Article Text

Abstract
Objective The primary aim of this study was to estimate the prevalence of depressive symptoms and life stress in elite coaches. The secondary aim was to explore the associations of depressive symptoms and life stress with demographic and lifestyle variables.
Methods National-level coaches were invited to participate in an online survey. Depressive symptoms were measured by the Centre for Epidemiological Studies Depression Scale-Revised (CESD-R). Life stress was measured using daily life hassle frequency and severity scores calculated from the Daily Hassles Questionnaire, with associations evaluated using linear regression.
Results Of 110 potential participants, 69 completed and two partially completed surveys were received. The majority of respondents were male (77%), coaching individual sports (70%) and aged under 50 (71%). Overall, 14% of coaches reported at least moderate depressive symptoms according to the CESD-R. Those contemplating retirement were more likely to show depressive symptoms. Reported life stress was higher in females and in those contemplating retirement. There was a strong association between life stress and the odds of experiencing depressive symptoms (p=0.006).
Conclusions Depressive symptoms are as prevalent in elite coaches as in general population, with potential risk factors including high levels of life stress and impending retirement.
- depression
- mental
- psychology
- psychiatry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the new findings
The prevalence of depressive symptoms in elite coaches in New Zealand is 14%. This is lower compared with the elite athletes, but is comparable to the general population.
High levels of life stress are associated with higher odds of depressive symptoms in elite coaches. There may also be an association of depressive symptoms with contemplation of retirement and family history of mood disorders, although further research is needed to confirm these associations.
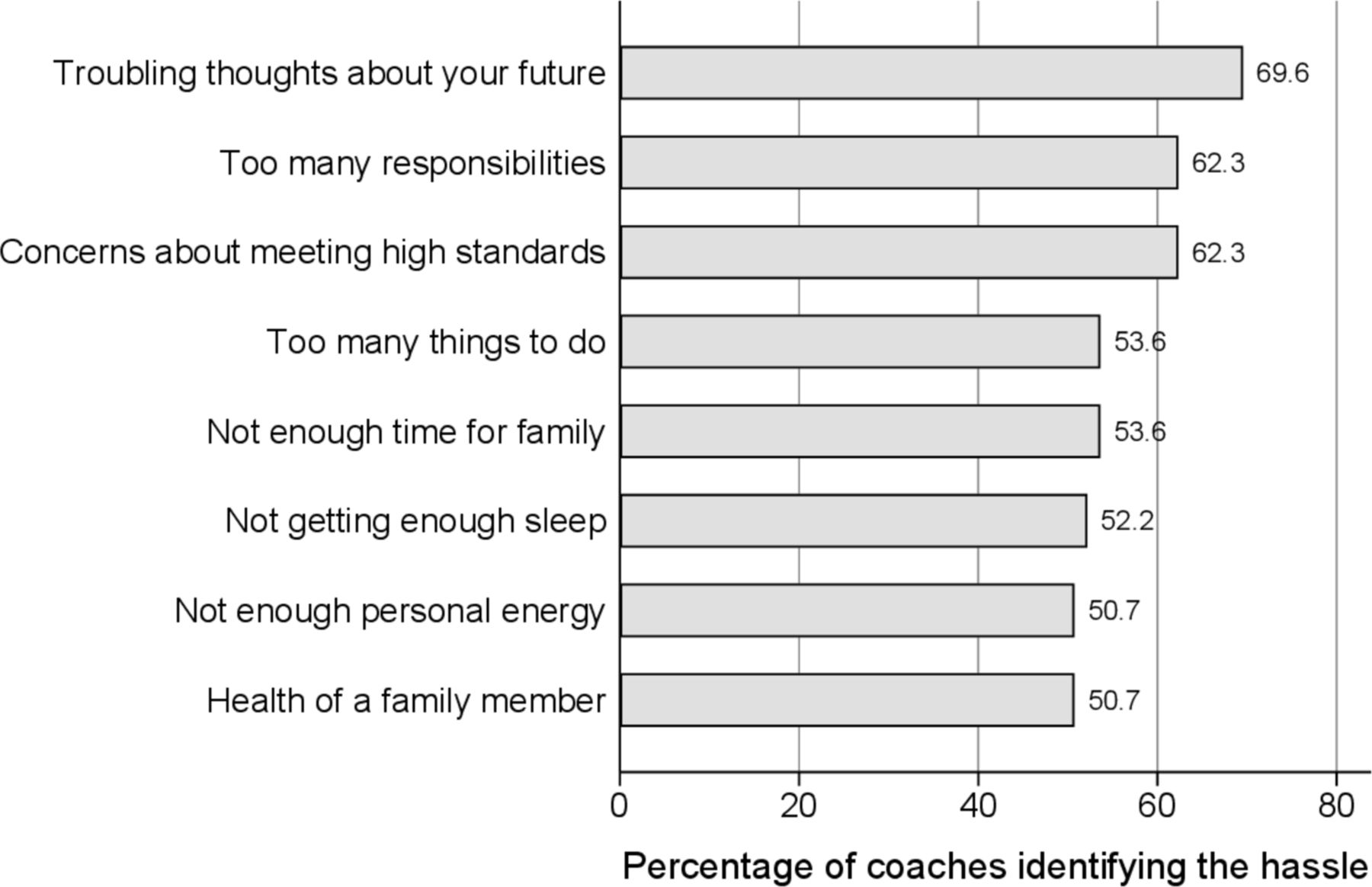
The most common types of life stress for the elite coaches include future thoughts, responsibilities and high standards.
