Article Text

Abstract
Objective To investigate the diagnostic accuracy of MRI for identifying posterior element bone stress injury (PEBSI) in the athletic population with low back pain (LBP).
Study Design A systematic review searched for published sources up until July 2020. Eligibility criteria: prospective cohort design, MRI diagnosis, adolescents/young adults, chief symptoms of LBP, PEBSI as the clinical diagnosis and SPECT-CT as reference standard. Risk of bias and overall quality were assessed using QUADAS-2 and GRADE, respectively. A narrative synthesis was conducted.
Results Four studies were included, with three included in the quantitative synthesis. Compared with SPECT-CT, two studies involving MRI demonstrated sensitivity and specificity of 80% and 100%, and 88% and 97%, respectively. Compared with CT, one study involving MRI demonstrated sensitivity and specificity of 97% and 91%, respectively. Risk of bias was moderate to high although consistency across studies was noted.
Conclusion Findings support further research to consider MRI as the modality of choice for diagnosing PEBSI. MRI was consistent with SPECT-CT for ruling-in PEBSI, but the clinical value of cases where MRI had false negatives remains uncertain due to possible over-sensitivity by SPECT-CT.
PROSPERO registration number CRD42015023979.
- Diagnosis
- Back injuries
- Evidence based review
- Athlete
- MRI
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Posterior element bone stress injury (PEBSI) is one of the most common reasons for low back pain (LBP) in athletic populations with reported incidence of 14–35%, especially in sports such as gymnastics, diving and throwing sports.1 LBP may hinder athletic performance,2 impact on health and contribute to time loss from training and competitions.3 This may also lead to untimely cessation of professional careers.4 Diagnosis of PEBSI, however, may help where existing evidence suggests that early diagnosis (ie, prior to an established fracture (spondylolysis)) allows causative factors to be identified and remedied, thus lessening the probability of progression to complete fracture and improving full-union bone healing.5 Late diagnosis increases the risk of non-union, surgery and lengthy rehabilitation.2
Clinically, individuals present with back pain that is exacerbated with extension, side flexion, or a combination of both that increases during sporting activities but decreases with rest, and is usually without neurological signs.1 The single-leg hyperextension test is commonly used to confirm secondary conditions that may develop as a result of delayed diagnosis of PEBSI (spondylolysis and/or spondylolisthesis); however, a recent systematic review has concluded that neither this test nor the clinical history have the diagnostic utility to confirm any of these conditions.6 These recent findings support the importance of diagnostic imaging for this spectrum of conditions.
Existing evidence suggests that early PEBSI is occult on X-rays1 7 and can be even missed with CT,8–10 when the cortical bone is still intact. Consequently, MRI and single-photon emission computerised tomography (SPECT) are used for their sensitivity to detect this crucial early phase with bone morrow oedema,8 and increased tracer uptake (hotspot),9 respectively. Nevertheless, the gold standard modality for diagnosing PEBSI remains a subject of controversy.1 11 Despite this lack of agreement and the exposure to ionising radiation, which frequently includes radioactive tracer injections in adolescents, there is still a tendency by some experts to use X-ray as the first line of investigation followed by SPECT and/or CT.11 The possible consequences of either late diagnosis and/or over-exposing young athletes to ionising radiation warrant further clarification.
Three recent systematic reviews were identified12–14 however none focused on the crucial early phase. Based on the scarcity of literature on PEBSI, there is an urgent need to provide recommendations of the most suitable modality for diagnosing PEBSI, with a particular interest in the early stages of bone stress reactions.
Objective
To investigate the diagnostic accuracy of MRI for identifying PEBSI in the athletic population with LBP.
METHODS
Design
A systematic review was conducted according to a registered protocol (PROSPERO CRD42015023979) and based on the Centre for Reviews and Dissemination.15 The review is reported in line with PRISMA (online supplemental file 1).16 See online supplemental file 2 for detailed report of the methodology.
