorespiratory pathophysiology in CF.
Patients that might benefit from exercise therapy.
Introduction
In cystic fibrosis (CF) regular physical activity represents an integral part of disease management,1 and as reduced exercise capacity has been shown to be prognostically disadvantageous, identifying patients in need of exercise counselling seems important.2 Pulmonary disease, eventually progressing to respiratory failure, is the leading cause of death in the CF population. Forced expiratory volume in 1 s (FEV1) is used as the single most important variable to monitor the development and progression of pulmonary disease in patients with CF, and its decline is negatively associated with survival.3–5 Although rising, the life expectancy of patients with CF it is still markedly reduced compared with the general population in the western hemisphere.6
Clinical exercise testing7 is recommended performed annually in the follow-up of patients with CF,8–10 and a standardised cardiopulmonary exercise test (CPET) is the most reliable method for determining cardiorespiratory fitness (CRF) by non-invasively measuring cardiopulmonary response during incremental exercise to maximum effort.7 11 Peak oxygen uptake (VO2peak) is considered the most important variable during CPET and provides valuable information about the cardiorespiratory system, the causes of dyspnoea and the prognosis of the patient.2 12 Desaturation during exercise testing is known to correlate with both accelerated lung function decline and increased likelihood of hospitalisation.13 It has recently been shown that the VO2peak and other CPET derived measures represent independent and significant predictors of death or lung-transplant at 10-year follow-up.2
Several studies have described CRF in the adult CF population.2 14–25 However, most of these studies were based on a limited number of participants,14–16 19–22 or described results in a population below the age of 30 years.14–23 In addition, CPET was conducted using a cycle ergometer2 14–19 21–25 in all but one study.20 Cycle ergometry, which is recommended for individuals with CF aged >10 years, is the preferred method at most CF centres.10 Although not shown in CF, a higher VO2peak is obtained on a treadmill then when using cycle ergometry in both patients with chronic obstructive pulmonary disease and healthy subjects.26 27 To the authors’ knowledge, no previous studies have described CRF and cardiopulmonary response during maximal exercise on a treadmill in a large number of adult patients with CF of varying age.
The objectives of the present study were (1) to describe the CRF determined by treadmill testing in an adult CF population related to sex and age, (2) to evaluate the causes of decreased CRF and (3) to study the association between VO2peak and FEV1 in all individuals and longitudinally in patients having performed three or more tests.
Materials and methods
Participants
CPETs performed between January 2006 and June 2017 were retrospectively included in an internal quality registry database (EpiData software—V.2.0.8.56, The EpiData Association, Odense, Denmark) at the Norwegian Resource Centre for Cystic Fibrosis in Oslo, Norway. CPET is an integrated part of the routine assessment of adult patients with CF . In a minority of the Norwegian CF population, chronic colonisation with Mycobacterium abscessus, Burkholderia sp, methicillin-resistant Staphylococcus aureus or multidrug-resistant Pseudomonas aeruginosa prevented CPET due to hygienic considerations. CPET was not performed during pulmonary exacerbations. No results from lung-transplanted patients were included in the present study for two reasons: (1) in Norway, the pulmonary function of lung-transplanted patients, including CF, is followed life-long by another institution (the national referral centre for lung transplantation, Oslo University Hospital Rikshospitalet) and (2) post-transplant CPET data, although interesting per se, would not benefit the aims of this study. Patients prescribed pancreatic enzyme replacement therapy (PERT) were considered pancreatic insufficient (PI), whereas those not on PERT were considered pancreatic sufficient (PS).
In total, 204 CPETs performed by 116 adult patients, aged 18–68 years, are listed in the database, and thus included in the present study. Fifty-three patients were tested three times or more. Results from patients tested more than once were included if represented in separate age-cohorts. In cases where the patient had several CPETs within the same age-cohort, only the latest was included.
Patient and public involvement
User involvement was provided through The Norwegian Cystic Fibrosis Association representatives to the council for Norwegian Resource Centre for Cystic Fibrosis.
Measurements
Height and body weight were measured to the nearest 0.5 cm and 0.1 kg, respectively, with participants wearing light clothing and no shoes.