How might it impact on clinical practice in the near future
The findings could help raise awareness about mental health problems in the elite coaching community and lead to enhanced mental health support.
Introduction
Depressive symptoms and disorders are the most prevalent psychological problems worldwide. A recent meta-analysis illustrated the prevalence of symptoms of depression and anxiety in elite athletes to be as high as 34%.1 In New Zealand elite athletes were found to have a prevalence of 21% for depressive symptoms2 while 14% of the adult population has been diagnosed with depression in their lifetime.3 An international professional rugby study, which included New Zealand players, found the prevalence for depressive and anxiety symptoms to be 28%.4 Recognising this issue, the IOC recently published a consensus statement on mental health in elite athletes.5 While there is emerging evidence that other groups, such as elite-level referees, are affected by symptoms of mental health disorders,6 there remains little awareness of the mental health of elite coaches.
Coach roles in elite sport are challenging with multiple functions, expectations and visible outcomes, resulting in many role-specific stressors.7 These include a range of personal and situational factors, contractual matters, a lack of job security, long working hours, unclear expectations, frequent travel and lack of social support.7–9 Existing research has focused on coaches’ approaches to stress management,7 10 and their knowledge and attitudes towards depression among the athletes they coach.11 The prevalence of depressive symptoms in elite sport coaches has not been formally studied.
The primary aim of the current study was to evaluate the prevalence of depressive symptoms and life stressors experienced by New Zealand elite-level coaches. The secondary aim was to explore the potential association of depressive symptoms and life stress with demographic and lifestyle variables.
Methods
A cross-sectional study was conducted among elite coaches working at either a national or international level with elite athletes, employed by either High Performance Sport New Zealand or New Zealand Football and aged 18 years or older. Potential participants received a link to an anonymous online survey (online supplementary appendix 1), which was hosted on a secure online platform. A total of 110 coaches were invited to participate.
Supplemental material
The Centre for Epidemiological Studies Depression Scale-Revised was used to measure symptoms of depression.12 The ‘Daily Hassles Scale’ was used to measure life stress.13 Further details of the questionnaires are presented in the online supplementary section.
Supplemental material
The prevalence of depressive symptoms was calculated along with exact binomial 95% CIs. χ2 test or Fisher’s exact test (for small cell counts) was used to evaluate associations of coach characteristics with the presence of either moderate or major depressive symptoms. Significant associations (p<0.05) were then assessed together in an adjusted logistic regression model, with results presented using ORs and 95% CIs. Potential associations of life stress with coach characteristics were assessed using a Kruskal-Wallis test due to the non-normal distribution of the continuous daily life hassle frequency and severity scores. Significant associations from unadjusted analysis were then evaluated together in a multiple linear regression model. Normality of residuals was evaluated for linear regression models. The association of life stress and depressive symptoms was also considered in unadjusted and adjusted (for coach characteristics associated with depressive symptoms) logistic regression models.
Results
Sixty-nine elite coaches fully completed the survey and two partially completed the survey, resulting in the response rate of 65%. Coach ‘characteristics’ are presented in table 1. The majority of respondents were male (77%), with 15 female (21%) and one gender diverse participants. To protect anonymity, the gender diverse individual was excluded from any analyses including gender.
Characteristics of 71 coaches participating in the survey, overall and by depressive symptoms
The prevalence of depressive symptoms and life stress (number of daily hassles) is shown in table 2. Ten coaches met the criteria for at least moderate depressive symptoms, with a prevalence of 14.1% (95% CI 7.0% to 24.4%). The average number of hassles reported was 24. There was a strong positive correlation between the total number of daily hassles and the average severity score being reported (Spearman’s r=0.63, p<0.001). Figure 1 shows the top-ranked daily hassles reported by the participants.
{kind=link}
Daily hassles experienced by at least 50% of coaches in the study.
Depressive symptoms and life stress in NZ coaches
Unadjusted analysis showed that contemplating retirement (OR=6.56, 95% CI 1.27 to 42.73; p=0.010) and having a family history of mood disorder (OR=4.08, 95% CI 1.01 to 16.41; p=0.037) were associated with a depressive symptom score of ≥16 (table 2). Using an adjusted logistic regression model including both variables, only the association with contemplation of retirement remained significant, where the odds of moderate or higher depressive symptom levels for those considering retirement were 5.71 times higher than those not considering retirement (95% CI 1.27 to 25.63, p=0.023). There were no significant associations between other demographic factors and depressive symptoms.