Supplemental material
Supplemental material
RESULTS
Study selection
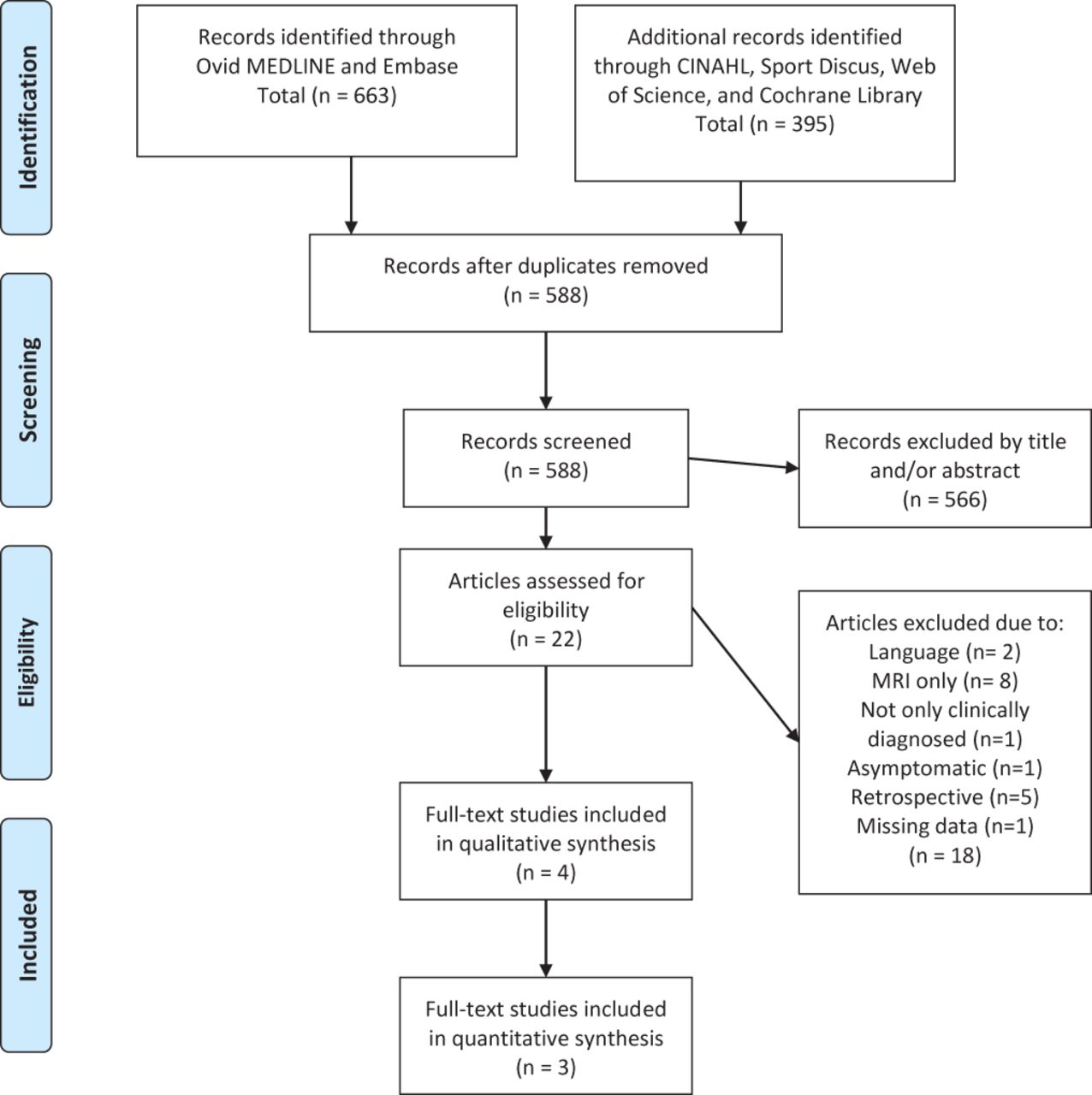
From 1058 records, 588 studies were included. See the PRISMA flow diagram for study selection