Spirometry were conducted (Sensor Medics, Yorba Linda, California, USA) according to the American Thoracic Society/European Respiratory Society guidelines.28 Maximal voluntary ventilation (MVV) was measured by asking the patients to breathe as fast and deep as possible for 12 s in a standing position. In the tests where the patients did not manage the MVV procedure (n=14), FEV1×40 was used as an estimate.
All tests (spirometry and CPET) were performed by the same experienced exercise physiologist, using an incremental protocol of uphill walking and running on a treadmill (Jaeger LE 100, Würzburg, Germany or Woodway, Würzburg, Germany). Prior to each CPET, complete volume and gas calibration was performed, and all patients were familiarised with treadmill walking. After a short warm-up at 3 km hour−1, speed and elevation were increased alternately every minute by 1 km hour−1 and 1% elevation, respectively, until exhaustion. Gas exchange and ventilatory variables were continuously determined by breath-by-breath sampling, averaged over 30 s intervals, through a Hans Rudolph two-way breathing mask (Hans Rudolph, Kansas City, USA). The breathing mask was connected to a Vmax SensorMedics metabolic analyser (Yorba Linda, California, USA) to assess ventilatory variables and the content of oxygen and carbon dioxide of expired air. At rest in a sitting position, during the entire exercise test, and in the recovery phase, percutaneous oxygen saturation (SpO2) was measured with a finger probe using a stationary pulse oximeter (NONIN 8600, Medical, Minneapolis, USA). Maximal heart rate (HRmax) was measured through a 12-lead ECG (Cardiosoft GE Marquette Medical Systems, Milwaukee, Wisconsin, USA). Ratings of perceived exertion (RPE) were recorded throughout the test using the BORG 6–20 scale,29 and the final rating during maximal effort is presented.
Data handling
The predicted spirometry values were calculated using the Global Lung Function Initiative 2012 reference values.30 End criteria used for evaluation of maximal effort were respiratory exchange ratio (RER ≥1.10) or RPE (BORG scale ≥17).31 Predicted VO2peak values were calculated according to Edvardsen et al, which was considered the most suitable reference material, being derived from a large Norwegian population using a treadmill.31
The ventilatory threshold (VT) was calculated using the ventilatory equivalent method,27 and expressed as VO2 (L min−1) and in percentage of VO2peak. The breathing reserve (%) was calculated using the following equation: ((MVV−VE)/MVV)×100, where VE is the maximal minute ventilation. The oxygen pulse was calculated by dividing VO2peak (in mL) by the HRmax. The VE and CO2 responses during exercise were used to calculate the VE/VCO2 slope, where we excluded the values after the respiratory compensation point.32
A low CRF was defined as a VO2peak <80% of predicted,9 ventilatory limitation was defined as a breathing reserve <15%, exercise hypoxaemia at maximal effort was defined as a SpO2 <88% and signs of ventilation perfusion (VQ) mismatch (gas exchange limitation) was defined as a VE/VCO2 slope ≥34.
Statistical analysis
Results are presented as mean±SD for continuous data and median and range for not normally distributed data. Cross-sectional data are reported by gender and age groups (5-year age cohorts). Analysis of variance (ANOVA) was used to evaluate differences in the cardiopulmonary variables between age cohorts tested by linear trends. Differences between groups based on exocrine pancreas status, RER and gender were tested with the Student’s t-test. Correlations between VO2peak, age, FEV1 and annual changes in FEV1 and VO2peak were assessed by Pearson’s correlation coefficient. In patients who had performed three or more CPETs, the annual change in FEV1 and VO2peak was calculated using linear regression. Statistical significance level was set to ≤0.05. Data were analysed using IBM SPSS Statistical Data Editor, V.24.0.
Results
Sixty-nine men (aged 18–68 years) and 47 women (aged 18–65 years) performed 204 CPETs using a treadmill until exhaustion, and no adverse events were observed. One hundred and fifty-two CPETs (75%) were performed by the patients with PI.
Baseline characteristics, spirometry and MVV values are listed in tables 1 and 2 for men and women, respectively. FEV1 was significantly lower in patients with PI compared with PS (64% vs 80% of predicted; p<0.001).