The total daily hassles and severity score according to coach characteristics are displayed in table 3. Female coaches reported an average of 14 more daily hassles (p=0.022), and perceived these stressors as being more severe (p=0.027) when compared with male coaches. Coaches not planning to retire within the next 12 months reported less daily hassles (p=0.015) and less severe hassles (p=0.011) compared with those who were either contemplating or planning to retire within 12 months. Including both these variables in an adjusted regression model, associations with the total daily hassles score remained statistically significant. There were no significant associations between other demographic factors and the number or severity of daily life hassles.
Association of coach characteristics and life stress
There was a strong association between the total number and severity of daily hassles and depressive symptoms (p<0.001). These associations persisted after adjustment for retirement plans and family history of mood disorder, with an average of 7% increase in the odds of experiencing symptoms consistent with moderate or major depression for each additional daily hassle reported (OR=1.07, 95% CI 1.02 to 1.12, p=0.007).
Discussion
To our knowledge, this is the first study exploring the prevalence of depressive symptoms and daily hassles in coaches of elite athletes. The 14% prevalence of clinically relevant depressive symptoms we observed in this coach population is comparable to the rates of clinically diagnosed anxiety and depression in the New Zealand adult population,3 but lower than reported symptom rates among elite athletes based in New Zealand (21%)2 and Australia (20%).14 There may be a number of explanations for this difference. Compared with elite-level athletes, coaches are generally older. Ninety per cent of the coaches in this sample were older than 30 years of age, compared with 17% of athletes.2 Older adults have been shown to have a higher ‘sense of coherence’ and ‘self-esteem’ and lower overall rates of depression and distress.15 The observed difference could relate to a coaching selection bias. Among elite coaches, traits such as perseverance, optimism, hope and resilience are desirable and have been recognised as being important for helping them cope with stress.16 These personality traits may be protective and individuals who do not have them may be less likely to become elite coaches. In contrast, success in elite athletes is related to the so-called ‘big five trait dimensions’—openness, conscientiousness, extraversion, agreeableness and neuroticism.17 Finally, it is also possible that being an elite athlete is intrinsically more stressful than being an elite coach. This may be related to factors that are unique to elite sport where athletes generally have a short career, are always at risk of a career-ending injury and are directly responsible for their performance,18 when compared with coaches. Perhaps reflecting this, elite athletes report similar types of life stress, but more frequently, than coaches when given the same survey.2
As previously observed in elite athlete populations,2 19 we observed in coaches a positive association between clinically relevant depressive symptoms and retirement plans. The relatively small sample size is an important limitation of this study (largely due to the small number of elite-level coaches in New Zealand) and as a result statistical power and potential to perform subgroup analyses was limited. CIs for associations were wide for estimates comparing the odds of depressive symptoms and therefore the results from logistic regression in this study should therefore be interpreted cautiously.
High levels of daily hassles have been associated with moderate level of depressive symptoms in elite athletes,2 19 and a similar association was demonstrated in this coaching population. The understanding of the association between life stress levels and psychological disorders, especially in depression, is enlarging.20 It is, however, important to recognise that high level of life stress does not necessarily precede a depressive episode, with many other factors influencing.21 Improved understanding of these associations may allow those working within elite sport to identify the individuals at risk of experiencing depressive symptoms and help establish effective means of support.
Coaches provide a critical role, both in the athletes’ quest for success,22 and in the early identification, intervention and guidance for athletes at risk of depression.11 23 Chronically elevated stress levels can impact negatively on a coach’s well-being, which may in turn reduce the individual’s ability to best support athletes that they coach.24 25 Currently in New Zealand, there is no formal structure to support the mental health of most coaches of elite athletes. It is hoped that the data from this study will help direct strategies to better support this group. This may involve the provision of mental health education, monitoring well-being and the removal of barriers to seeking appropriate assistance. This research suggests that establishing support structures during periods of transition such as retirement and times of high life stress levels should be prioritised.
Conclusion
This is the first study to evaluate the prevalence of depressive symptoms in coaches of elite athletes. The current study has demonstrated that these coaches are affected by depressive symptoms, with a prevalence (14%) comparable to the general New Zealand adult population but lower than the elite athlete population. Elite coaches are also affected by similar types of life stress to elite athletes, and there was a significant association between the reported number of daily life hassles and depressive symptoms. We hope that this study will help raise awareness about mental health problems in the elite coaching community and lead to enhanced mental health support.
Acknowledgments
We thank the High Performance Sport New Zealand (HPSNZ) and New Zealand Football for their assistance with this research. Financial assistance was provided by HPSNZ for statistical analysis.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval was granted by the University of Auckland Human Ethics Committee (reference 020439).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.