process (figure 1). One author failed to respond for missing data to determine eligibility.17 Four studies were included in the synthesis.18–21
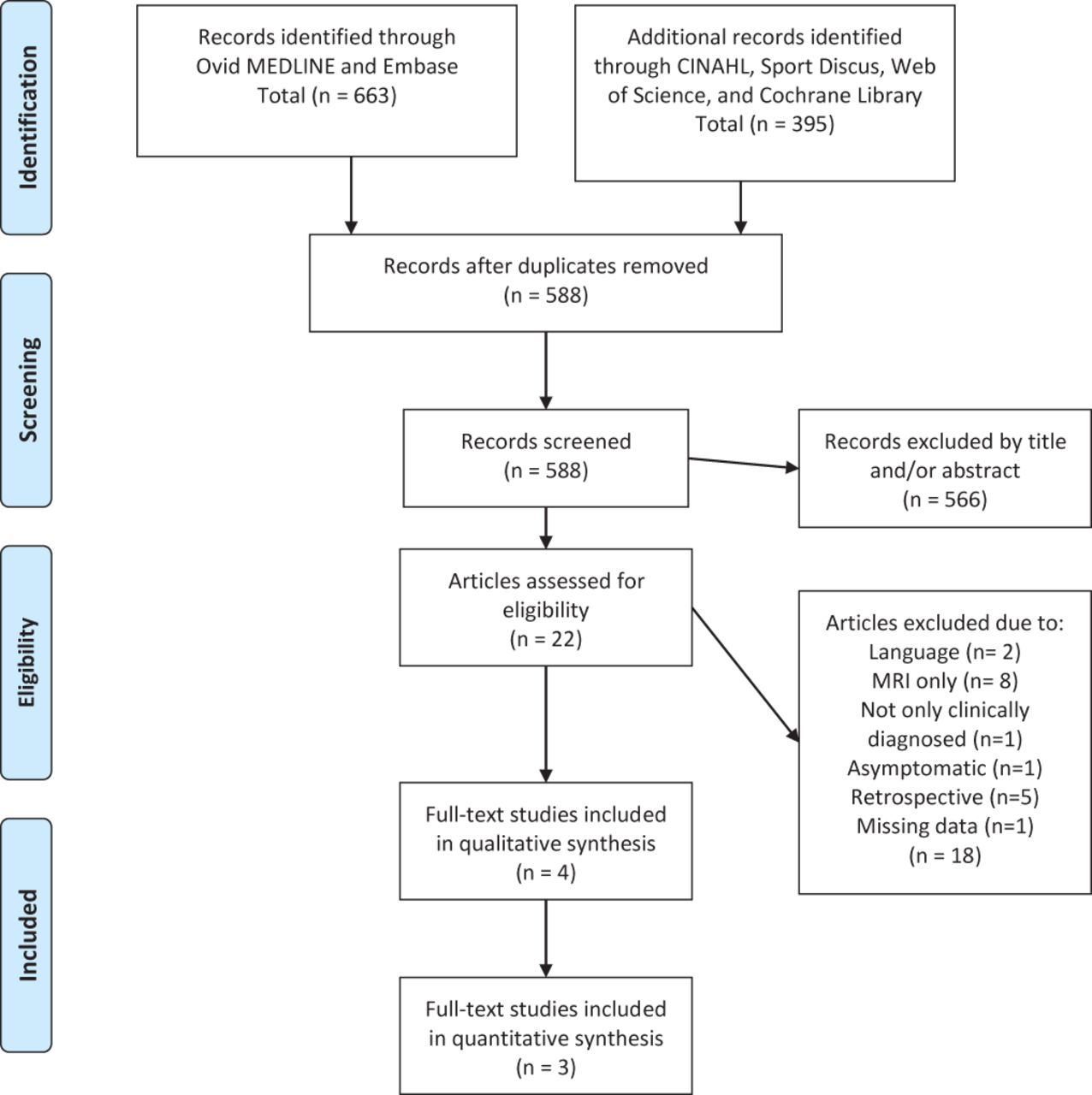
PRISMA flow chart.