Baseline characteristics, spirometry and maximal voluntary ventilation (MVV) values for men; all and divided by 5-year age cohorts
Baseline characteristics, spirometry and maximal voluntary ventilation (MVV) values for women; all and divided by 5-year age cohorts
Tables 3 and 4 show the physiological variables of cardiopulmonary response during CPET, including end-criteria RER and RPE for men and women, respectively. RER and RPE were high throughout all age cohorts for both genders, indicating excellent effort during CPET. In the 34 tests (17%) in which the RER ≥1.10 criterion was not achieved, both FEV1 and VO2peak were significantly lower as compared with the tests that reached RER ≥1.10 (44% vs 73% of predicted (p<0.001) and 69% vs 91% of predicted (p<0.001), respectively).
Cardiopulmonary response during exercise on a treadmill for men; all and divided by 5-year age cohorts
Cardiopulmonary response during exercise on a treadmill for women; all and divided by 5-year age cohorts
VO2peak was <50% of predicted in 9 tests (4%), 50%–79% of predicted in 62 tests (30%), 80%–119% of predicted in 121 tests (59%) and ≥120% of predicted in 11 tests (5%). A tendency towards lower VO2peak in percentage of predicted was observed in patients with PI compared with PS (86%±22% vs 91%±20%, p=0.057). In CPETs with a low CRF (<80% of predicted) (n=71, 35%), a ventilatory limitation was found in 16 (23%), exercise induced hypoxaemia in 33 (46%) and signs of VQ mismatch in 6 (8%). In 14 CPETs more than one limiting factor was identified. Three limiting factors was found in 2 CPETs. In 31 tests (44%), no cardiopulmonary limiting factors could be identified.
