Article Text

Abstract
Objective Conventionally, knee extension strength is often used as the indicator for lower limb muscle strength; however, several recent studies have also used quadriceps setting strength. This study aimed to investigate and compare the association of quadriceps setting and knee extension strength with health-related physical fitness.
Methods We evaluated quadriceps setting strength and isometric knee extension strength in 75 elderly subjects (mean age, 76.8±5.3 years) to determine their lower limb muscle strength. Health-related physical fitness was evaluated using the physical fitness test advocated by the Ministry of Education and Culture, Sports, Science and Technology in Japan. The test consists of the following components: grip strength, sit-up, sit and reach, one leg standing with eyes open, 10 m obstacle walk and 6 min walk.
Results When adjusted for age, sex and body mass index, quadriceps setting strength was significantly correlated with grip strength, number of sit-ups, sit and reach distance, 10 m obstacle walking time and 6 min walking distance. In contrast, knee extension strength was associated only with grip strength and number of sit-ups.
Conclusion More health-related physical fitness parameters with quadriceps setting strength than knee extension strength. Quadriceps setting strength may be superior to knee extension strength as a predictor of health-related physical fitness.
- elderly people
- strength isometric isokinetic
- physical fitness
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings?
Quadriceps setting strength is associated with various physical fitness tests (grip strength, sit-up, sit and reach, 10 m obstacle walk and 6 min walk), independently of age, sex and body mass index (BMI).
When adjusted for age, sex and BMI, knee extension strength is related only to the grip strength and sit-up tests.
Health-related physical fitness has a stronger association with quadriceps setting strength than with knee extension strength.
Introduction
Muscle weakness can affect the physical independence of elderly people. The age-related loss of lower limb muscle strength is associated with poor functional performance,1 physical disability,2 3 falls4 and mortality.5 Several parameters such as hip abductor muscle strength, knee flexion and extension muscle strength are used to evaluate lower limb muscle strength. In particular, knee extension muscle strength is often adopted to evaluate lower limb muscle strength because knee extension strength is more strongly related to activities of daily living (ADL) than other parameters.6 7
Quadriceps setting strength is an alternative measurement used to determine lower limb muscle strength.8 It is measured through the quadriceps setting exercise, which involves training of the quadriceps femoris muscle. Interestingly, Inoue et al9 investigated the association between lower limb muscle strength and gait in elderly individuals and found that quadriceps setting strength was the most important determinant of walking speed compared with other muscles of the lower limb. This suggests that quadriceps setting strength may be more strongly associated with physical function than other parameters used to evaluate lower limb muscle strength. However, few studies have clarified the usefulness of using quadriceps setting strength in this regard.
Understanding the best way to measure lower limb muscle strength is important to ensure early detection and prevention of decline in the physical function of elderly individuals. In addition, it is important to determine the overall physical fitness of elderly people. Health-related physical fitness, which consists of four domains including strength and endurance of muscle, flexibility, cardiorespiratory fitness and body composition, is essential for having healthy daily lives of elderly individuals.10 11 Therefore, the aim of the present study was to investigate and compare how closely the quadriceps setting and knee extension strength values relate to health-related physical fitness.
Methods
Subjects of the study
The subjects were 75 (23 men and 52 women) community-dwelling elderly people. They belonged to a senior club in Kyoto and volunteered to participate in a physical fitness test held by the club. Recruitment was conducted through information posted on bulletin boards, circular notices and websites. The inclusion criteria for this study were as follows: (1) age ≥65 years, (2) valid measurements of quadriceps setting strength and isometric knee extension strength and (3) living at home, with the capacity of self-care. Informed consent was obtained from all subjects.
Measurements of lower limb muscle strength
Lower limb muscle strength was determined by measuring quadriceps setting and knee extension strength. The muscle strength in the right and left legs was measured twice after a trial measurement. The highest value of the two measurements was registered and used for analysis.