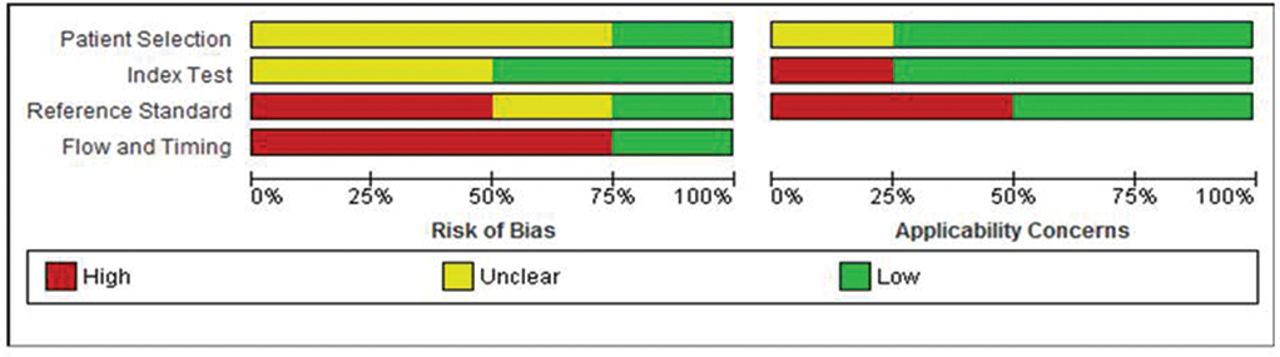
Risk of bias (ROB) and applicability concerns.

{kind=link}
{kind=link}
{kind=link}
Diagnostic accuracy estimates with 95% CI forest plots.
Study characteristics
The weighted mean age was 14.9 years,18 20 21 including 62–74% males. Symptom onset to imaging investigation varied but was less than 6 months19 and 36 days on average.21 The common objective for all studies was to evaluate the usefulness of MRI in identifying spondylolysis and the use of optimised parameters to diagnose PEBSI. Most studies aimed to evaluate the efficacy of MRI at early and/or acute stages of spondylolysis that is, PEBSI18 19 21; with one study investigating whether MRI could effectively replace SPECT-CT altogether.20 Two studies considered SPECT-CT and MRI as the reference standard and index test, respectively.19 20 The other two studies used only CT in their comparison with MRI18 21; and although not explicit, CT was considered as the reference standard. Further, Yamane et al 21 also reported the results of their follow-up CT, which were used in their comparison with MRI findings. Kobayashi et al 18 performed CT scans based only on positive MRI results, and thus did not provide the data to construct a 2×2 table summary. This study was therefore excluded from the quantitative synthesis. See table 1 for details of study characteristics.
Summary of included studies
Risk of bias (ROB) within studies and concerns for applicability
A summary of results is presented in table 2. Strength of agreement for ROB assessment was very good (Kappa=0.9, 95% CI 0.79 to 1). None of the included studies were at low ROB with most domains deemed unclear or at high ROB. Participant recruitment was unclear in most studies,19–21 and thus selection bias could not be excluded. Similarly, lack of clarity was also noticeable of the index domain in defining the criteria for a positive result.19 21
QUADAS-2 appraisal form
Quality of evidence
All included studies started as high quality because of their diagnostic framework.22 Nevertheless, other factors, primarily the high ROB, decreased the overall quality of evidence. Also, patient important outcomes, such as benefit and/or harm, were not assessed within the included studies. Summary of GRADE can be viewed in table 3.
GRADE quality assessment of the body of evidence
Results of individual studies
Most studies showed consistent results. Two studies, investigating the diagnostic accuracy of MRI versus SPECT-CT, demonstrated MRI sensitivity of 80% (95% CI 65 to 89) and MRI specificity of 100% (95% CI 99 to 100),19 and MRI sensitivity of 88% (95% CI 75 to 95) and MRI specificity of 97% (95% CI 94 to 98).20 The study by Yamane et al,21 that investigated the diagnostic accuracy of MRI versus CT, demonstrated MRI sensitivity of 97% (95% CI 85 to 99) and MRI specificity of 91% (95% CI 85 to 95). The sequences used in this study could not distinguish between stages of non-lysis and pseudarthrosis, thus values were calculated based on the presence and absence of abnormal MRI signal. Consequently, pseudarthrosis cases that had no abnormal signal on MRI were considered chronic and, therefore, true negative. If calculated according to CT classification, the outcome would be incorrect, and misleading. Additionally, calculating the acute stage alone, that is, without pseudarthrosis, maintained a high level of accuracy.
Overall, the diagnostic value of MRI for ruling PEBSI in was conclusive, and moderate to conclusive for ruling it out.
Synthesis of results
Meta-analysis was inappropriate due to the low number of studies (2), quality and clinical heterogeneity.15
DISCUSSION
This is the first systematic review to investigate the diagnostic accuracy of MRI for identifying PEBSI in the lumbar spine in young athletes with LBP. MRI’s accuracy was found high and consistent throughout in comparison with SPECT-CT.