ANOVA for VO2peak (mL kg−1 min−1) between the defined age cohorts did not reveal any age-related decrease in men or women. When correcting for the expected physiological reduction of VO2peak with increasing age by using VO2peak in percentage of predicted, no age dependent reduction could be established, neither when both genders were pooled nor when split.
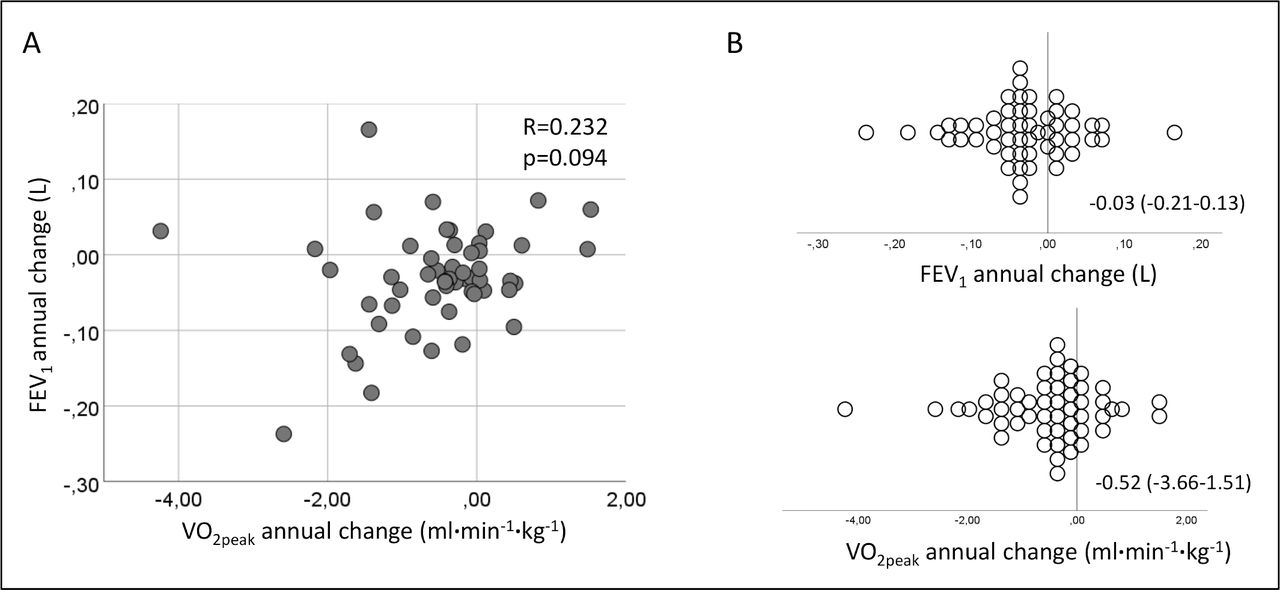
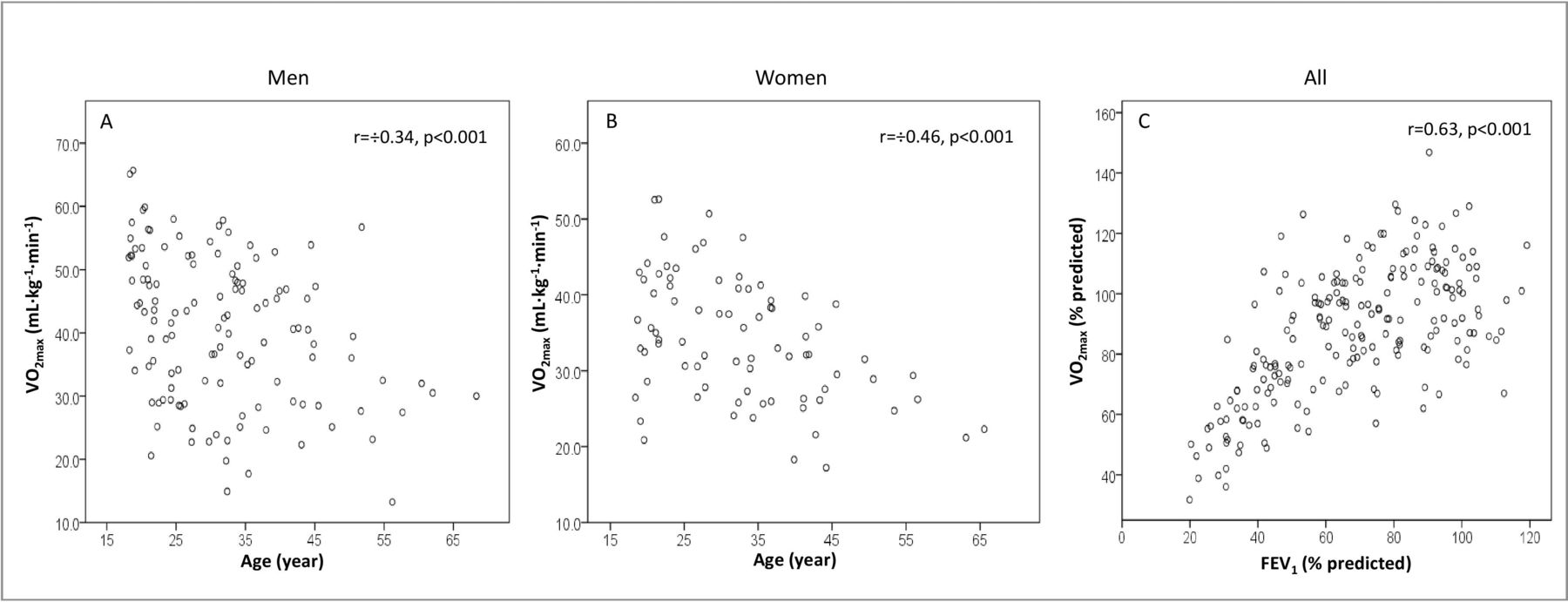
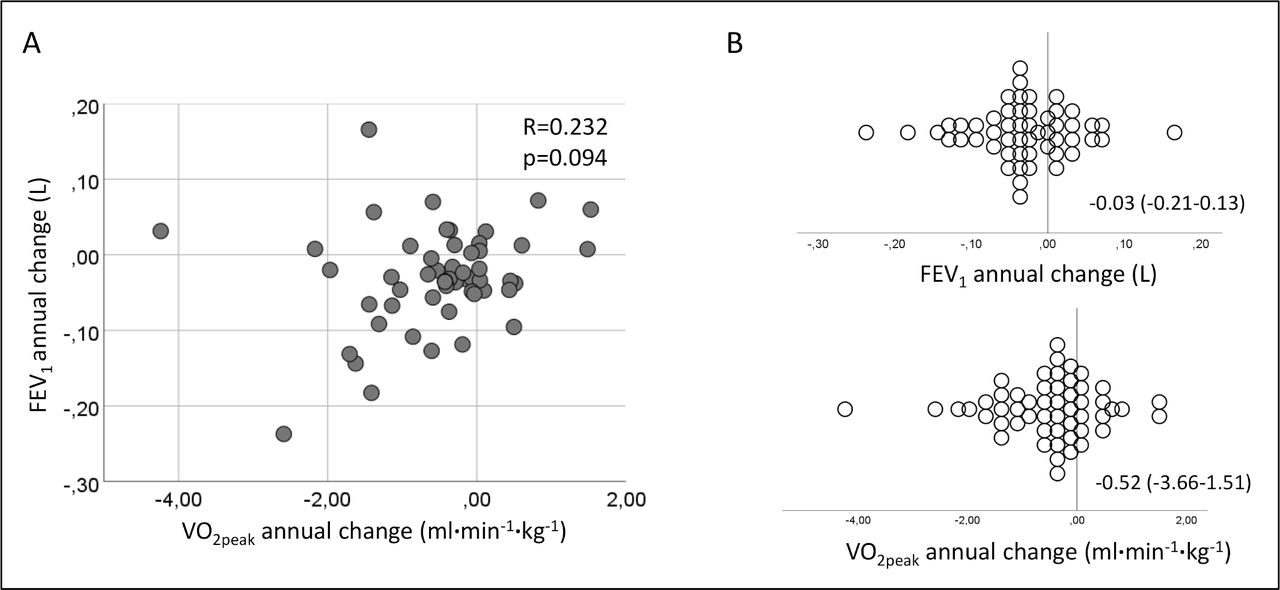
The correlation between VO2peak and age for men and women was −0.46 and −0.34, respectively (both p<0.001) (figure 1A,B). Between VO2peak and FEV1 (both in %-predicted) for both genders combined the correlation was r=0.63 (p<0.001) (figure 1C). For the 53 patients that had performed three or more tests, linear regression was used to calculate longitudinal data for FEV1 and VO2peak (expressed as annual change in mL and mL min−1 kg−1, respectively). The median observation period for the longitudinal data was 7.9 (2–17) years. The mean annual change in FEV1 and VO2peak was −31 mL (95% CI −212-132) and −0.52 mL min−1 kg−1(95% CI −3.66-1.51), respectively (figure 2B) and the correlation between the two parameters was r=0.23 (figure 2A). In the 71 CPETs where VO2peak was low (VO2peak <80% of predicted), the corresponding FEV1 varied from 20% to 112% of predicted.
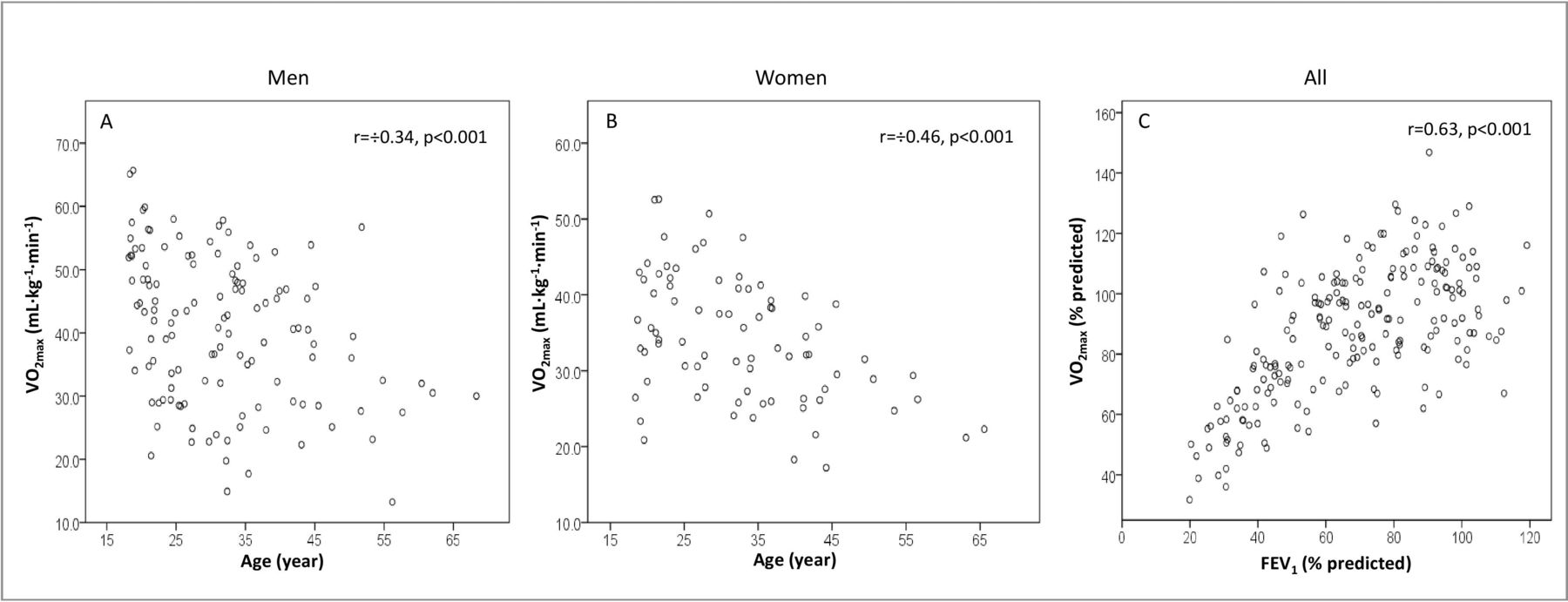
Correlation between peak oxygen uptake (VO2peak) and age for men (A), women (B) and for forced expiratory volume after 1 s (FEV1) for all patients (C).