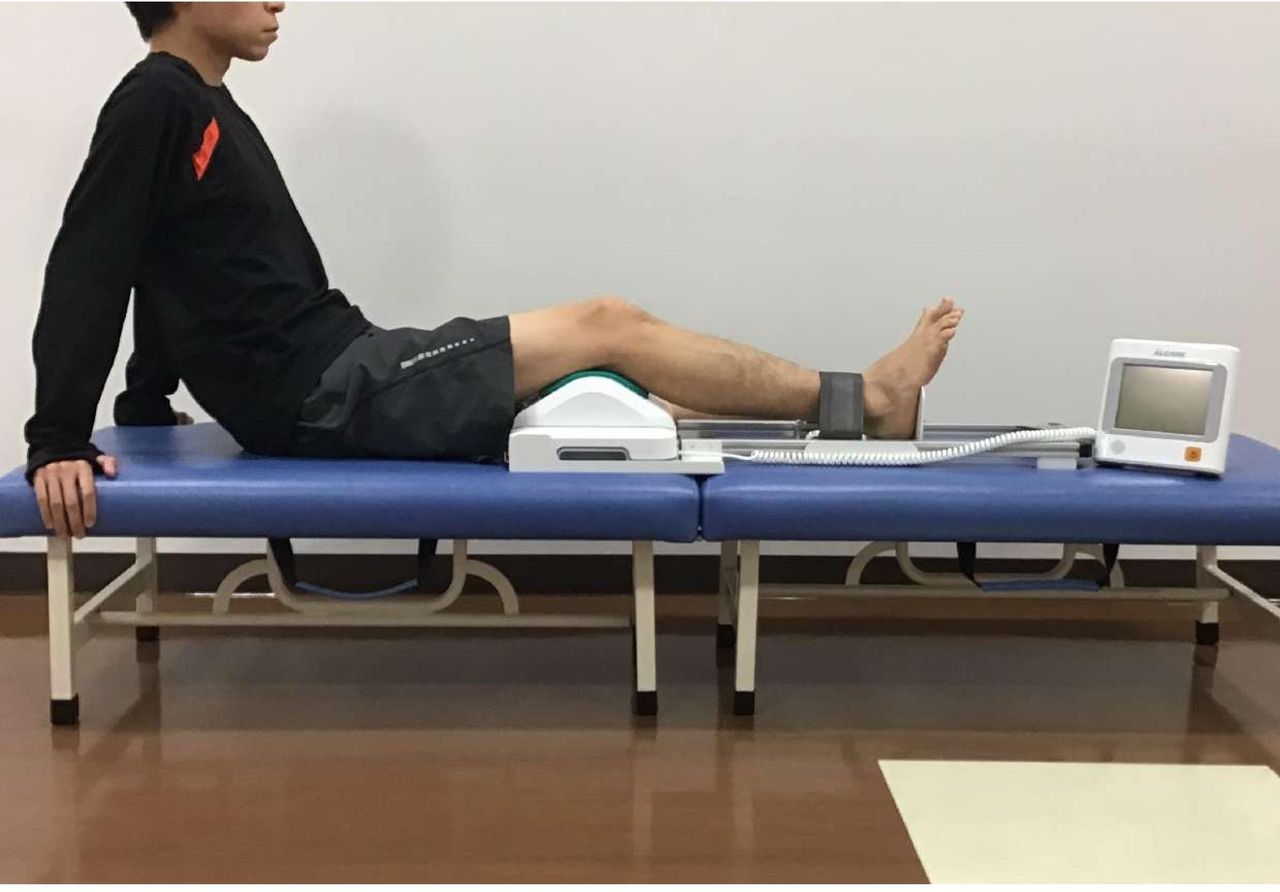
Quadriceps setting strength was measured using a Locomoscan device (Alcare Co Ltd, Tokyo, Japan).8 12 As shown in figure 1, a force sensor was placed in the popliteal fossa in a long sitting position. The distal leg participating in the movement was fixed using a belt. The subjects were asked to extend the knee with maximum force.
{kind=link}
Quadriceps setting strength measuring system.
Knee extension strength was measured using a custom-made dynamometer chair, as previously described.13 The ankle was attached via a belt to a dynamometer (T.K.K.5710e, Takei Scientific Instruments Co Ltd, Niigata, Japan). The subjects were in a sitting position with the hip and knee flexed 90° and were required to extend the knee with maximum force.
Measurements of health-related physical fitness
Health-related physical fitness was evaluated using the physical fitness test for elderly individuals, which was approved by the Ministry of Education, Culture, Sports, Science and Technology (MEXT) in Japan.14 This test emphasises the measurement of health-related physical fitness and consists of six tests: grip strength, sit-up, sit and reach, one leg standing with eyes open, 10 m obstacle walk, and 6 min walk. These were measured in accordance with the guidelines of the MEXT in Japan.14
Statistical analysis
The relationship between lower limb muscle strength (quadriceps setting and knee extension strength) and health-related physical fitness (grip strength, sit-up, sit and reach, one leg standing with eyes open, 10 m obstacle walk and 6 min walk) was assessed using the Pearson's correlation coefficients. In addition, the partial correlation coefficients adjusted for age, sex and body mass index (BMI) were used. The 95% CIs were calculated for the correlation and partial correlation coefficients. The data were analysed using IBM SPSS Statistics V.25.0 (IBM Corp, Armonk, New York, USA). The level of statistical significance was set at p<0.05.