The diagnostic value of MRI for ruling PEBSI in was conclusive across all studies, and moderate to conclusive for ruling it out. Accuracy estimates were calculated based on normal versus abnormal scans for clarifying the ability of MRI in distinguishing between the presence and absence of posterior element pathology. The confidence in the overall quality of evidence is low to moderate. MRI was as accurate as CT in detecting fully formed fractures. With respect to follow-ups, where cortical bone disruption is not evident on CT,10 MRI offers insights to stages of healing owing to its sensitivity to bone marrow oedema.8 Kobayashi et al 18 demonstrated that 43% of participants with positive findings on MRI were occult on reverse gantry-CT even with prior knowledge of MRI detected changes.
With respect to the early stages of fracture development, high levels of false negative were found for MRI compared with SPECT.19 20 Reasons for this are two-fold. First, as opposed to CT and MRI, there is no established grading system defining SPECT abnormalities in the lumbar spine. In the absence of a rigorous grading system to a particular diagnosis, reliability findings of observers are of limited value.26 Masci et al,19 for example, not only lacked a clear classification system for SPECT, but also modified a validated classification system for MRI.27
Second, SPECT is highly sensitivity to ongoing bone turnover activity.9 Essentially, in the absence of a true reference standard, caution should be taken as to the clinical value of positive SPECT scans. Scintigraphy uptake occurs frequently in athletes (34–45.2%) in non-painful sites.28 Such, false positive cases are commonly regarded as adaptive changes and are perceived normal.28 With the evidence supporting SPECT over planar bone scans for its enhanced sensitivity,9 it may be even more difficult distinguishing what ‘normal’ uptake is.
Lastly, patient-important outcomes such as exposure to ionising radiation and the associated risks in the athletic population should not be overlooked. The effective dose from a single course of X-ray and SPECT-CT scans is 10X more,29 than what UK dwellings get in a year from natural background radiation exposure.30
In contrast to previous reviews,12–14 our findings recommend seeking consensus about shifting the diagnostic focus to the earliest, potentially reversible, PEBSI stage. Accordingly, use of radiographs should be discouraged7 and with advancements in MRI, the latter should be considered as the first-line investigation in all circumstances. Further, volumetric interpolated breath-hold examination (VIBE) MRI scan was found accurate in characterising incomplete pars fractures in comparison with CT.8 These sequences, however, are not sensitive to bone marrow oedema.31 Consequently, VIBE sequences should be incorporated in a PEBSI MRI protocol with other highly sensitive sequences to bone marrow oedema. This takes into account the continuum of this condition, thus avoiding complementary diagnostic imaging and hence saving time, money and avoiding radiation exposure.
Strengths and limitations
This is the first review to consider patient-important factors to inform evidenced-based decisions regarding the use of imaging for identifying PEBSI, especially in the absence of a gold-standard consensus. Publication bias was minimised as the search excluded two possible non-English studies, which nonetheless were not discussed in similar studies.
CONCLUSION
Findings suggest MRI having an important role in the diagnosis of PEBSI, with consistency between MRI and SPECT-CT in ruling-in PEBSI but importantly without the exposure to ionising radiation. Further research is required to consider MRI as an alternative to SPECT-CT and to balance benefits versus risks for the appropriate investigation approach.
What is already known?
MRI and SPECT are considered the most sensitive modalities for assessing early signs of stress fracture.
There is no clear-cut gold standard for confirming the diagnosis of PEBSI.
MRI, unlike other modalities, has no risks of exposure to ionising radiation.
What are the new findings?
Clinically, the diagnostic value of MRI for ruling PEBSI was conclusive, and moderate to conclusive for ruling it out.
The available literature for investigating PEBSI is scarce and low in quality.
In the process of choosing an imaging modality, patient-important outcomes may assist in the clinical decision making.
REFERENCES
Footnotes
Twitter Nicola Heneghan @Nicola_Heneghan.
Contributors The initial protocol and design were developed by RE, RK, KS, SS, LF, AR and NRH; RE, LHJG, RK, KS and NRH were involved in the completion of searches, data extraction, quality assessment and analysis; all authors contributed to the interpretation and write-up of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.