{kind=link}
{kind=link}
Correlation between the annual changes in forced expiratory volume after 1 s (FEV1) and peak oxygen uptake (VO2peak) (A), and scatter-plots for annual changes in FEV1 and VO2peak (mean and 95% CI in text) (B).
Discussion
The present study describes the CRF in a large adult CF population age 18–68 years, and evaluates the cause of low CRF. In addition, the association between VO2peak and FEV1 and between the annual changes in VO2peak and FEV1, were assessed. The main findings were that CRF, as measured by VO2peak, was well preserved, as two-thirds of the tests resulted in scores within the reference limits of healthy Norwegians.31 In tests demonstrating a low CRF, 44% showed a normal cardiorespiratory response without any sign of ventilatory limitation, hypoxaemia or VQ mismatch (gas exchange limitation). The R-squared value between VO2peak and FEV1, both in percentage of predicted, was 0.41, indicating that 41% of the variance in VO2peak could be predicted by FEV1. Further, there was no significant correlation between the calculated annual changes in FEV1 and VO2peak, where only 5% of the variance in annual VO2peak change could be attributed to annual FEV1 change.
Cardiorespiratory fitness
The CRF in the majority of the CF population was found to be within the reference values of healthy Norwegians.31 Surprisingly, a normal CRF could be achieved despite a markedly reduced FEV1 (as low as 35% of predicted). Our data showed markedly higher VO2peak than previously reported in CF populations consisting of adolescents and young adults from Germany and Switzerland,18 in young adults from Belgium23 and in adults from UK.24 This difference cannot be explained by a better preserved FEV1 in our population, but may partly be due to the use of a treadmill instead of a cycle ergometer in the present study.26 27 It is well known that VO2peak is task specific, and is most reliably measured during dynamic work that uses large muscle groups such as uphill walking and running. Consequently, VO2peak is 10%–20% higher during uphill walking and running compared with cycling in both healthy individuals27 33 34 and in patients with lung disease.26
In addition to high RER and RPE (BORG scale score), a high HR in the present study indicates excellent effort by the patients in the vast majority of tests and good validity of our data. Even though satisfactory RER levels were reported in the two above-mentioned previous studies18 23 as well, the use of a cycle ergometer implies higher RER levels at lower physical effort due to earlier contribution of anaerobic metabolism.33 We find a significantly lower FEV1 in the subgroup of patients not reaching RER ≥1.10, which is in accordance with the previous finding that RER is of limited value as a sole end-criterion for maximal effort in patients with severely reduced lung function.27 Our database does not include any measurement of daily physical activity. Thus, the possibility of a higher physical activity level in our CF population contributing to the higher VO2peak in the present study, cannot be clarified.