Results
The characteristics of the subjects and results obtained in each individual tests are shown in table 1.
Characteristics of the subjects and results of each test of the health-related physical fitness assessment
On average, men had higher measurements than women for height, weight, knee extension strength, grip strength and 6 min walking distance; however, men had shorter 10 m obstacle walking time than women.
The correlation coefficients between quadriceps setting strength, knee extension strength and individual tests of the health-related physical fitness assessment are shown in table 2.
Single correlation between quadriceps setting and knee extension strength with individual test of the health-related physical fitness assessment
Quadriceps setting strength was significantly associated with grip strength, number of sit-ups, sit and reach distance, one leg standing time, 10 m obstacle walking time and 6 min walking distance. knee extension strength was only significantly related with grip strength, number of sit-ups, 10 m obstacle walking time and 6 min walking distance.
The partial correlation coefficients between quadriceps setting and knee extension strength with individual test of the health-related physical fitness assessment are shown in table 3.
Partial correlation between quadriceps setting and knee extension strength with individual test of the health-related physical fitness assessment
When age, sex and BMI were defined as control variables, both quadriceps setting and knee extension strength were significantly correlated with grip strength and number of sit-ups. However, when adjusting for age, sex and BMI, quadriceps setting strength significantly correlated with the sit and reach distance, 10 m obstacle walking time and 6 min walking distance, whereas knee extension strength was not significantly associated with any of these tests.
Discussion
Lower limb muscle strength generates a propulsive force forward during walking, playing a role in supporting the lower limb. Previous studies have reported that lower limb muscle strength is related to balance and walking ability.15–18 This study showed that quadriceps setting and knee extension strength were significantly associated with health-related physical fitness; however, the coefficient of quadriceps setting strength was higher than that of knee extension strength, with the exception of grip strength and number of sit-ups. The difference in muscles and joints mobilised when exerting muscular strength may affect the results of this study. Previous studies reported that not only the quadriceps femoris muscle but also the hip extensor muscles, such as the hamstrings and gluteus maximus, are active in quadriceps setting exercises.19 20 Therefore, it is considered that quadriceps setting strength requires cooperation of multiple muscles because both the knee and hip joints are extended when exerting quadriceps setting strength. In contrast, only the knee joint is extended when knee extension strength is exerted. Some studies have shown that lower limb muscle strength by multijoint movements had stronger relationships with physical performance and ADLs than lower limb muscle strength by single-joint movements.21 22
The 10 m obstacle walk and 6 min walk tests evaluated the functional walking ability of the subjects. The 10 m obstacle walk requires a high dynamic balance ability to support the body with a single leg when straddling an obstacle. Brown et al23 showed that avoiding obstacles in daily life poses a risk of falls among elderly individuals. In addition, falls are a significant cause of mortality in older adults.24 25 The 6 min walk measures the cardiorespiratory fitness and associates with diseases such as diabetes and cardiovascular disease.26 27 In the present study, we found that these tests, related to not only walking ability but also the risk factors for falls and various diseases, showed a stronger association with quadriceps setting strength than with knee extension strength.
The measurement of quadriceps setting strength is easy because the device used to measure it is readily movable, and the test can be performed in a small space.8 The ability to measure the physical fitness of elderly individuals at locations other than hospitals and research institutes makes it possible to evaluate a higher number of people. From the viewpoint of early detection and primary prevention, an indicator that can detect a decline in physical function in a healthy population and can be measured easily is invaluable. Hence, when using quadriceps setting strength to evaluate physical function in elderly individuals, it can become a valuable parameter to detect a decline in the physical function at an early stage.
The present study has several limitations. We cannot assume that the subjects of the present study represent the general elderly population in Japan, owing to sampling bias. In addition, the number of subjects in our study was small. Nevertheless, our findings provide a foundation for larger prospective studies to determine a relationship between quadriceps setting strength and health-related physical fitness in elderly individuals.
Conclusion
We clarified that health-related physical fitness has a stronger association with quadriceps setting strength than with knee extension strength, which is often used to evaluate lower limb muscle strength. Our findings suggest that quadriceps setting strength can, therefore, be useful in the early detection of the decline in physical function.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Doshisha University of Human Subject Research Ethics Committee (approval no. 17081).
Acknowledgments
We thank everyone in the Kita Ward Health Club who participated in this study and also the staff of the Kyoto-Murasakino Community General Support Centre.
References
Footnotes
Contributors YI contributed to conception and design, data collection and analysis, drafting and revising the manuscript. TA, TS and KO contributed to data collection and revised the manuscript. KI contributed to conception and design and helped to draft the manuscript. All authors approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.