As CF is a progressive disease, a more pronounced age-related reduction of VO2peak than in the general population would be expected. However, by studying VO2peak in percentage of predicted, thereby correcting for the age-related fall in VO2peak in the general population, no significant difference between the age cohorts were observed. This finding might be caused by a combination of effects leading to the skewing towards milder disease phenotypes in the higher age cohorts. Patients with severe phenotypes are less likely to be represented in the highest age cohorts of the study due to higher mortality at young age, increased prevalence of bacterial colonisation which prevented CPET due to hygienic concerns and a higher likelihood of being lung-transplanted.
CF disease-severity is known to correlate with exocrine pancreatic function status, and patients with PS most often present a milder disease course as compared with patients with PI.35 This is in accordance with our results, showing lower FEV1 and a tendency towards lower VO2peak in patients with PI. Unfortunately, our database does not include information regarding other disease manifestations (eg, CT scores, bacterial colonisation, diabetes, inhaled antibiotics) that might influence CRF.
Causes of low CRF
VO2peak has been shown to correlate well with prognosis and survival in CF.2 12 As shown by others, and confirmed by our data, FEV1 measurement alone will not allow for an invariable identification of individuals with impaired CRF.7 Further, whereas many exercise tests will identify a low CRF, only more complex measures, such as a CPET, will provide detailed information about the underlying cause.7 27 In tests with a low CRF (<80% of predicted) (n=101), a ventilatory limitation was found in 23%, exercise induced hypoxaemia in 46% and signs of VQ mismatch in 8%. In 44% of the tests, no cardiopulmonary limiting factors could be identified, and the low CRF in this group is probably due to deconditioning. Thus, CPET may provide valuable guidance for the clinician in order to choose an adequate intervention measure, in this case exercise therapy.
Correlation between VO2peak and FEV1
The correlation between VO2peak and FEV1, both in percentage of predicted, indicates that 41% of the reduction in VO2peak can be explained by FEV1. The annual change in VO2peak could not be attributed to changing FEV1. In some cases, patients with a low CRF had well-preserved lung function, as defined by FEV1. Vice versa, some patients with a severely reduced FEV1 achieved a normal CRF. This is in accordance with studies in patients with obstructive lung diseases,7 finding FEV1 a poor indicator of the patients physical function.
Strengths and limitations
The present study includes a high number of tests and covers a large age-span for both men and women with CF. In addition, all test were performed on a treadmill, which is shown to results in a higher VO2peak than cycle ergometer testing in patients with other lung diseases.26 All measurements were performed by the same exercise physiologists using the same equipment and test protocol throughout the whole data collection period of 12 years.
Regarding limitations, some patients may have higher impact on the overall results due to a higher number of CPETs performed in the data collection period, even though no patient were represented more than once in each age-cohort. Unfortunately, we did not measure exercise tidal flow-volume loops for detection of exercise induced dynamic hyperinflation and flow-limitation, a phenomenon which may have a negative impact on CRF.
Conclusions
To our knowledge, no previous studies have described CRF in an adult CF population of this size and age-span measured on a treadmill. Two-thirds of the tests resulted in a VO2peak within the reference limits of the general population. In those with impaired CRF, no cardiorespiratory limitation could be identified in a surprisingly large proportion, indicating deconditioning as a major contributor to reduced CRF in CF. Thus, CPET can be used to identify a patient group in which exercise therapy will be especially beneficial. The latter notion represents an incentive for future intervention trials. CRF in patients with CF cannot invariably be predicted by FEV1.
References
Footnotes
Contributors All authors have given substantial contributions to the submitted article and have approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study is approved by the Oslo University Hospital’s Data and Privacy Protection Officer (approval 18/09502, database 2016/3030), provided that the anonymity of all individual test results is maintained.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Derived data might be available from the corresponding author AO upon reasonable request and after evaluation by Oslo University Hospital’s Data and Privacy Protection Officer.